Write in detail principles of hepatic resection . discuss the indication , classification and post op management of HEPATIC resection
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hepatic resection" AND "principles"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
I now have all the material needed to write a comprehensive, detailed answer. Here it is:
Hepatic Resection: Principles, Indications, Classification, and Postoperative Management
1. HISTORICAL BACKGROUND
Although liver resections were attempted in the late 1800s, the first true anatomic right hepatectomy is credited to Lortat-Jacob in 1952, marking the start of modern hepatic surgery. Early series from the 1970s-1980s reported mortality rates often exceeding 20% for major resections, largely due to massive intraoperative blood loss. Over the past three decades, three transformative advances have changed outcomes dramatically:
- Recognition that most intraoperative blood loss comes from the hepatic veins, prompting the routine use of low central venous pressure (CVP < 5 mmHg) technique
- An improved understanding of Couinaud's segmental anatomy of the liver
- Development of modern parenchymal transection devices and hemostatic agents
In experienced centers today, perioperative mortality is routinely ≤3-5%, with many centers reporting mortality approaching 1-2%.
2. SURGICAL ANATOMY - THE FOUNDATION OF HEPATIC SURGERY
Safe hepatic resection is impossible without detailed knowledge of liver anatomy. Couinaud's (1954) system divides the liver into 8 functionally independent segments (I-VIII), each with its own portal pedicle (hepatic artery branch + portal vein branch + bile duct) and its own hepatic venous drainage.
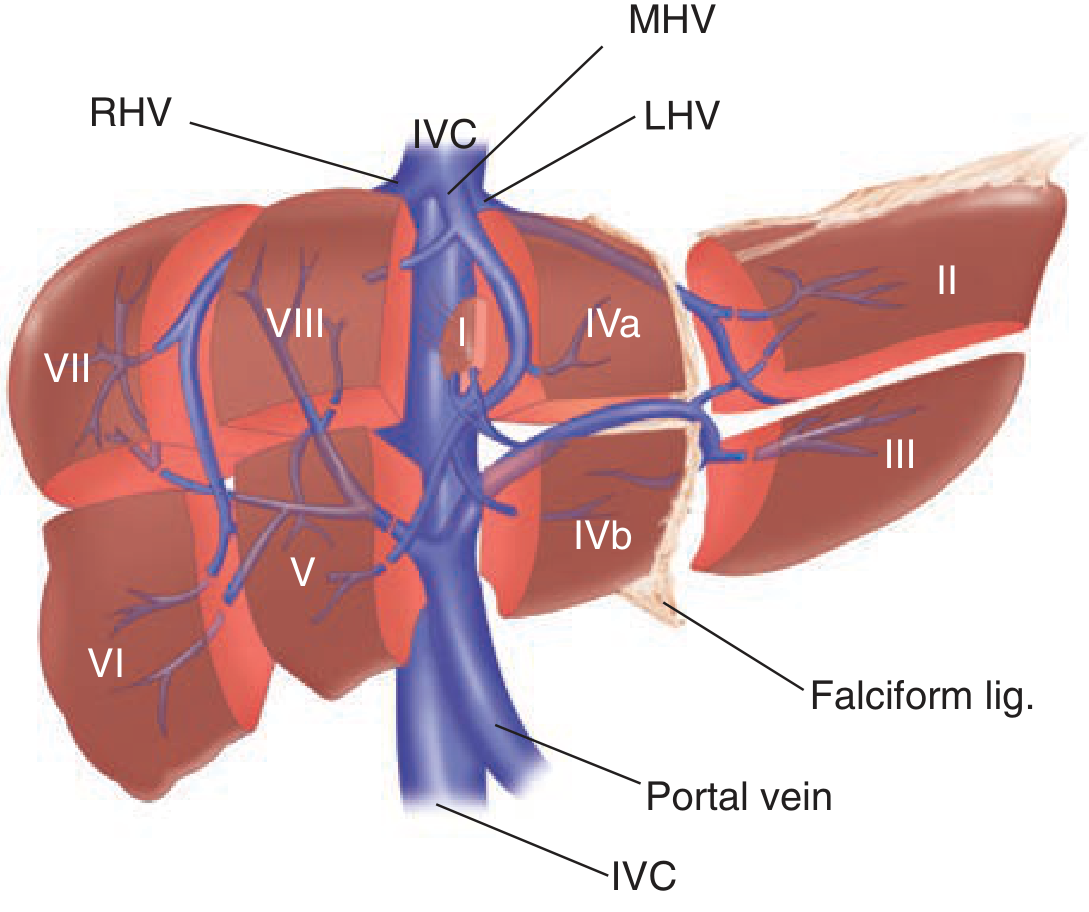
Hepatic anatomy: Couinaud segments I-VIII with hepatic veins and portal vein. Right liver = Segments V-VIII; Left liver = Segments II-IV; Caudate = Segment I. (Schwartz's Principles of Surgery, 11e)
Key anatomic landmarks:
- The principal plane (Cantlie's line) runs from the gallbladder fossa to the middle hepatic vein, dividing the liver into right and left hemilivers; it has no surface marking
- Three hepatic veins (right, middle, left) divide the liver into four sections
- The middle hepatic vein is the watershed between right and left hemilivers
- The falciform ligament marks the left intersegmental fissure between segments II/III and segment IV
- The umbilical fissure contains the pars umbilicalis of the left portal vein; branches to the left medial segment (IVa/IVb) run rightward from this structure, while branches to the left lateral segment (II and III) run leftward - critical orientation for safe left-sided resections
- In ~12% of patients, the right portal vein trifurcates directly (no proper RPV trunk), giving the appearance of a trifurcation at the porta hepatis
3. PRINCIPLES OF HEPATIC RESECTION
3.1 Preoperative Assessment and Patient Selection
Liver Function Reserve
The functional capacity of the liver is the single most important determinant of whether a patient can tolerate resection. Key parameters assessed include:
| Parameter | Normal liver | Cirrhotic liver |
|---|---|---|
| Max safe resection | Up to 80% | Much less (often 20-30%) |
| Child-Pugh A | Usually can resect | With caution, limited resection |
| Child-Pugh B/C | N/A | Contraindicated |
| Portal hypertension | N/A | Contraindicated |
- The future liver remnant (FLR) is the volume of functional liver that will remain after resection
- For a normal liver: FLR should be ≥20-25% of total liver volume
- For a liver with underlying disease (chemotherapy-associated steatohepatitis, fibrosis): FLR ≥30-40%
- For a cirrhotic liver: FLR ≥40%
- The risk of postoperative hepatic dysfunction is minimal if the reduction of functional liver parenchyma is less than 50%, but rises steeply when the FLR approaches 20-25%
Preoperative Functional Tests
- Indocyanine green (ICG) retention test at 15 minutes: normal is <10%; values >14% indicate compromised function
- Child-Pugh score: incorporates bilirubin, albumin, PT/INR, ascites, and encephalopathy
- MELD score: used in the context of cirrhosis
- CT volumetry: quantitative measurement of FLR volume
Strategies to Augment FLR (when FLR is inadequate)
Portal Vein Embolization (PVE)
- First described by Makuuchi et al. in 1984
- The portal supply to the hemiliver intended for resection is embolized percutaneously
- This induces atrophy of the embolized liver and compensatory hypertrophy of the FLR over ~4 weeks
- PVE increases the standardized FLR (sFLR) and provides a dynamic test of regenerative capacity
- The Kinetic Growth Rate (KGR) = (difference in sFLR before/after PVE) ÷ elapsed weeks; a KGR ≥ 2%/week is associated with 0% postoperative hepatic insufficiency
Liver Venous Deprivation (LVD)
- Simultaneous embolization of the portal vein AND hepatic vein(s) of the hemiliver to be resected
- Superior to PVE alone: induces 61% vs. 29% volume increase; reduced rate of postoperative liver failure
- Recommended when starting sFLR < 19% or in staged hepatectomy planning
Two-Stage Hepatectomy
- For bilateral liver metastases not safely removable in one operation
- Stage 1: clear the FLR (usually left liver) of disease
- PVE may be performed after stage 1 if needed
- Stage 2: major hepatectomy (usually right liver)
3.2 Operative Principles
A. Low Central Venous Pressure (CVP) Technique
- Most intraoperative blood loss originates from hepatic veins, not the portal system or hepatic arteries
- Maintaining CVP < 5 mmHg during parenchymal transection reduces back-bleeding from hepatic veins
- Achieved by: mild Trendelenburg position, fluid restriction, vasodilators (nitroglycerin, isoflurane), and active diuresis if necessary
- Volume is restored after the liver is removed and the cut surface secured
B. Vascular Inflow Control - The Pringle Manoeuvre
- First described by J.H. Pringle in 1908 (Notes on arrest of hepatic haemorrhage due to trauma, Ann Surg 1908)
- A vascular clamp or tourniquet is applied across the hepatoduodenal ligament, occluding the portal vein and hepatic artery simultaneously
- The normal liver tolerates up to 60 minutes of continuous ischemia
- In cirrhotic livers or to reduce ischemia-reperfusion injury: intermittent clamping with cycles of 15-20 minutes ON and 5 minutes OFF is preferred
- Total ischemic time should not exceed 120 minutes
C. Anatomic vs. Non-Anatomic Resection
- Anatomic (formal) resection: follows Couinaud's segmental planes, ligating the portal pedicle to that segment/section first. Provides the best oncologic margins for malignant disease.
- Non-anatomic (wedge) resection: removes tumor with a rim of normal liver without following segmental planes. Higher rates of margin involvement and disease recurrence for malignancy. Appropriate for benign disease where minimal normal liver sacrifice is desired.
- For colorectal liver metastases (CLM): parenchymal-sparing non-anatomic resection provides comparable oncologic outcomes with markedly fewer complications when compared to major anatomic resection, and is now preferred when feasible.
D. Parenchymal Transection Devices and Hemostasis
| Technique/Device | Mechanism |
|---|---|
| Finger fracture / blunt dissection + clips | Manual, oldest technique |
| CUSA (Cavitron Ultrasonic Surgical Aspirator) | Emulsifies liver parenchyma, spares vessels/ducts |
| Harmonic scalpel / LigaSure | Thermal energy coagulation and sealing |
| Hydro-Jet dissector | High-pressure water dissection |
| Argon beam coagulator | Surface coagulation of cut edge |
| Bipolar cautery + suture ligation | Fine vessel sealing |
| Endovascular staplers | Division of major hepatic/portal veins |
The guiding philosophy is that dividing liver tissue is a dissection requiring complete understanding of vascular anatomy, regardless of the instrument used.
E. Biliary Control
- Bile leaks occur in 10-20% of hepatectomies even without biliary reconstruction
- Individual identification and ligation of biliary radicals as they are encountered during parenchymal transection is essential
- A dilute hydrogen peroxide solution applied to the cut surface can highlight bile leaks (bubbling) at the end of resection
- Completion intraoperative cholangiography or biliary pressure test may be used in complex cases
F. Intraoperative Ultrasound
- Mandatory in modern hepatic surgery
- Identifies lesions not visible on preoperative imaging
- Confirms vascular anatomy in real time
- Guides the transection plane relative to major vessels
- Used to confirm completion: adequate remnant portal inflow, hepatic venous outflow, and absence of residual lesions
G. Liver Regeneration
- The liver has remarkable regenerative capacity: up to 80% of a normal non-cirrhotic liver can be resected, with functional compensation within weeks
- In cirrhotic livers, regenerative capacity is severely impaired, making even minor resections potentially catastrophic
4. INDICATIONS FOR HEPATIC RESECTION
4.1 Malignant Indications
Primary Liver Tumors
Hepatocellular Carcinoma (HCC)
- Hepatic resection is the gold standard and treatment of choice for HCC in patients with preserved liver function (Child-Pugh A, no clinically significant portal hypertension)
- In patients with Child-Pugh B/C cirrhosis, liver transplantation (meeting Milan criteria) is preferred over resection
- HCC is the leading indication for resection in Asia and Sub-Saharan Africa
- A 1-cm resection margin was historically considered necessary, but recent studies show comparable survival with narrower margins
Cholangiocarcinoma (CCA)
- Intrahepatic cholangiocarcinoma (iCCA): formal anatomic resection is preferred, often extended to include hilar nodes
- Perihilar cholangiocarcinoma (Klatskin tumor): requires resection of segments I, IV-VIII for right-sided tumors with caudate lobectomy; portal vein reconstruction may be required
- Distal CCA: managed by pancreaticoduodenectomy
Gallbladder cancer with hepatic invasion: requires en-bloc segments IVb and V resection with regional lymphadenectomy
Hepatic angiosarcoma, hepatoblastoma (pediatric): surgical resection is the backbone of treatment
Hepatic Metastases
Colorectal liver metastases (CLM) - the most common indication in Western centers
- Resection offers the only chance for cure with ~40% 5-year survival in carefully selected patients
- Criteria for resectability (modern, oncologic):
- Complete (R0) resection of all hepatic and extrahepatic disease must be achievable
- Adequate FLR must be preserved
- Absence of unresectable extrahepatic disease
- Previously: ≤4 metastases, unilobar disease - now largely abandoned; resectability is defined by what can be left, not what is removed
- Synchronous and staged resections are both acceptable; timing depends on the primary tumor presentation and extent of metastases
Non-colorectal, non-neuroendocrine metastases (breast, gastric, pancreatic): resection is selective; best results in controlled systemic disease, solitary metastasis
Neuroendocrine tumor liver metastases: resection provides excellent symptom control and prolonged survival; debulking ≥90% of disease is the target
4.2 Benign Indications
| Condition | Indication for resection |
|---|---|
| Symptomatic hepatic hemangioma | Large (>10 cm), symptomatic (pain, Kasabach-Merritt) |
| Hepatic adenoma | >5 cm, male sex, pregnancy, OCP use, rupture risk; all adenomas in men should be resected |
| Focal nodular hyperplasia (FNH) | Rare; only if symptomatic or diagnosis uncertain |
| Simple hepatic cysts | Only if large and symptomatic (usually fenestration preferred) |
| Polycystic liver disease | Fenestration/resection in selected symptomatic patients |
| Hydatid (Echinococcal) cyst | Pericystectomy, partial hepatectomy if needed; PAIR procedure for some |
| Liver abscess (pyogenic/amoebic) | Rarely; failure of percutaneous drainage, ruptured abscess |
| Caroli disease | Segmentectomy for localized disease; transplant if diffuse |
| Biliary cystadenoma/cystadenocarcinoma | Formal resection to prevent recurrence |
4.3 Contraindications to Hepatic Resection
Absolute contraindications:
- Child-Pugh B or C cirrhosis
- Clinically significant portal hypertension (varices, splenomegaly, thrombocytopenia < 100,000/µL)
- Unresectable extrahepatic metastatic disease
- Predicted FLR < 20% (normal liver), < 30% (diseased liver), < 40% (cirrhotic liver)
- Medically unfit for major surgery
Relative contraindications:
- Major vessel involvement (often overcome with reconstruction)
- Bilobar multifocal disease (overcome with staged resection + PVE)
- Prior liver resection (repeat hepatectomy possible in selected centers)
5. CLASSIFICATION OF HEPATIC RESECTIONS
5.1 Brisbane 2000 Nomenclature
The International Hepato-Pancreato-Biliary Association (IHPBA) consensus meeting in Brisbane, Australia in 2000 standardized terminology to enable universal communication. The terms below are based on Couinaud's segmental anatomy.
| Old Terminology | Brisbane 2000 Terminology | Segments Removed |
|---|---|---|
| Right hepatic lobectomy | Right hepatectomy / Right hemihepatectomy | V, VI, VII, VIII |
| Left hepatic lobectomy | Left hepatectomy / Left hemihepatectomy | II, III, IV |
| Right trisegmentectomy | Right trisectionectomy / Extended right hepatectomy | IV, V, VI, VII, VIII |
| Left trisegmentectomy | Left trisectionectomy / Extended left hepatectomy | II, III, IV, V, VIII |
| Left lateral segmentectomy | Left lateral sectionectomy / Bisegmentectomy | II, III |
| Right posterior lobectomy | Right posterior sectionectomy | VI, VII |
| Caudate lobectomy | Caudate lobectomy / Segmentectomy 1 | I |
The term "lobectomy" is discouraged because there are no external markings on the liver denoting a lobe. When in doubt, use numeric segment description (e.g., "bisegmentectomy II-III").
5.2 Classification by Extent
A. Major Hepatic Resections (≥3 Couinaud segments)
- Right hepatectomy (segments V-VIII): removes ~60% of liver volume
- Left hepatectomy (segments II-IV): removes ~40%
- Extended right hepatectomy / Right trisectionectomy (segments IV-VIII): removes ~80%
- Extended left hepatectomy / Left trisectionectomy (segments II, III, IV, V, VIII)
B. Minor Hepatic Resections (<3 segments)
- Bisegmentectomy (e.g., II+III = left lateral sectionectomy)
- Segmentectomy (single segment: e.g., seg VI, VII)
- Subsegmental / Wedge resection
C. Special Resections
- Caudate lobectomy (segment I): most complex; isolated between IVC and portal structures; required for hilar cholangiocarcinoma
- Central hepatectomy (segments IVa, IVb, V, VIII): preserves both right posterior and left lateral sections; used when tumor abuts both hepatic veins
- Ex vivo liver resection: liver removed, perfused on bench, lesion resected, then reimplanted; used for IVC involvement
5.3 Classification by Approach
Open hepatectomy: standard, best exposure for complex resections
Laparoscopic hepatectomy:
- Now performed by experienced surgeons for most types of resections including major hepatectomies
- Advantages: less blood loss, decreased morbidity, reduced postoperative pain, faster return of bowel function, shorter hospitalization (~50% reduction in LOS)
- Long-term oncologic outcomes for HCC and CLM are comparable to open surgery (propensity-score matched studies and meta-analyses)
- Learning curve: ~60 cases for minor resections; greater for laparoscopic major hepatectomy
- Pure laparoscopic, hand-assisted laparoscopic, and robotic approaches are all used
Robotic hepatectomy: emerging; advantages in complex dissections; adoption increasing globally
6. OPERATIVE STEPS: RIGHT HEPATECTOMY (Representative Procedure)
- Bilateral subcostal ("chevron") incision ± midline extension; fixed self-retaining retractor
- Laparotomy and systematic exclusion of extrahepatic disease
- Intraoperative ultrasound to confirm resectability and define transection plane
- Cholecystectomy (leaves cystic duct stump for traction)
- Divide right coronary and triangular ligaments; mobilize right lobe anteriorly and to the left
- Mobilize liver from anterior IVC in "piggyback" fashion; ligate short hepatic veins progressing cephalad to the right hepatic vein (RHV)
- Right hilar dissection: lower hilar plate; doubly ligate and divide right hepatic artery (confirm left hepatic artery pulsation before ligation); doubly ligate/divide the right portal vein (RPV) with a vascular stapler or between clamps
- A line of ischemic demarcation appears on the liver surface - this is the true right/left boundary
- Right hepatic duct is identified and ligated (usually during parenchymal transection to minimize bile duct injury)
- Dissect avascular tissue between RHV and middle hepatic vein (MHV) at the IVC; pass a silastic drain (the "liver-hanging manoeuvre" of Belghiti) through this gap
- Parenchymal transection along the principal plane (Cantlie's line), just to the right of the MHV unless the tumor extends over it, using CUSA/hydro-jet + Bovie + argon beam coagulator + suture ligation under Pringle manoeuvre
- As the RHV is encountered, divide between vascular clamps and suture ligate
- Inspect cut surface: figure-of-eight vascular sutures for bleeding points; clip/suture bile leaks; hydrogen peroxide test for occult bile leaks
- Completion intraoperative ultrasound: confirm left portal vein inflow and remaining hepatic venous outflow
- Suture falciform ligament to diaphragm to prevent rotation of remnant
- Tissue sealant to cut surface; closed suction drain in right subphrenic space
- Close abdomen
7. POSTOPERATIVE MANAGEMENT
7.1 Immediate Postoperative Care (ICU/HDU - First 24-48 Hours)
Monitoring:
- Continuous hemodynamic monitoring (arterial line, CVP)
- Urine output hourly
- Serum electrolytes, glucose, lactate, CBC every 4-6 hours
- Coagulation studies (PT/INR) - expect transient coagulopathy as the liver regains synthetic function
Fluid Management:
- Cautious fluid administration to avoid hepatic edema and ascites
- Albumin infusion (20-25%) to maintain serum albumin > 3 g/dL
- Avoid hypo-oncotic crystalloid overload
- Monitor for hypovolemia vs. interstitial sequestration
Liver Function Monitoring:
- Daily LFTs (bilirubin, AST/ALT, ALP, GGT)
- Daily coagulation studies (PT, INR, aPTT)
- Serum ammonia if encephalopathy suspected
- Glucose monitoring q4h (risk of hypoglycemia due to impaired glycogen storage)
7.2 Major Postoperative Complications and Management
A. Post-Hepatectomy Liver Failure (PHLF)
- Definition (ISGLS criteria): Impaired ability of the liver to maintain its synthetic, excretory, and detoxifying functions postoperatively, manifested as an elevated INR and bilirubin on or after postoperative day 5 (Grades A, B, C)
- Risk factors: Extensive resection, cirrhosis, excessive blood loss, prolonged ischemia, pre-existing steatohepatitis, chemotherapy-associated liver injury
- Prevention: Adequate FLR assessment, PVE when needed, low-CVP technique, limit ischemia time
- Management: Supportive care, nutritional support (enteral feeding), BCAA (branched-chain amino acids), fresh frozen plasma and vitamin K for coagulopathy, lactulose/rifaximin for encephalopathy; liver support systems (MARS) in refractory cases; transplantation in extreme cases
B. Bile Leak
- Occurs in 10-20% of major hepatectomies
- Presentation: drain output with elevated bilirubin (drain/serum bilirubin ratio > 3), fever, abdominal pain
- Management:
- Maintain drain; if no drain was placed, CT-guided percutaneous drainage of biloma
- ERCP with stenting/sphincterotomy to decompress biliary pressure (most effective)
- Repeat exploration for major ductal injury; hepatico-jejunostomy (Roux-en-Y) if needed
C. Bleeding and Coagulopathy
- Post-hepatectomy coagulopathy is expected (transient); INR often peaks on day 2-3
- Active hemorrhage: blood products, FFP, platelets, cryoprecipitate; correct hypothermia and acidosis
- Packing and re-exploration for ongoing surgical bleeding
- Angioembolization for arterial bleeding
- Hepatic artery pseudoaneurysm can cause delayed hemobilia (triad: GI bleed, jaundice, RUQ pain - Quincke's triad); diagnosed by CT angiography, treated by selective angioembolization
D. Pulmonary Complications
- Right pleural effusion: occurs in ~30-50% after right hepatectomy due to diaphragmatic lymphatic disruption
- Management: observation for small effusions; thoracocentesis for symptomatic large effusions
- Atelectasis and pneumonia: incentive spirometry, early mobilization, chest physiotherapy, analgesia (epidural or PCA for adequate respiratory effort)
E. Infectious Complications
- Intra-abdominal abscess: percutaneous CT-guided drainage; antibiotics
- Wound infection: wound care, antibiotics
- Biloma/infected biloma: drain and antibiotics
- Cholangitis: usually associated with biliary anastomosis or biliary obstruction; IV antibiotics + biliary drainage
F. Ascites
- Common after major hepatectomy, especially in cirrhotic patients
- Management: low-sodium diet, diuretics (spironolactone first-line, furosemide as add-on), large-volume paracentesis with albumin replacement if tense/symptomatic
G. Renal Failure
- Secondary to hepatorenal syndrome in PHLF, or direct nephrotoxicity (aminoglycosides, contrast)
- Prevention: maintain adequate circulating volume, avoid nephrotoxic drugs, N-acetylcysteine
- Management: early nephrology consult; renal replacement therapy (CVVH) if severe
7.3 Nutritional Support
- Early enteral nutrition within 24-48 hours is the standard of care
- Hepatectomy increases protein catabolism and impairs gluconeogenesis and glycogen storage
- High-protein diet (1.5-2 g/kg/day) to support liver regeneration and prevent muscle wasting
- Branched-chain amino acids (BCAA) supplementation: particularly in cirrhotic patients to support synthetic function and reduce encephalopathy risk
- Total parenteral nutrition (TPN) reserved for patients who cannot tolerate enteral feeding
- Adequate vitamin K replacement (10 mg IV/IM daily) to correct coagulopathy
7.4 Drain Management
- Jackson-Pratt or similar closed suction drain placed in the right subphrenic space
- Check drain fluid bilirubin on POD 1, 3, and 5 (ISGLS criteria)
- Early drain removal (POD 1-3) if drain bilirubin is low and no evidence of bile leak (reduces infectious complications)
- Late removal or conversion to bulb suction if bile leak identified
7.5 Thromboembolic Prophylaxis
- Paradox: patients are both coagulopathic (bleeding risk) and hypercoagulable (portal vein thrombosis risk, DVT)
- Mechanical prophylaxis (compression stockings, sequential compression devices) from day 0
- Pharmacological prophylaxis (LMWH) initiated once surgical hemostasis is confirmed (typically POD 1-2), balancing bleeding risk
- Portal vein thrombosis: early detection by Doppler ultrasound (routine POD 3-5); anticoagulation if found
7.6 Monitoring Liver Regeneration
- Liver begins regenerating within hours of resection; functional compensation takes weeks
- Peak hypertrophy of the remnant occurs by 4-6 weeks
- Serial LFTs: bilirubin normalizes within 5-10 days in uncomplicated major hepatectomy; INR normalizes within 7-14 days
- Cross-sectional imaging (CT volumetry) at 4-6 weeks to assess remnant hypertrophy if needed
7.7 Discharge Criteria and Long-Term Follow-up
- Typical hospital stay: 7-10 days for open major hepatectomy; 3-5 days for laparoscopic resection
- Discharge criteria: tolerating oral diet, pain controlled, afebrile, downtrending LFTs, no drain output concerns
- Oncologic follow-up (for malignant disease): tumor markers (CEA for CLM, AFP for HCC) + CT/MRI at 3-monthly intervals for the first 2 years, then 6-monthly
- Surveillance for de novo HCC in cirrhotic remnant: 6-monthly AFP + ultrasound
- Adjuvant chemotherapy for CLM (FOLFOX/CAPOX) - discussed at multidisciplinary team meeting
8. OUTCOMES SUMMARY
| Outcome | Benchmark |
|---|---|
| Operative mortality (experienced center) | 1-3% |
| Major morbidity | 20-45% |
| Blood transfusion rate | < 30% (modern era) |
| Bile leak rate | 10-20% |
| PHLF rate (Grade B/C) | 5-10% |
| 5-year survival, CLM (selected) | ~40% |
| 5-year survival, HCC (Child-Pugh A) | 50-70% |
| Hospital stay, open major hepatectomy | 7-10 days |
| Hospital stay, laparoscopic hepatectomy | 3-5 days |
Sources:
- Sabiston Textbook of Surgery, 21e - Principles of Hepatic Resection, Chapter 89-90, pp. 1905-1922
- Schwartz's Principles of Surgery, 11e - Hepatic Resection, Chapter 31, pp. 1407-1414
- Fischer's Mastery of Surgery, 8e - Chapters 172, 192 (Pringle Manoeuvre, Portal Anatomy)
- Bailey & Love's Short Practice of Surgery, 28e - Chapter 79
This is a shared conversation. Sign in to Orris to start your own chat.