
57317.jpg
ENT
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Now I have everything needed to write a thorough, exam-ready answer. Let me compile it:
Facial Nerve Palsy - Complete Case Analysis
Case Summary: This 35-year-old man with acute unilateral right-sided lower motor neuron (LMN) facial palsy - loss of forehead wrinkling, inability to close the eye, Bell's phenomenon, flattening of the nasolabial fold, deviation of mouth to left, no sensory loss, no limb weakness - is a classic presentation of Bell's palsy (idiopathic peripheral facial paralysis).
Learning Objective 1 - Anatomy and Functional Components of CN VII
The facial nerve (CN VII) innervates structures derived from Reichert's cartilage (2nd branchial arch). It has five fiber types:
| Fiber Type | Function |
|---|---|
| Special Visceral Efferent (SVE) | Motor supply to muscles of facial expression, stapedius, stylohyoid, posterior belly of digastric |
| General Visceral Efferent (GVE) | Parasympathetic supply to lacrimal gland (via GSPN), submandibular and sublingual glands (via chorda tympani) |
| Special Visceral Afferent (SVA) | Taste from anterior 2/3 of tongue (via chorda tympani), tonsillar fossae, and posterior palate (via GSPN) |
| General Somatic Afferent (GSA) | Sensation from EAC and conchal skin of auricle |
| Visceral Afferent | From mucosa of nose, pharynx, and palate |
Three brainstem nuclei:
- Motor nucleus - caudal pons (SVE)
- Superior salivatory nucleus - dorsal to motor nucleus (GVE)
- Nucleus of the solitary tract - medulla (SVA - taste)
Key point: The superior (rostral) part of the motor nucleus (innervating frontalis and orbicularis oculi) receives both crossed and uncrossed cortical input. The inferior (caudal) part receives only ipsilateral input - this is why UMN lesions spare the forehead.
Learning Objective 2 - Course of the Facial Nerve: Origin to Terminal Branches
The facial nerve has five intratemporal segments (traverses the fallopian canal):
Intracranial Segment (~24 mm)
- From the lateral pons to the porus of the internal auditory canal (IAC)
- Travels through the cerebellopontine angle (CPA)
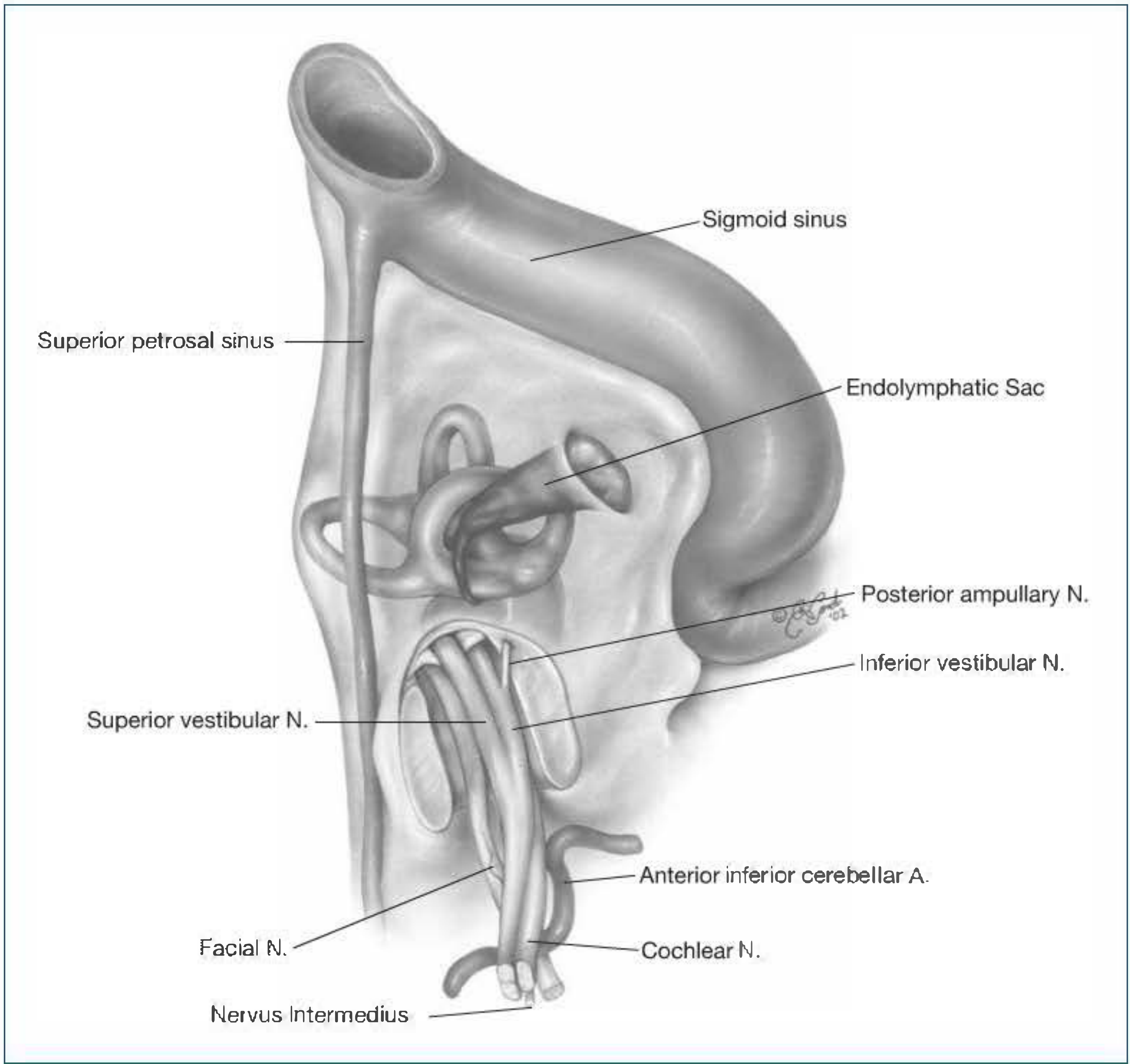
- Within the IAC, occupies the anterosuperior quadrant at the fundus (Bill's bar separates it from the superior vestibular nerve)
- Joined here by the nervus intermedius
Labyrinthine Segment (~4 mm)
- Shortest and narrowest segment
- From the fundus of the IAC to the geniculate ganglion
- Runs superior to the cochlea
- First genu (bend) occurs at the geniculate ganglion
- First branch: Greater Superficial Petrosal Nerve (GSPN) - parasympathetics to lacrimal gland
Tympanic (Horizontal) Segment (~13 mm)
- From geniculate ganglion to the pyramidal eminence
- Courses in the medial wall of the tympanic cavity
- Superior to the cochleariform process and oval window
- Second branch: Nerve to stapedius (in upper mastoid)
Mastoid (Vertical) Segment (~20 mm)
- From the second genu (at the lateral SCC / pyramidal eminence) to the stylomastoid foramen
- Third branch: Chorda tympani - taste from anterior 2/3 tongue + parasympathetics to submandibular/sublingual glands
Extratemporal Segment
- Exits the stylomastoid foramen
- Gives off: posterior auricular nerve, branch to posterior belly of digastric, branch to stylohyoid
- Enters the parotid gland where it divides at the pes anserinus into:
- Temporofacial trunk - temporal and zygomatic branches
- Cervicofacial trunk - buccal, marginal mandibular, and cervical branches
Mnemonic for terminal branches: "To Zanzibar By Motor Car" (Temporal, Zygomatic, Buccal, Marginal mandibular, Cervical)
Learning Objective 3 - Surgical Landmarks of the Facial Nerve
| Facial Nerve Segment | Surgical Landmark |
|---|---|
| Labyrinthine segment | Vertical crest (Bill's bar) in IAC; cochlea (superior) |
| Geniculate ganglion | Cochleariform process (medially); tegmen (superiorly); middle fossa dura |
| Tympanic segment | Cochleariform process anteriorly; oval window niche inferiorly; lateral SCC |
| Second genu | Just anteroinferior to the lateral semicircular canal; anterior to short process of incus |
| Mastoid segment | Posterior to digastric ridge; medial to tympanomastoid suture; lateral to jugular bulb |
| Stylomastoid foramen | Digastric ridge (tympanomastoid suture); tragal pointer (pointer of tragal cartilage ~1 cm anteromedial); posterior belly of digastric |
Extratemporal (parotid) landmarks:
- Tympanomastoid suture → stylomastoid foramen 6-8 mm deep
- Tragal pointer (main trunk is ~1 cm deep to apex of tragal cartilage)
- Posterior belly of digastric muscle
- Mastoid tip
Learning Objective 4 - Clinical Features of Facial Nerve Palsy
This patient demonstrates the classic LMN features:
Motor:
- Loss of forehead wrinkling (ipsilateral)
- Inability to close the eye completely (lagophthalmos)
- Bell's phenomenon - eye rolls upward and outward when patient attempts to close the eye (protective reflex)
- Flattening of the nasolabial fold
- Mouth deviates to the unaffected (contralateral) side on smiling
- Drooling from the ipsilateral angle of the mouth
- Inability to whistle, blow, puff cheeks
Autonomic (depending on level of lesion):
- Reduced tearing (if above GSPN)
- Hyperacusis (if stapedius branch affected)
- Reduced salivation / altered taste (if chorda tympani affected)
Sensory:
- Herpetic vesicles in EAC and conchal bowl (Ramsay Hunt syndrome if VZV)
House-Brackmann Grading Scale (used to grade severity):
- Grade I = Normal function
- Grade II = Slight dysfunction (slight forehead movement, complete eye closure with effort)
- Grade III = Moderate (some forehead movement, complete eye closure with effort)
- Grade IV = Moderately severe (no forehead movement, incomplete eye closure)
- Grade V = Severe (no movement, barely perceptible motion)
- Grade VI = Total paralysis
Learning Objective 5 - UMN vs. LMN Facial Palsy
This is the single most important clinical distinction:
| Feature | UMN Palsy (Supranuclear) | LMN Palsy (Infranuclear) |
|---|---|---|
| Forehead sparing | YES - forehead spared (bilateral cortical supply to upper face) | NO - forehead involved (all muscles affected) |
| Eye closure | Preserved (or only mildly affected) | Impaired - lagophthalmos |
| Bell's phenomenon | Absent | Present |
| Emotional movements | May be selectively preserved (emotional vs. volitional dissociation) | Both volitional and emotional affected equally |
| Taste, lacrimation, salivation | Normal | May be affected (depends on level) |
| Cause | Stroke, brain tumor, MS (contralateral hemisphere) | Bell's palsy, Ramsay Hunt, otitis media, parotid tumor, trauma |
| Associated findings | Contralateral limb weakness, hemiplegia | Isolated facial palsy possible |
| Side of weakness | Contralateral lower face to lesion | Ipsilateral entire face |
This patient's forehead involvement + Bell's phenomenon confirms LMN palsy.
The mechanism: The upper face (frontalis, orbicularis oculi) receives cortical input from both hemispheres (ipsilateral AND contralateral). So a unilateral cortical/UMN lesion still has innervation from the intact contralateral hemisphere - hence forehead is spared. The lower face receives predominantly contralateral unilateral cortical supply - so UMN lesions cause contralateral lower facial weakness.
Learning Objective 6 - Electrodiagnostic Tests
These tests determine prognosis and guide surgical decision-making in complete paralysis:
1. Nerve Excitability Test (NET)
- Simplest test (Laumans and Jonkees)
- Electrical stimulation over stylomastoid foramen - lowest current producing facial twitch compared bilaterally
- >3.5 mA difference between sides = severe degeneration → consider decompression
- Useful only in first 2-3 weeks of complete paralysis
- Limitations: subjective endpoint, observer-dependent
2. Maximal Stimulation Test (MST)
- Modification of NET using maximum current
- Compares movement between sides (equal, reduced, absent)
- More sensitive than NET
3. Electroneurography (ENoG / ENOG)
- Most objective electrical test
- Supramaximal stimulation at stylomastoid foramen; compound muscle action potential (CMAP) recorded from nasolabial fold
- Compares peak-to-peak amplitude of affected vs. normal side
- >90% degeneration on ENOG (within 2 weeks of onset) = poor prognosis, candidate for surgical decompression
- Most useful: begins 3 days after complete paralysis, repeated every 1-3 days
4. Electromyography (EMG)
- Detects fibrillation potentials (denervation, ~2-3 weeks after injury)
- Detects polyphasic reinnervation potentials (earliest sign of recovery - appears before clinical movement)
- Useful for long-term prognosis and detecting reinnervation
- Complements ENoG
5. Acoustic Reflex Testing (Stapedial Reflex)
- Tests integrity of the stapedius branch (distal to geniculate ganglion in mastoid segment)
- Absent reflex = lesion proximal to or at the stapedius branch
- Topodiagnostic significance
Learning Objective 7 - Causes of Facial Nerve Palsy
Idiopathic
- Bell's palsy (~75% of all cases) - likely HSV-1 reactivation
Infective
- Ramsay Hunt syndrome (herpes zoster oticus - VZV) - vesicles in EAC/concha, otalgia, sensorineural hearing loss
- Otitis media (acute or chronic)
- Malignant (necrotizing) otitis externa
- Mastoiditis
- HIV, Lyme disease (Borrelia burgdorferi), mumps, EBV
Traumatic
- Temporal bone fracture (transverse > longitudinal in causing facial palsy)
- Birth trauma (forceps delivery)
- Penetrating injuries
- Iatrogenic (surgery - parotid, mastoid, middle ear)
Neoplastic
- Primary facial nerve tumors (facial neuroma / schwannoma)
- Parotid gland malignancy
- Acoustic neuroma
- Glomus jugulare / tympanicum
- Metastatic disease
- Cholesteatoma
Neurological
- Stroke (UMN palsy - note: contralateral lower face)
- Multiple sclerosis
- Guillain-Barré syndrome (bilateral facial palsy)
- Möbius syndrome (congenital)
Metabolic / Systemic
- Diabetes mellitus
- Pregnancy (increased risk, especially with pre-eclampsia)
- Sarcoidosis (Heerfordt syndrome - uveoparotid fever)
Other
- Melkersson-Rosenthal syndrome (recurrent facial palsy + facial edema + fissured tongue)
Learning Objective 8 - Topodiagnostic Tests for Intratemporal Lesions
These tests localize the level of the lesion along the intratemporal course by testing branches given off sequentially:
| Test | Branch Tested | Level Assessed |
|---|---|---|
| Schirmer's Test (Lacrimation test) | Greater Superficial Petrosal Nerve (GSPN) | Proximal to / at geniculate ganglion (labyrinthine segment) |
| Stapedial Reflex (Acoustic reflex) | Nerve to stapedius | At / proximal to pyramidal eminence (tympanic-mastoid junction) |
| Taste testing (anterior 2/3 tongue) | Chorda tympani | At / proximal to mid-mastoid segment |
| Submandibular salivary flow (Salivary flow test) | Chorda tympani → submandibular ganglion | At / proximal to chorda tympani origin |
Interpretation:
Brainstem → Geniculate → Pyramidal → Chorda tympani → Stylomastoid → Parotid
ganglion eminence (mid-mastoid) foramen
↓ ↓ ↓
Schirmer Stapedial Taste test
(GSPN) reflex Salivary flow
- All tests abnormal → lesion at or proximal to geniculate ganglion (labyrinthine or more proximal)
- Schirmer normal, others abnormal → lesion between GSPN and stapedius branch (tympanic segment)
- Schirmer + Stapedius normal, taste abnormal → lesion between stapedius and chorda tympani origin (upper mastoid)
- All tests normal, only motor palsy → lesion at or distal to stylomastoid foramen (extratemporal)
Note: Schirmer's test - normal is >25 mm wetting in 5 minutes; <25 mm or >50% asymmetry = abnormal (reduced lacrimation = more proximal/severe lesion).
However, topodiagnostic testing has limitations due to variability and is less reliable for precise localization than initially hoped. Clinical interpretation must be integrated with imaging (MRI with gadolinium).
Learning Objective 9 - Management Plan for Facial Nerve Palsy
Acute Phase (Bell's Palsy)
1. Medical Treatment (mainstay):
- Corticosteroids (initiated within 72 hours, definitely within 2 weeks):
- Prednisolone 1 mg/kg/day (60-80 mg/day orally) for 10 days, then brief taper
- Improves rate and completeness of recovery
- Antiviral agents:
- Valacyclovir 500 mg TDS or acyclovir 400 mg 5x/day for 10 days
- Combined with steroids (combination may be superior to steroids alone)
- Gastroprotection: PPI or H2 blocker with steroids
- Monitor blood sugar (especially in diabetics on steroids)
2. Eye Care (critical - prevents corneal damage):
- Lubricating eye drops (artificial tears) during day
- Lubricating eye ointment at night
- Moisture chamber / taping of eyelid at night
- Dark glasses for outdoor use
- Regular ophthalmological review if incomplete closure persists
3. Physiotherapy:
- Facial exercises (mirror biofeedback)
- Gentle massage
4. Follow-up and Monitoring:
- Complete paralysis → obtain ENOG at day 3 of complete paralysis
- Repeat ENoG every 1-3 days
- If degeneration <90%: continue medical treatment
- If degeneration >90% (within 2 weeks of onset) + no voluntary EMG activity → surgical decompression candidate
5. Surgical Decompression (controversial, selected cases):
- Criteria: complete paralysis, >90% degeneration on ENoG within 2 weeks of onset
- Middle fossa approach (decompresses the labyrinthine segment and meatal foramen - the narrowest point)
Incomplete recovery / sequelae management:
- Synkinesis (aberrant regeneration) → botulinum toxin injections
- Persistent lagophthalmos → gold weight implant in upper eyelid, lateral tarsorrhaphy
- Persistent paralysis → facial reanimation surgery (nerve grafting, muscle transfer)
Learning Objective 10 - Complications of Facial Paralysis
| Complication | Mechanism | Management |
|---|---|---|
| Exposure keratitis / corneal ulceration | Lagophthalmos → corneal drying and abrasion | Eye care, lubricants, tarsorrhaphy |
| Synkinesis | Aberrant reinnervation (axons regrow to wrong muscles) | Botulinum toxin, physiotherapy |
| Hemifacial spasm | Abnormal ephaptic transmission after reinnervation | Botulinum toxin, microvascular decompression |
| Contracture | Fibrosis of denervated muscles | Physiotherapy, splinting |
| Crocodile tears (gustatory lacrimation) | Aberrant regeneration of salivary fibers → lacrimal gland | Common after Bell's palsy recovery; botulinum toxin |
| Psychological disturbance | Body image, communication difficulty | Counseling, support groups |
| Ectropion | Sagging of lower eyelid | Surgical correction |
| Dysarthria and dysphagia | Buccinator and orbicularis dysfunction | Speech therapy |
Back to the Case - Diagnosis and Approach
Diagnosis: Bell's Palsy (LMN Facial Nerve Palsy, Right Side)
Confirmatory features:
- Acute onset, complete unilateral LMN palsy (forehead involved - rules out UMN)
- Bell's phenomenon present
- No sensory deficit, no limb weakness (rules out stroke/central cause)
- No vesicles described (rules out Ramsay Hunt)
- Young male, otherwise healthy
Minimum Diagnostic Criteria (Taverner):
- ✅ Paralysis/paresis of all muscle groups of one side
- ✅ Sudden onset
- ✅ Absence of CNS disease signs
- ✅ Absence of ear or CPA disease signs
Investigations to exclude other causes: MRI with gadolinium enhancement of facial nerve, audiometry, blood glucose, Lyme serology, CBC.
Treatment:
- Prednisolone 60 mg/day × 10 days (taper over days 11-14)
- Valacyclovir 500 mg TDS × 10 days
- Lubricant eye drops + night-time eye ointment
- ENoG if progresses to complete paralysis (at day 3 of complete palsy)
Prognosis: ~85% recover completely within 3-6 weeks to 6 months. ~15% have incomplete recovery with risk of synkinesis, contracture, or crocodile tears.
Sources: Shambaugh Surgery of the Ear, p. 68-71 (anatomy/course); Cummings Otolaryngology Head and Neck Surgery (electrodiagnostic tests, surgical landmarks, Bell's palsy management); Bradley and Daroff's Neurology in Clinical Practice (UMN vs. LMN, clinical features); Shambaugh Surgery of the Ear, p. 650-651 (Bell's palsy pathophysiology and management)
Make pdf
Reading File
Running Command
ls /home/daytona/workspace/ 2>/dev/null || mkdir -p /home/daytona/workspace
Running Command
mkdir -p /home/daytona/workspace/facial-nerve-palsy && python3 -c "import reportlab; print('reportlab ok')" && python3 -c "import weasyprint; print('weasyprint ok')" 2>&1 || true
Writing File
~/facial-nerve-palsy/generate_pdf.py
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.units import mm
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, KeepTogether
)
from reportlab.lib.enums import TA_LEFT, TA_CENTER, TA_JUSTIFY
from reportlab.pdfbase import pdfmetrics
from reportlab.pdfbase.ttfonts import TTFont
OUTPUT = "/home/daytona/workspace/facial-nerve-palsy/Facial_Nerve_Palsy_ENT.pdf"
doc = SimpleDocTemplate(
OUTPUT,
pagesize=A4,
leftMargin=20*mm, rightMargin=20*mm,
topMargin=18*mm, bottomMargin=18*mm,
title="Facial Nerve Palsy – ENT Case Study",
author="Orris Medical AI"
)
W, H = A4
styles = getSampleStyleSheet()
# ── Custom styles ──────────────────────────────────────────────────────────
NAVY = colors.HexColor("#1a3355")
TEAL = colors.HexColor("#00796b")
LTBLUE = colors.HexColor("#e3f0fa")
LTGRN = colors.HexColor("#e8f5e9")
LTYEL = colors.HexColor("#fffde7")
HEADER_BG = colors.HexColor("#1a3355")
ALT1 = colors.HexColor("#f0f4f8")
ALT2 = colors.white
def style(name, **kw):
s = ParagraphStyle(name, **kw)
return s
title_style = style("MyTitle",
fontName="Helvetica-Bold", fontSize=20, textColor=colors.white,
alignment=TA_CENTER, leading=26, spaceAfter=4)
subtitle_style = style("MySubtitle",
fontName="Helvetica", fontSize=11, textColor=colors.HexColor("#b0c4de"),
alignment=TA_CENTER, leading=14, spaceAfter=2)
h1 = style("H1",
fontName="Helvetica-Bold", fontSize=13, textColor=colors.white,
backColor=NAVY, alignment=TA_LEFT, leading=18,
spaceBefore=10, spaceAfter=6,
leftIndent=4, rightIndent=4,
borderPad=4)
h2 = style("H2",
fontName="Helvetica-Bold", fontSize=11, textColor=TEAL,
leading=15, spaceBefore=8, spaceAfter=4, leftIndent=0)
h3 = style("H3",
fontName="Helvetica-BoldOblique", fontSize=10, textColor=NAVY,
leading=14, spaceBefore=5, spaceAfter=3, leftIndent=6)
body = style("Body",
fontName="Helvetica", fontSize=9.5, textColor=colors.HexColor("#222222"),
leading=14, spaceAfter=4, alignment=TA_JUSTIFY, leftIndent=4)
bullet = style("Bullet",
fontName="Helvetica", fontSize=9.5, textColor=colors.HexColor("#222222"),
leading=13, spaceAfter=2, leftIndent=14, firstLineIndent=-10)
bold_body = style("BoldBody",
fontName="Helvetica-Bold", fontSize=9.5, textColor=NAVY,
leading=13, spaceAfter=2, leftIndent=4)
caption = style("Caption",
fontName="Helvetica-Oblique", fontSize=8.5, textColor=colors.HexColor("#555555"),
alignment=TA_CENTER, leading=11, spaceAfter=4)
case_style = style("Case",
fontName="Helvetica", fontSize=9.5, textColor=colors.HexColor("#1a1a1a"),
backColor=LTBLUE, leading=14, spaceAfter=3, alignment=TA_JUSTIFY,
leftIndent=8, rightIndent=8, borderPad=6)
note_style = style("Note",
fontName="Helvetica-Oblique", fontSize=8.5, textColor=colors.HexColor("#444444"),
backColor=LTYEL, leading=12, spaceAfter=3, leftIndent=6, rightIndent=6)
def tbl(data, col_widths, hdr_rows=1, alt_rows=True, hdr_bg=NAVY, hdr_fg=colors.white):
ts = [
('BACKGROUND', (0,0), (-1, hdr_rows-1), hdr_bg),
('TEXTCOLOR', (0,0), (-1, hdr_rows-1), hdr_fg),
('FONTNAME', (0,0), (-1, hdr_rows-1), 'Helvetica-Bold'),
('FONTSIZE', (0,0), (-1,-1), 9),
('LEADING', (0,0), (-1,-1), 12),
('VALIGN', (0,0), (-1,-1), 'TOP'),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING',(0,0),(-1,-1), 4),
('LEFTPADDING',(0,0), (-1,-1), 6),
('RIGHTPADDING',(0,0),(-1,-1), 6),
('GRID', (0,0), (-1,-1), 0.4, colors.HexColor("#aaaaaa")),
('ROWBACKGROUNDS', (0, hdr_rows), (-1,-1), [ALT1, ALT2] if alt_rows else [ALT2]),
]
t = Table(data, colWidths=col_widths, repeatRows=hdr_rows)
t.setStyle(TableStyle(ts))
return t
def wrap(text, sty):
return Paragraph(text, sty)
def b(text): return f"<b>{text}</b>"
def i(text): return f"<i>{text}</i>"
story = []
# ═══════════════════════════════════════════════════════════════
# COVER BANNER
# ═══════════════════════════════════════════════════════════════
banner_data = [[Paragraph("FACIAL NERVE PALSY", title_style)],
[Paragraph("ENT Case Study & Complete Learning Guide", subtitle_style)],
[Paragraph("Based on: Cummings Otolaryngology · Shambaugh Surgery of the Ear · Bradley & Daroff's Neurology", subtitle_style)]]
banner_tbl = Table(banner_data, colWidths=[170*mm])
banner_tbl.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), NAVY),
('TOPPADDING', (0,0), (-1,-1), 8),
('BOTTOMPADDING', (0,0), (-1,-1), 8),
('LEFTPADDING', (0,0), (-1,-1), 10),
('RIGHTPADDING', (0,0), (-1,-1), 10),
('ROUNDEDCORNERS', [6]),
]))
story.append(banner_tbl)
story.append(Spacer(1, 8*mm))
# ═══════════════════════════════════════════════════════════════
# CLINICAL CASE
# ═══════════════════════════════════════════════════════════════
story.append(Paragraph("CLINICAL CASE PRESENTATION", h1))
story.append(Spacer(1, 2*mm))
case_box = Table([[Paragraph(
"A <b>35-year-old man</b> presents to ENT OPD with <b>sudden onset weakness of the right side of his face</b> "
"since yesterday morning. He complains of difficulty closing his right eye, drooling of saliva from the right "
"corner of his mouth, and inability to smile properly. He denies limb weakness, headache, loss of "
"consciousness, or recent trauma.",
case_style)]], colWidths=[170*mm])
case_box.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), LTBLUE),
('BOX', (0,0), (-1,-1), 1.5, TEAL),
('TOPPADDING', (0,0), (-1,-1), 8),
('BOTTOMPADDING', (0,0), (-1,-1), 8),
('LEFTPADDING', (0,0), (-1,-1), 10),
('RIGHTPADDING', (0,0), (-1,-1), 10),
]))
story.append(case_box)
story.append(Spacer(1, 4*mm))
story.append(Paragraph(b("On Examination:"), bold_body))
exam_data = [
[wrap(b("Finding"), bold_body), wrap(b("Detail"), bold_body)],
[wrap("Forehead wrinkling", body), wrap("Lost on the right side", body)],
[wrap("Eye closure", body), wrap("Cannot close right eye completely (lagophthalmos)", body)],
[wrap("Nasolabial fold", body), wrap("Flattened on the right", body)],
[wrap("Mouth on smiling", body), wrap("Deviates to the left (unaffected side)", body)],
[wrap("Bell's phenomenon", body), wrap("Present (eye rolls up and out on attempted closure)", body)],
[wrap("Sensory deficits", body), wrap("None", body)],
[wrap("Limb power/reflexes", body), wrap("Normal bilaterally", body)],
]
story.append(tbl(exam_data, [60*mm, 110*mm]))
story.append(Spacer(1, 3*mm))
story.append(Paragraph(
"⚡ <b>Diagnosis: Bell's Palsy</b> – Right-sided LMN facial palsy (forehead involved + Bell's phenomenon "
"confirms peripheral/infranuclear lesion).",
style("Diag", fontName="Helvetica-Bold", fontSize=10, textColor=colors.HexColor("#ffffff"),
backColor=TEAL, leading=14, spaceAfter=4, leftIndent=6, rightIndent=6, borderPad=5)))
story.append(Spacer(1, 6*mm))
# ═══════════════════════════════════════════════════════════════
# LO 1 – ANATOMY & FUNCTIONAL COMPONENTS
# ═══════════════════════════════════════════════════════════════
story.append(Paragraph("LO 1 – ANATOMY & FUNCTIONAL COMPONENTS OF CN VII", h1))
story.append(Paragraph(
"The facial nerve (CN VII) innervates structures derived from <b>Reichert's cartilage (2nd branchial arch)</b>. "
"Three brainstem nuclei give rise to its fibres:", body))
story.append(Paragraph("• <b>Motor nucleus</b> – caudal pons (SVE)", bullet))
story.append(Paragraph("• <b>Superior salivatory nucleus</b> – dorsal to motor nucleus (GVE)", bullet))
story.append(Paragraph("• <b>Nucleus of the solitary tract</b> – medulla (SVA – taste)", bullet))
story.append(Spacer(1, 3*mm))
story.append(Paragraph(b("Five Fibre Types:"), h2))
ft_data = [
[wrap(b("Fibre Type"), bold_body), wrap(b("Abbreviation"), bold_body), wrap(b("Function"), bold_body)],
[wrap("Special Visceral Efferent", body), wrap("SVE", body),
wrap("Motor to muscles of facial expression, stapedius, stylohyoid, posterior belly of digastric", body)],
[wrap("General Visceral Efferent", body), wrap("GVE", body),
wrap("Parasympathetic to lacrimal gland (via GSPN), submandibular & sublingual glands (via chorda tympani)", body)],
[wrap("Special Visceral Afferent", body), wrap("SVA", body),
wrap("Taste from anterior 2/3 tongue (chorda tympani), tonsillar fossae & palate (GSPN)", body)],
[wrap("General Somatic Afferent", body), wrap("GSA", body),
wrap("Sensation from EAC and conchal skin of auricle", body)],
[wrap("Visceral Afferent", body), wrap("VA", body),
wrap("Mucosa of nose, pharynx, and palate", body)],
]
story.append(tbl(ft_data, [55*mm, 25*mm, 90*mm]))
story.append(Spacer(1, 3*mm))
story.append(Paragraph(
"<b>Key fact:</b> The <b>superior (rostral) motor nucleus</b> (innervating frontalis & orbicularis oculi) "
"receives <b>bilateral cortical input</b> (crossed + uncrossed). The <b>inferior (caudal) motor nucleus</b> "
"(lower face) receives <b>only contralateral/unilateral</b> input — explaining why UMN lesions spare the forehead.",
note_style))
story.append(Spacer(1, 6*mm))
# ═══════════════════════════════════════════════════════════════
# LO 2 – COURSE OF THE NERVE
# ═══════════════════════════════════════════════════════════════
story.append(Paragraph("LO 2 – COURSE OF THE FACIAL NERVE: ORIGIN TO TERMINAL BRANCHES", h1))
story.append(Paragraph(b("Five Intratemporal Segments (Fallopian Canal):"), h2))
seg_data = [
[wrap(b("Segment"), bold_body), wrap(b("Length"), bold_body),
wrap(b("Course & Key Relations"), bold_body), wrap(b("Branch Given Off"), bold_body)],
[wrap("1. Intracranial", body), wrap("~24 mm", body),
wrap("Lateral pons → porus of IAC; traverses CPA; anterosuperior quadrant at fundus (Bill's bar)", body),
wrap("Nervus intermedius joins here", body)],
[wrap("2. Labyrinthine", body), wrap("~4 mm (shortest & narrowest)", body),
wrap("Fundus of IAC → geniculate ganglion; superior to cochlea; meatal foramen is narrowest point (0.68 mm)", body),
wrap("Greater Superficial Petrosal Nerve (GSPN) – lacrimal gland", body)],
[wrap("3. Tympanic (Horizontal)", body), wrap("~13 mm", body),
wrap("1st genu (geniculate ganglion) → 2nd genu (pyramidal eminence); medial wall of tympanic cavity; "
"superior to cochleariform process & oval window", body),
wrap("Nerve to stapedius", body)],
[wrap("4. Mastoid (Vertical)", body), wrap("~20 mm", body),
wrap("2nd genu at lateral SCC → stylomastoid foramen; anteroinferior to lateral SCC", body),
wrap("Chorda tympani (taste anterior 2/3 tongue + salivary parasympathetics)", body)],
[wrap("5. Extratemporal", body), wrap("Variable", body),
wrap("Exits stylomastoid foramen → posterior auricular nerve → digastric/stylohyoid branches → "
"parotid gland → pes anserinus → terminal branches", body),
wrap("Temporal, Zygomatic, Buccal, Marginal mandibular, Cervical\n"
"Mnemonic: "To Zanzibar By Motor Car"", body)],
]
story.append(tbl(seg_data, [38*mm, 22*mm, 66*mm, 44*mm]))
story.append(Spacer(1, 6*mm))
# ═══════════════════════════════════════════════════════════════
# LO 3 – SURGICAL LANDMARKS
# ═══════════════════════════════════════════════════════════════
story.append(Paragraph("LO 3 – SURGICAL LANDMARKS OF THE FACIAL NERVE", h1))
sl_data = [
[wrap(b("Segment"), bold_body), wrap(b("Surgical Landmark(s)"), bold_body)],
[wrap("Labyrinthine / IAC", body),
wrap("Vertical crest (Bill's bar) separates facial nerve from superior vestibular nerve at fundus", body)],
[wrap("Geniculate ganglion", body),
wrap("Cochleariform process (medial); tegmen (superior); middle fossa dura (superior)", body)],
[wrap("Tympanic segment", body),
wrap("Cochleariform process (anteriorly); oval window niche (inferiorly); lateral SCC (posteriorly)", body)],
[wrap("2nd genu", body),
wrap("Just anteroinferior to lateral semicircular canal; anterior to short process of incus", body)],
[wrap("Mastoid segment", body),
wrap("Posterior to digastric ridge; medial to tympanomastoid suture; lateral to jugular bulb", body)],
[wrap("Stylomastoid foramen", body),
wrap("Digastric ridge (tympanomastoid suture); Tragal pointer (~1 cm anteromedial to tip); posterior belly of digastric", body)],
[wrap("Extratemporal / parotid", body),
wrap("Tympanomastoid suture → foramen 6–8 mm deep; tragal pointer; mastoid tip; posterior belly of digastric", body)],
]
story.append(tbl(sl_data, [45*mm, 125*mm]))
story.append(Spacer(1, 6*mm))
# ═══════════════════════════════════════════════════════════════
# LO 4 – CLINICAL FEATURES
# ═══════════════════════════════════════════════════════════════
story.append(Paragraph("LO 4 – CLINICAL FEATURES OF FACIAL NERVE PALSY", h1))
story.append(Paragraph(b("Motor Features (LMN):"), h2))
for f in [
"<b>Loss of forehead wrinkling</b> – ipsilateral (entire face affected in LMN)",
"<b>Lagophthalmos</b> – inability to close eye completely; widened palpebral fissure",
"<b>Bell's phenomenon</b> – eye rolls upward and laterally on attempted closure (protective reflex)",
"<b>Flattening of nasolabial fold</b> on affected side",
"<b>Deviation of mouth</b> to unaffected side on smiling (contralateral pull)",
"Drooling from ipsilateral angle of mouth",
"Inability to whistle, blow, or puff cheeks",
]:
story.append(Paragraph(f"• {f}", bullet))
story.append(Spacer(1, 3*mm))
story.append(Paragraph(b("Autonomic Features (depending on level of lesion):"), h2))
for f in [
"Reduced tearing (lesion proximal to GSPN – labyrinthine segment or above)",
"Hyperacusis – reduced stapedius function (lesion proximal to pyramidal eminence)",
"Reduced salivation + altered taste (lesion proximal to chorda tympani in mastoid segment)",
"Herpetic vesicles in EAC / concha → Ramsay Hunt syndrome (VZV aetiology)",
]:
story.append(Paragraph(f"• {f}", bullet))
story.append(Spacer(1, 3*mm))
story.append(Paragraph(b("House-Brackmann Grading Scale:"), h2))
hb_data = [
[wrap(b("Grade"), bold_body), wrap(b("Description"), bold_body), wrap(b("Features"), bold_body)],
[wrap("I", body), wrap("Normal", body), wrap("Normal function all areas", body)],
[wrap("II", body), wrap("Slight dysfunction", body),
wrap("Slight forehead movement; complete eye closure with minimal effort; slight asymmetry at rest", body)],
[wrap("III", body), wrap("Moderate dysfunction", body),
wrap("Some forehead movement; complete eye closure with effort; obvious weakness; no synkinesis", body)],
[wrap("IV", body), wrap("Moderately severe", body),
wrap("No forehead movement; incomplete eye closure; obvious disfiguring asymmetry", body)],
[wrap("V", body), wrap("Severe dysfunction", body),
wrap("Barely perceptible motion; asymmetry at rest", body)],
[wrap("VI", body), wrap("Total paralysis", body),
wrap("No movement at all", body)],
]
story.append(tbl(hb_data, [15*mm, 40*mm, 115*mm]))
story.append(Spacer(1, 6*mm))
# ═══════════════════════════════════════════════════════════════
# LO 5 – UMN vs LMN
# ═══════════════════════════════════════════════════════════════
story.append(Paragraph("LO 5 – UMN vs. LMN FACIAL PALSY", h1))
story.append(Paragraph(
"The <b>single most important clinical distinction</b> in facial palsy. Determined by whether the "
"<b>forehead is spared or involved</b>.", body))
story.append(Spacer(1, 2*mm))
ul_data = [
[wrap(b("Feature"), bold_body), wrap(b("UMN (Supranuclear)"), bold_body),
wrap(b("LMN (Infranuclear)"), bold_body)],
[wrap("Forehead sparing", body),
wrap("✅ YES – forehead SPARED (bilateral cortical supply to upper face nucleus)", body),
wrap("❌ NO – forehead INVOLVED (all branches of facial nerve affected)", body)],
[wrap("Eye closure", body),
wrap("Preserved or mildly affected", body),
wrap("Impaired – lagophthalmos present", body)],
[wrap("Bell's phenomenon", body),
wrap("Absent", body),
wrap("Present", body)],
[wrap("Emotional vs volitional", body),
wrap("Dissociation possible: emotional movements preserved", body),
wrap("Both equally affected", body)],
[wrap("Taste / lacrimation", body),
wrap("Normal", body),
wrap("May be affected (level-dependent)", body)],
[wrap("Side of weakness", body),
wrap("Contralateral lower face to hemisphere lesion", body),
wrap("Ipsilateral entire face", body)],
[wrap("Associated CNS signs", body),
wrap("Often: contralateral limb weakness, aphasia, gaze palsy", body),
wrap("Isolated facial palsy usual; no limb signs", body)],
[wrap("Common causes", body),
wrap("Stroke, brain tumour, MS (contralateral hemisphere)", body),
wrap("Bell's palsy, Ramsay Hunt, AOM, parotid tumour, trauma", body)],
]
story.append(tbl(ul_data, [38*mm, 66*mm, 66*mm]))
story.append(Spacer(1, 3*mm))
story.append(Paragraph(
"<b>Mechanism:</b> The upper face (frontalis, orbicularis oculi) motor nucleus receives <b>bilateral</b> "
"cortical input. A unilateral cortical (UMN) lesion still has intact input from the contralateral "
"hemisphere — so the forehead is spared. The lower face motor nucleus has predominantly <b>unilateral "
"contralateral</b> cortical supply — so UMN lesions cause contralateral lower facial weakness only.",
note_style))
story.append(Spacer(1, 6*mm))
# ═══════════════════════════════════════════════════════════════
# LO 6 – ELECTRODIAGNOSTIC TESTS
# ═══════════════════════════════════════════════════════════════
story.append(Paragraph("LO 6 – ELECTRODIAGNOSTIC TESTS", h1))
story.append(Paragraph(
"Used to determine <b>prognosis</b> and guide surgical decision-making. All tests are useful only in "
"<b>complete paralysis</b>; unnecessary in incomplete palsy (prognosis always good).", body))
story.append(Spacer(1, 2*mm))
ed_data = [
[wrap(b("Test"), bold_body), wrap(b("Principle"), bold_body),
wrap(b("Significant Result"), bold_body), wrap(b("Notes"), bold_body)],
[wrap("1. Nerve Excitability Test (NET)", body),
wrap("Minimal current to produce visible facial twitch; compare both sides over stylomastoid foramen", body),
wrap(">3.5 mA difference = severe degeneration", body),
wrap("Useful first 2–3 weeks only; subjective endpoint", body)],
[wrap("2. Maximal Stimulation Test (MST)", body),
wrap("Uses maximal current; compares movement response (equal / reduced / absent)", body),
wrap("Absent = total degeneration", body),
wrap("More sensitive than NET; simple", body)],
[wrap("3. Electroneurography (ENoG / ENOG)", body),
wrap("Supramaximal stimulation at stylomastoid foramen; CMAP amplitude compared bilaterally", body),
wrap(">90% degeneration vs. normal side = poor prognosis → consider decompression", body),
wrap("Most objective test; begin 3 days after complete paralysis; repeat every 1–3 days", body)],
[wrap("4. Electromyography (EMG)", body),
wrap("Detects spontaneous electrical activity in facial muscles", body),
wrap("Fibrillation potentials = denervation (2–3 wks); Polyphasic potentials = early reinnervation", body),
wrap("Detects reinnervation before clinical movement returns; useful long-term", body)],
[wrap("5. Stapedial / Acoustic Reflex", body),
wrap("Tests stapedius branch integrity", body),
wrap("Absent = lesion at or proximal to stapedius branch", body),
wrap("Topodiagnostic significance; quick and non-invasive", body)],
]
story.append(tbl(ed_data, [38*mm, 46*mm, 46*mm, 40*mm]))
story.append(Spacer(1, 6*mm))
# ═══════════════════════════════════════════════════════════════
# LO 7 – CAUSES
# ═══════════════════════════════════════════════════════════════
story.append(Paragraph("LO 7 – CAUSES OF FACIAL NERVE PALSY", h1))
causes_data = [
[wrap(b("Category"), bold_body), wrap(b("Causes"), bold_body)],
[wrap("Idiopathic (~75%)", body),
wrap("Bell's palsy (HSV-1 reactivation most likely; diagnosis of exclusion)", body)],
[wrap("Infective", body),
wrap("Ramsay Hunt syndrome (VZV – vesicles in EAC, otalgia, SNHL); Acute/chronic otitis media; "
"Malignant otitis externa; Mastoiditis; Lyme disease (Borrelia); HIV; EBV; Mumps", body)],
[wrap("Traumatic", body),
wrap("Temporal bone fracture (transverse > longitudinal for palsy); Birth trauma (forceps); "
"Penetrating injuries; Iatrogenic (parotidectomy, mastoidectomy, middle ear surgery)", body)],
[wrap("Neoplastic", body),
wrap("Facial nerve schwannoma/neuroma; Parotid malignancy; Acoustic neuroma; "
"Glomus jugulare/tympanicum; Cholesteatoma; Metastatic disease", body)],
[wrap("Neurological", body),
wrap("Stroke (UMN – contralateral lower face); Multiple sclerosis; "
"Guillain-Barré (bilateral facial palsy); Möbius syndrome (congenital)", body)],
[wrap("Metabolic / Systemic", body),
wrap("Diabetes mellitus; Pregnancy + pre-eclampsia; "
"Sarcoidosis (Heerfordt syndrome – uveoparotid fever)", body)],
[wrap("Other", body),
wrap("Melkersson-Rosenthal syndrome (recurrent palsy + facial oedema + fissured tongue); "
"Amyloidosis; Wegener's granulomatosis", body)],
]
story.append(tbl(causes_data, [38*mm, 132*mm]))
story.append(Spacer(1, 6*mm))
# ═══════════════════════════════════════════════════════════════
# LO 8 – TOPODIAGNOSTIC TESTS
# ═══════════════════════════════════════════════════════════════
story.append(Paragraph("LO 8 – TOPODIAGNOSTIC TESTS FOR INTRATEMPORAL LESIONS", h1))
story.append(Paragraph(
"These tests localise the level of lesion along the intratemporal facial nerve by sequentially testing "
"branches given off at specific anatomical levels.", body))
story.append(Spacer(1, 3*mm))
topo_data = [
[wrap(b("Test"), bold_body), wrap(b("Branch Tested"), bold_body),
wrap(b("Level Assessed"), bold_body), wrap(b("Method"), bold_body)],
[wrap("Schirmer's Test (Lacrimation)", body),
wrap("Greater Superficial Petrosal Nerve (GSPN)", body),
wrap("Proximal to / at geniculate ganglion (labyrinthine segment)", body),
wrap("Filter paper under eyelid at medial canthus × 5 min. Normal: >25 mm wetting. "
"Abnormal: <25 mm or >50% asymmetry", body)],
[wrap("Stapedial Reflex Testing", body),
wrap("Nerve to stapedius", body),
wrap("At / proximal to pyramidal eminence (tympanic-mastoid junction)", body),
wrap("Acoustic immittance testing; absent reflex = affected", body)],
[wrap("Taste Testing", body),
wrap("Chorda tympani", body),
wrap("At / proximal to mid-mastoid segment", body),
wrap("Electrogustometry or filter paper strips with sweet/sour/salty solutions on anterior 2/3 tongue", body)],
[wrap("Salivary Flow Test (Saxon test)", body),
wrap("Chorda tympani → submandibular ganglion", body),
wrap("At / proximal to chorda tympani origin", body),
wrap("Submandibular flow comparison bilaterally; <25% of normal side = significant", body)],
]
story.append(tbl(topo_data, [38*mm, 38*mm, 42*mm, 52*mm]))
story.append(Spacer(1, 3*mm))
story.append(Paragraph(b("Interpretation Ladder:"), h2))
interp_data = [
[wrap(b("All tests abnormal"), bold_body),
wrap("Lesion at or proximal to geniculate ganglion (labyrinthine/intracranial)", body)],
[wrap(b("Schirmer normal; stapedial, taste abnormal"), bold_body),
wrap("Lesion between GSPN and stapedius branch (tympanic segment)", body)],
[wrap(b("Schirmer + Stapedial normal; taste abnormal"), bold_body),
wrap("Lesion between stapedius branch and chorda tympani origin (upper mastoid)", body)],
[wrap(b("All normal; only motor palsy"), bold_body),
wrap("Lesion at or distal to stylomastoid foramen (extratemporal / parotid)", body)],
]
story.append(tbl(interp_data, [68*mm, 102*mm], hdr_rows=0, hdr_bg=TEAL))
story.append(Spacer(1, 3*mm))
story.append(Paragraph(
"<i>Note: Topodiagnostic tests have limitations due to variability in results. MRI with gadolinium "
"enhancement provides superior anatomical localisation.</i>", note_style))
story.append(Spacer(1, 6*mm))
# ═══════════════════════════════════════════════════════════════
# LO 9 – MANAGEMENT
# ═══════════════════════════════════════════════════════════════
story.append(Paragraph("LO 9 – MANAGEMENT PLAN FOR FACIAL NERVE PALSY", h1))
story.append(Paragraph(b("1. Medical Treatment (Bell's Palsy – Acute Phase):"), h2))
med_data = [
[wrap(b("Drug"), bold_body), wrap(b("Dose & Duration"), bold_body), wrap(b("Notes"), bold_body)],
[wrap("Prednisolone (corticosteroid)", body),
wrap("1 mg/kg/day (60–80 mg/day orally) × 10 days, then taper over 4–5 days", body),
wrap("Must start within 72 hours (definitely within 2 weeks). Monitor blood sugar (DM) and BP.", body)],
[wrap("Valacyclovir (antiviral)", body),
wrap("500 mg TDS × 10 days (or Acyclovir 400 mg 5×/day)", body),
wrap("Combined with steroids may be superior. Prodrug of acyclovir – better absorption.", body)],
[wrap("Gastroprotection", body),
wrap("PPI or H2 blocker throughout steroid course", body),
wrap("Prevents GI ulceration from corticosteroids", body)],
]
story.append(tbl(med_data, [42*mm, 62*mm, 66*mm]))
story.append(Spacer(1, 3*mm))
story.append(Paragraph(b("2. Eye Care (Critical – Prevents Corneal Damage):"), h2))
for f in [
"Lubricating eye drops (artificial tears) during the day",
"Lubricating eye ointment at night",
"Moisture chamber / taping of eyelid at night (if incomplete closure)",
"Protective glasses outdoors",
"Regular ophthalmological review if incomplete closure persists",
]:
story.append(Paragraph(f"• {f}", bullet))
story.append(Spacer(1, 3*mm))
story.append(Paragraph(b("3. Physiotherapy:"), h2))
story.append(Paragraph("• Facial exercises with mirror biofeedback", bullet))
story.append(Paragraph("• Gentle massage of facial muscles", bullet))
story.append(Spacer(1, 3*mm))
story.append(Paragraph(b("4. Monitoring and Electrodiagnostic-Guided Decisions:"), h2))
story.append(Paragraph(
"• If progresses to <b>complete paralysis</b> → obtain ENoG at <b>day 3</b> of complete palsy", bullet))
story.append(Paragraph(
"• Repeat ENoG every 1–3 days until degeneration reaches >90% or voluntary EMG activity seen", bullet))
story.append(Paragraph(
"• <b>ENoG <90% degeneration</b>: continue medical treatment, good prognosis", bullet))
story.append(Paragraph(
"• <b>ENoG >90% degeneration</b> + no voluntary EMG (within 2 weeks of onset) → consider surgical decompression", bullet))
story.append(Spacer(1, 3*mm))
story.append(Paragraph(b("5. Surgical Decompression (Selected Cases):"), h2))
story.append(Paragraph(
"• Criteria: complete paralysis + >90% degeneration on ENoG + within 2 weeks of onset + no EMG activity", bullet))
story.append(Paragraph(
"• Approach: <b>Middle cranial fossa</b> (decompresses labyrinthine segment and meatal foramen – the narrowest point, 0.68 mm)", bullet))
story.append(Paragraph("• Remains controversial; evidence base still debated", bullet))
story.append(Spacer(1, 3*mm))
story.append(Paragraph(b("6. Management of Sequelae:"), h2))
seq_data = [
[wrap(b("Complication"), bold_body), wrap(b("Management"), bold_body)],
[wrap("Synkinesis (aberrant reinnervation)", body), wrap("Botulinum toxin injections; biofeedback physiotherapy", body)],
[wrap("Persistent lagophthalmos", body), wrap("Gold weight implant in upper eyelid; lateral tarsorrhaphy", body)],
[wrap("Persistent complete paralysis", body), wrap("Facial reanimation surgery: nerve grafting (greater auricular / sural nerve), muscle transfer (temporalis/masseter transposition), free gracilis transfer", body)],
[wrap("Crocodile tears", body), wrap("Botulinum toxin to lacrimal gland (if disabling)", body)],
[wrap("Ectropion", body), wrap("Lateral canthopexy or surgical correction", body)],
]
story.append(tbl(seq_data, [55*mm, 115*mm]))
story.append(Spacer(1, 6*mm))
# ═══════════════════════════════════════════════════════════════
# LO 10 – COMPLICATIONS
# ═══════════════════════════════════════════════════════════════
story.append(Paragraph("LO 10 – COMPLICATIONS FOLLOWING FACIAL PARALYSIS", h1))
comp_data = [
[wrap(b("Complication"), bold_body), wrap(b("Mechanism"), bold_body),
wrap(b("Clinical Features"), bold_body), wrap(b("Management"), bold_body)],
[wrap("Exposure Keratitis / Corneal Ulceration", body),
wrap("Lagophthalmos → corneal drying, abrasion, secondary infection", body),
wrap("Eye pain, redness, photophobia, reduced vision", body),
wrap("Lubricants, tarsorrhaphy, ophthalmology referral", body)],
[wrap("Synkinesis", body),
wrap("Aberrant reinnervation – axons regrow to incorrect muscles (e.g., eye closes when smiling)", body),
wrap("Involuntary co-contraction of facial muscles", body),
wrap("Botulinum toxin; physiotherapy; selective neurolysis", body)],
[wrap("Hemifacial Spasm", body),
wrap("Ephaptic transmission after nerve regeneration; vascular compression of facial nerve at REZ", body),
wrap("Involuntary unilateral facial muscle twitching", body),
wrap("Botulinum toxin; microvascular decompression (MVD)", body)],
[wrap("Crocodile Tears (Gustatory Lacrimation)", body),
wrap("Aberrant regeneration of salivary parasympathetic fibres → lacrimal gland", body),
wrap("Tearing while eating (instead of salivation)", body),
wrap("Botulinum toxin to lacrimal gland; often tolerated", body)],
[wrap("Facial Contracture", body),
wrap("Fibrosis and shortening of chronically denervated facial muscles", body),
wrap("Persistent facial asymmetry, stiffness, drawn appearance", body),
wrap("Physiotherapy; surgical correction in severe cases", body)],
[wrap("Ectropion", body),
wrap("Lower eyelid sagging due to orbicularis weakness", body),
wrap("Epiphora, eyelid drooping, exposure", body),
wrap("Lateral canthopexy; surgical repair", body)],
[wrap("Psychological Complications", body),
wrap("Disfigurement, communication difficulty, social withdrawal", body),
wrap("Depression, anxiety, reduced quality of life", body),
wrap("Counselling; support groups; early rehabilitation", body)],
]
story.append(tbl(comp_data, [38*mm, 44*mm, 44*mm, 44*mm]))
story.append(Spacer(1, 6*mm))
# ═══════════════════════════════════════════════════════════════
# PROGNOSIS (Bell's Palsy)
# ═══════════════════════════════════════════════════════════════
story.append(Paragraph("PROGNOSIS – BELL'S PALSY", h1))
prog_data = [
[wrap(b("Outcome"), bold_body), wrap(b("Proportion"), bold_body), wrap(b("Notes"), bold_body)],
[wrap("Complete recovery", body), wrap("~70–85%", body),
wrap("Usually within 3 weeks to 6 months; better with early steroid treatment", body)],
[wrap("Asymmetric movement / synkinesis", body), wrap("~15%", body),
wrap("Aberrant reinnervation; may require botulinum toxin", body)],
[wrap("Severe deformity, minimal recovery", body), wrap("~15%", body),
wrap("Risk factors: age >60, complete palsy, >90% ENoG degeneration, DM, hypertension", body)],
[wrap("Recurrence", body), wrap("7–12%", body),
wrap("Recurrence should raise suspicion for tumour or Melkersson-Rosenthal syndrome", body)],
]
story.append(tbl(prog_data, [55*mm, 25*mm, 90*mm]))
story.append(Spacer(1, 4*mm))
# SOURCES
story.append(HRFlowable(width="100%", thickness=1, color=colors.HexColor("#cccccc")))
story.append(Spacer(1, 2*mm))
story.append(Paragraph(
"<i>Sources: Shambaugh Surgery of the Ear (anatomy, Bell's palsy); "
"Cummings Otolaryngology Head and Neck Surgery (electrodiagnostic tests, surgical landmarks, management); "
"Bradley and Daroff's Neurology in Clinical Practice (UMN vs LMN, clinical features); "
"Scott-Brown's Otorhinolaryngology Head & Neck Surgery (surgical anatomy)</i>",
style("src", fontName="Helvetica-Oblique", fontSize=8, textColor=colors.grey,
leading=11, spaceAfter=2)))
# BUILD
doc.build(story)
print(f"PDF saved to: {OUTPUT}")
Running Command
python3 /home/daytona/workspace/facial-nerve-palsy/generate_pdf.py 2>&1
Editing File
~/facial-nerve-palsy/generate_pdf.py
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/facial-nerve-palsy/generate_pdf.py'
Running Command
python3 /home/daytona/workspace/facial-nerve-palsy/generate_pdf.py 2>&1
Your PDF is ready:
Facial Nerve Palsy ENT
PDF Document · PDF
The PDF covers all 10 learning objectives with:
- Clinical case with examination findings table and diagnosis highlight
- CN VII fibre types table (SVE, GVE, SVA, GSA, VA)
- 5 intratemporal segments with lengths, course, and branches
- Surgical landmarks by segment
- House-Brackmann grading scale
- UMN vs LMN comparison table with mechanism explanation
- 5 electrodiagnostic tests (NET, MST, ENoG, EMG, stapedial reflex)
- Causes by category (idiopathic, infective, traumatic, neoplastic, etc.)
- Topodiagnostic tests with the interpretation ladder
- Management plan (steroids, antivirals, eye care, monitoring, surgery)
- Complications table with mechanisms and management
- Prognosis table
This is a shared conversation. Sign in to Orris to start your own chat.