Normal shoulder and glenoid patho anatomy
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
I now have all the content I need to give a comprehensive answer. Let me compile this into a well-organized response.
Normal Shoulder & Glenoid Pathoanatomy
1. Bony Framework of the Normal Shoulder
The shoulder girdle consists of three bones: the clavicle, scapula, and the proximal humerus.
Clavicle
- The only bony bridge between the trunk and upper limb; palpable throughout its S-shaped length.
- The acromial (lateral) end is flat and articulates with the acromion at the AC joint.
- The sternal (medial) end is quadrangular and articulates with the manubrium and first costal cartilage.
- The inferior surface of the lateral third bears the conoid tubercle and trapezoid line - attachment points for the coracoclavicular ligament.
Scapula
-
Large, flat triangular bone with three angles (lateral, superior, inferior), three borders (superior, lateral, medial), and three processes (acromion, spine, coracoid).
-
The lateral angle bears the shallow, comma-shaped glenoid cavity, which articulates with the humeral head to form the glenohumeral joint.
-
The infraglenoid tubercle (inferior to the glenoid) anchors the long head of triceps brachii.
-
The supraglenoid tubercle (superior to the glenoid) anchors the long head of biceps brachii.
-
Gray's Anatomy for Students
2. Normal Glenoid Anatomy
Shape and Orientation
The glenoid fossa is pear-shaped or oval on sagittal sections. Normal glenoid retroversion is approximately 5-7 degrees. On axial imaging, three main glenoid surface shapes are described:
- (a) Concave - most common
- (b) Flat
- (c) Convex - associated with instability
The posteroinferior edge can be triangular (normal), rounded/J-shaped, or delta-shaped - the latter two variants are associated with posterior shoulder instability due to loss of inferior concavity.
Normal Variants (Beware - Don't Mistake for Pathology)
-
Tubercle of Assaki: A focal ridge/elevation of subchondral bone at the center of the glenoid with overlying cartilage thinning. Should NOT be mistaken for a cartilage defect.
-
Bare area: An oval area denuded of cartilage in the mid-third of the glenoid; developmental, should be differentiated from true cartilage injury.
-
Glenoid dysplasia: Osseous hypoplasia of the posteroinferior glenoid edge with flattening and sloping, marked retroversion on axial images, and hypertrophy of adjacent cartilage/labrum. Can lead to instability, accelerated OA, or posterior labral tears.
-
Imaging Anatomy: Bones, Joints, Vessels and Nerves (Thieme)
3. Glenoid Labrum - Normal Anatomy
The labrum is a fibrocartilaginous bumper that forms a circumferential ring around the glenoid rim. It is attached to articular cartilage via a narrow fibrocartilaginous transition zone but is otherwise purely fibrous.
Key Biomechanical Functions:
| Function | Detail |
|---|---|
| Deepens glenoid socket | A-P depth: 2.5 mm → 5.0 mm; S-I depth: increased to ~9 mm |
| Loss of labrum | Decreases socket depth by up to 50% in all directions |
| Concavity-compression | Most effective mechanism resisting tangential forces; humeral head resists forces up to 60% of compressive load |
| Negative intra-articular pressure | Acts as a valve/piston seal; disruption eliminates joint suction and proprioceptive feedback |
| Capsuloligamentous anchor | GHLs and biceps anchor attach to/via the labrum |
Regional Variation:
- Superiorly (above equator): Loosely attached; significant anatomic variability is normal
- Anteroinferior labrum: Intimately attached to glenoid rim - any detachment here is abnormal
Labral Shape Variants (normal):
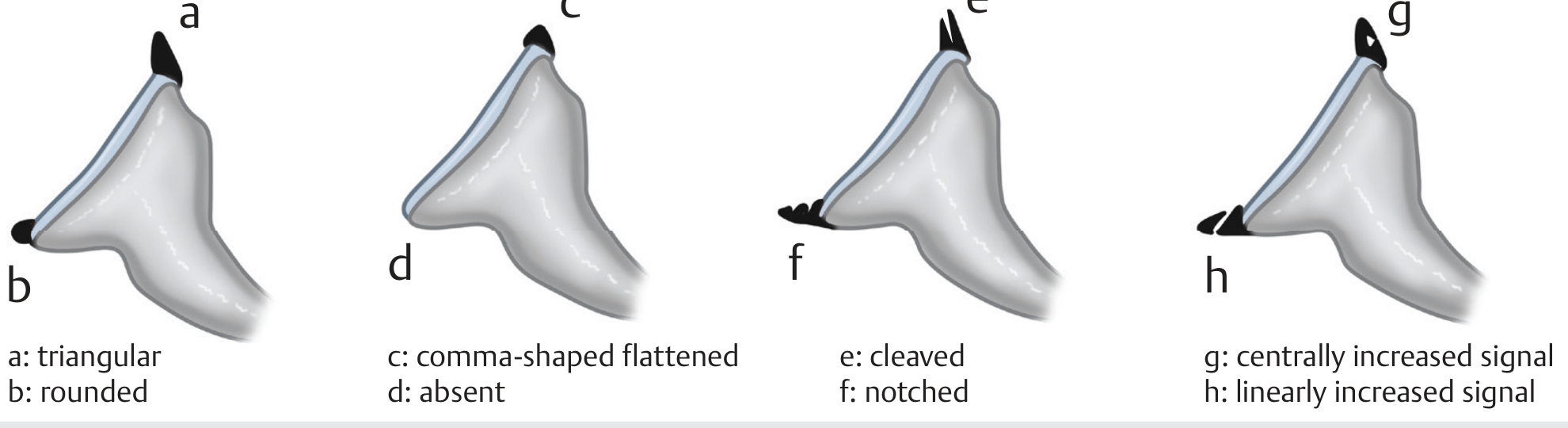
Important Labral Normal Variants (must distinguish from tears):
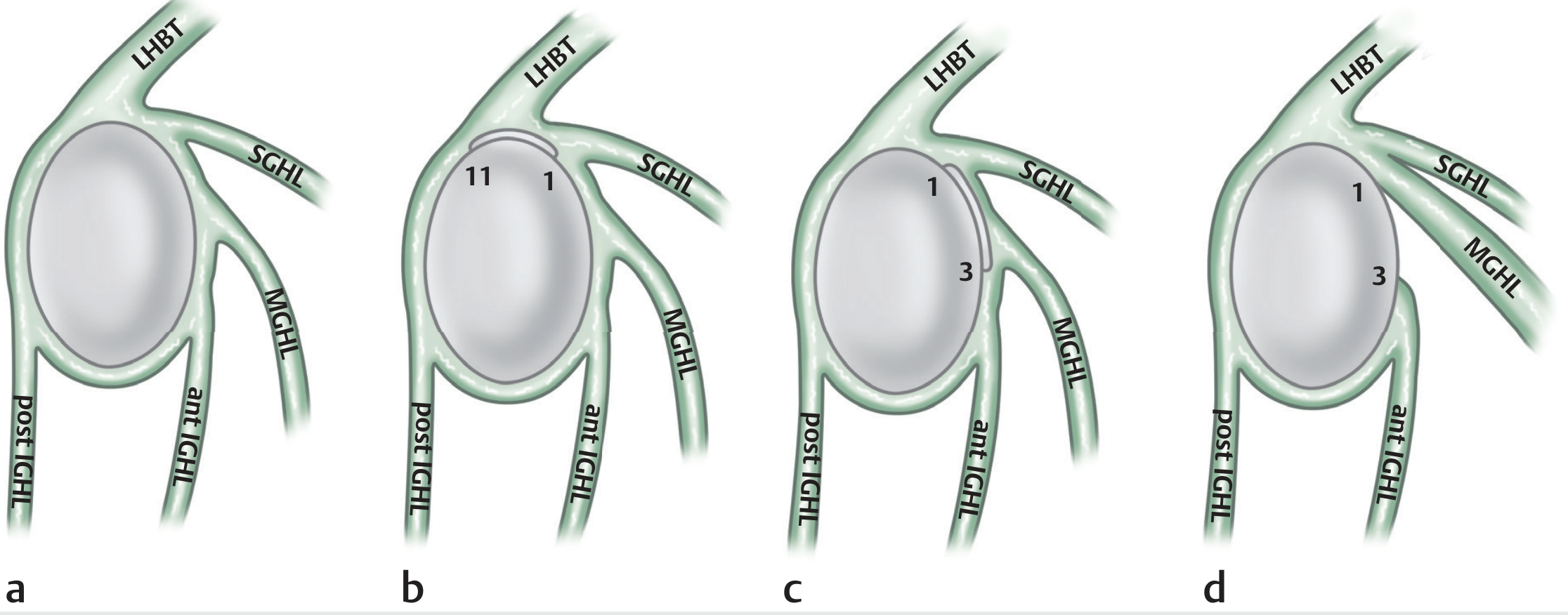
1. Sublabral Recess (Sublabral Sulcus)
- Physiologic recess at the 11-1 o'clock position
- Smooth margins, < 2 mm width
- Extends medially along glenoid rim, does not extend posterior to biceps anchor
- Must be distinguished from a Type II SLAP lesion (which extends laterally/posteriorly)
2. Sublabral Foramen (Sublabral Hole)
- Normal detachment of the anterosuperior labrum (1-3 o'clock)
- Communicates between glenohumeral joint and subscapular recess
3. Buford Complex
- Cord-like MGHL with an absent anterosuperior labrum
- Can mimic a labral tear - the key is the normal posterior labrum and the cord-like MGHL
- Imaging Anatomy: Bones, Joints, Vessels and Nerves (Thieme)
4. Glenohumeral Ligaments (GHLs)
GHLs are fibrous thickenings of the anterior joint capsule and are the most important passive stabilizers of the shoulder.
Superior GHL (SGHL)
- Origin: supraglenoid tubercle (anteroinferior to biceps origin)
- Insertion: proximal tip of the lesser tuberosity
- Function: limits inferior translation and external rotation in the adducted arm; limits posterior translation with arm in FAIR position (flexion, adduction, internal rotation)
Middle GHL (MGHL)
- Most variable - absent in up to 30%, poorly defined in another 10%
- Origin: superior glenoid (1-3 o'clock), inferior to SGHL
- Insertion: blends with subscapularis tendon (~2 cm medial to lesser tuberosity)
- Function: limits anterior translation at 45° abduction + ER; limits external rotation and inferior translation when adducted
- Buford complex: cord-like MGHL with absent anterosuperior labrum (normal variant)
Inferior GHL Complex (IGHL)
- A hammock-like structure - the primary static stabilizer against anterior dislocation
- Three components: anterior band (AIGHL), posterior band (PIGHL), and the axillary pouch between them
- Origin: anteroinferior glenoid rim and labrum
- Insertion: inferior humeral articular surface and anatomic neck
- The anterior band is the primary restraint to anterior translation in 90° abduction + ER (the position of dislocation)
- Also reinforced on the glenoid side by the spiral GHL (fasciculus obliquus)
Rotator Interval
-
The triangular zone between the superior border of subscapularis and anterior border of supraspinatus
-
Contains: SGHL and coracohumeral ligament (CHL)
-
CHL: extends from the lateral coracoid to greater and lesser tuberosities (adjacent to bicipital groove)
-
Rotator interval deficiency → multidirectional instability (MDI)
-
Rotator interval contracture → restricted ER and FF (adhesive capsulitis, post-traumatic stiffness)
-
Rockwood and Green's Fractures in Adults 10e
5. Glenoid Pathoanatomy
A. Anterior Instability - Bankart Lesion & Bone Loss
Bony Bankart Lesion
- Avulsion of the anteroinferior glenoid rim with the attached labrum and IGHL complex
- Prevalence of glenoid rim lesions in recurrent instability: up to 90% (50% bony Bankart + 40% glenoid erosion)
- The "inverted pear" glenoid morphology (loss of the normal pear shape) is associated with 25-27% loss of anteroinferior glenoid width - a critical finding indicating need for bony augmentation
Critical Glenoid Bone Loss Thresholds:
| Threshold | Clinical Significance |
|---|---|
| Historically: 20-25% | Traditional "critical" cutoff requiring bony procedure (Latarjet/bone graft) |
| 13.5% (Shaha et al.) | "Subcritical" bone loss - still leads to significantly worse WOSI scores and higher failure rate |
| 17.3% (Shin et al.) | Failure rate jumps from 3.7% to 42.9% above this threshold |
| >15% | Recent biomechanical studies also identify this as clinically significant |
- Measurement: Glenoid bone loss is calculated by comparing the surface area of the defect to the surface area of the inferior 2/3 of the glenoid (best-fit circle method) - A/B × 100 where A = missing anterior glenoid width and B = diameter of the inferior glenoid circle.
B. Degenerative Glenoid Wear - Walch Classification (Modified by Bercik)
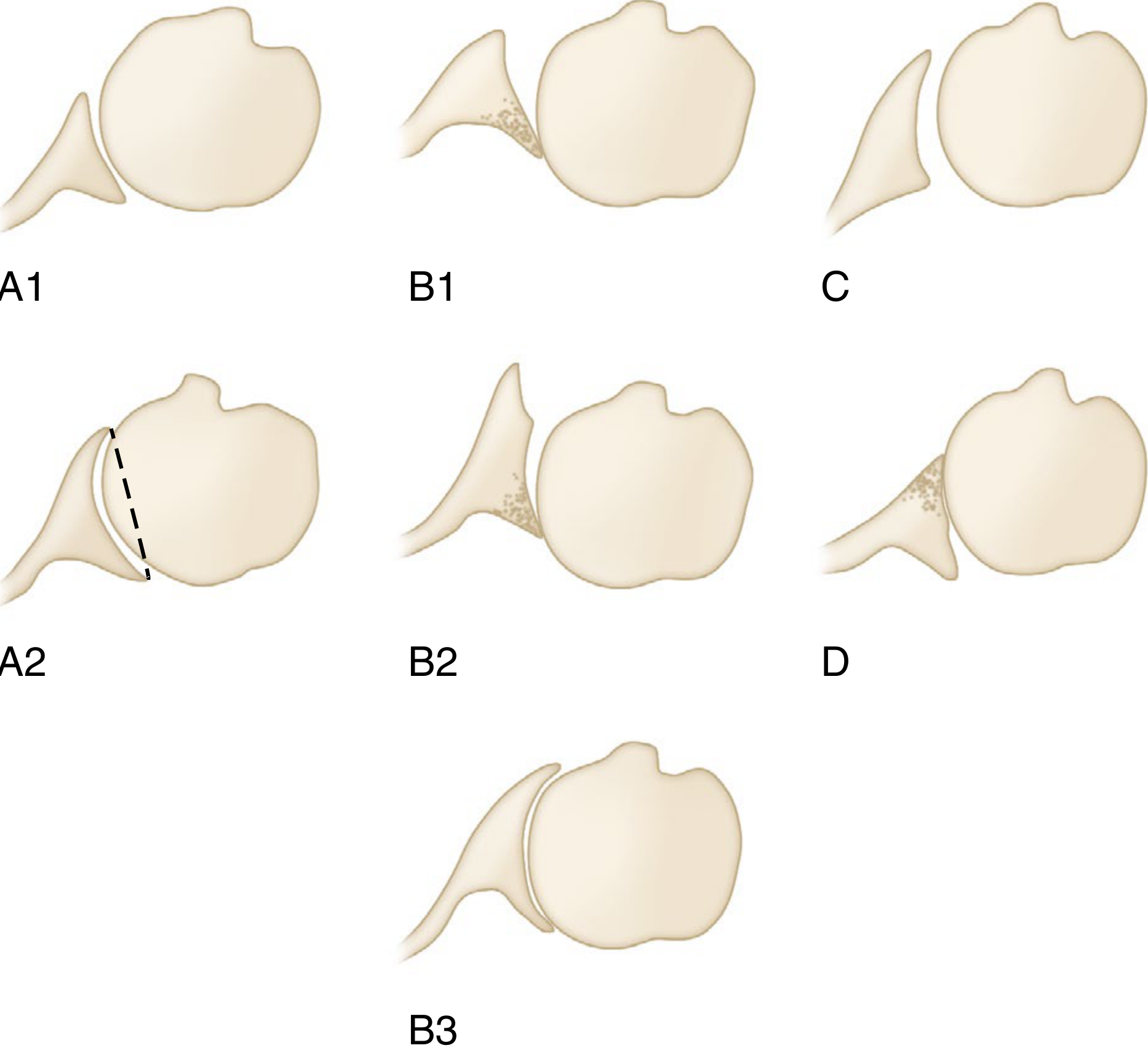
| Type | Description |
|---|---|
| A1 | Central wear, minor |
| A2 | Central wear; line from anterior to posterior rim transects humeral head |
| B1 | Posterior wear without retroversion; joint space narrowing, subchondral sclerosis |
| B2 | Biconcave glenoid - posterior wear with retroversion; classic OA pattern |
| B3 | Monoconcave, posterior wear, >15° retroversion, >70% posterior humeral head subluxation |
| C | Excessive glenoid retroversion >25° (dysplastic) |
| D | Any anteversion or anterior humeral head subluxation <40% |
Key points:
-
Central (Type A) wear is most common in rheumatoid arthritis; < 1 cm depth generally precludes glenoid component fixation without bone grafting
-
Posterior (Type B) wear is most common in osteoarthritis (posterior humeral subluxation tendency); can progress to severe B2/B3 patterns
-
Sperling classification grades severity: None → Mild (erosion to subchondral bone) → Moderate (hemispheric deformation + medialization) → Severe (bone loss to coracoid base)
-
Campbell's Operative Orthopaedics 15e 2026
C. Glenoid Dysplasia
- Developmental osseous hypoplasia of the posteroinferior glenoid
- Features: flattening and sloping of the posterior glenoid edge, marked retroversion on axial MRI, hypertrophy of adjacent cartilage and labrum
- Consequences: posterior shoulder instability, accelerated OA, posterior labral tears
Summary Table: Normal vs. Pathological Glenoid
| Feature | Normal | Pathological |
|---|---|---|
| Retroversion | 5-7° | >15-25° (dysplasia/wear) |
| Labrum attachment (anteroinferior) | Intimately attached | Detached = Bankart |
| Labrum attachment (superior) | Loosely attached, variable | SLAP tear if extends posteriorly/laterally |
| Glenoid shape | Pear-shaped, concave | Inverted pear (bone loss), biconcave (B2), flat (C) |
| Bone loss | None | >13.5-25% = surgical threshold |
| Sublabral sulcus | < 2 mm, smooth, medial extension | SLAP = extends lateral/posterior |
| Absent anterosuperior labrum | Normal if Buford complex | Abnormal without cord-like MGHL |
Key Sources:
- Gray's Anatomy for Students (glenohumeral bony anatomy)
- Imaging Anatomy: Bones, Joints, Vessels and Nerves, Vol. 3 (glenoid variants, labral anatomy, GHLs)
- Rockwood and Green's Fractures in Adults, 10e 2025 (labral biomechanics, GHLs, critical bone loss)
- Campbell's Operative Orthopaedics, 15e 2026 (Walch/Bercik glenoid wear classification)
Recurrent patellar dislocation
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive content for a thorough answer on recurrent patellar dislocation.
Recurrent Patellar Dislocation
1. Overview & Epidemiology
Patellar dislocation is almost always lateral. It is most common in young athletes after trauma, but the pathogenesis is multifactorial with a genetic predisposition.
-
Recurrence rate after a first-time dislocation: 15% to 60%
-
Associated with ongoing anterior knee pain even between episodes
-
Risk factors for recurrence: younger age, female sex, patella alta, and trochlear dysplasia
-
In patients with joint hypermobility, instability is attributed to ligamentous laxity combined with muscular imbalance - joint hypermobility is a poor prognostic factor for operative outcomes
-
Miller's Review of Orthopaedics 9e; Rheumatology 2e (Elsevier)
2. Pathoanatomy & Risk Factors
Patellar instability is driven by a combination of bony and soft-tissue abnormalities. Understanding each is essential for surgical planning.
A. Trochlear Dysplasia (Most Important Bony Risk Factor)
The trochlear groove normally guides the patella into engagement at ~20-30° of flexion. A shallow or dysplastic trochlea removes this bony constraint.
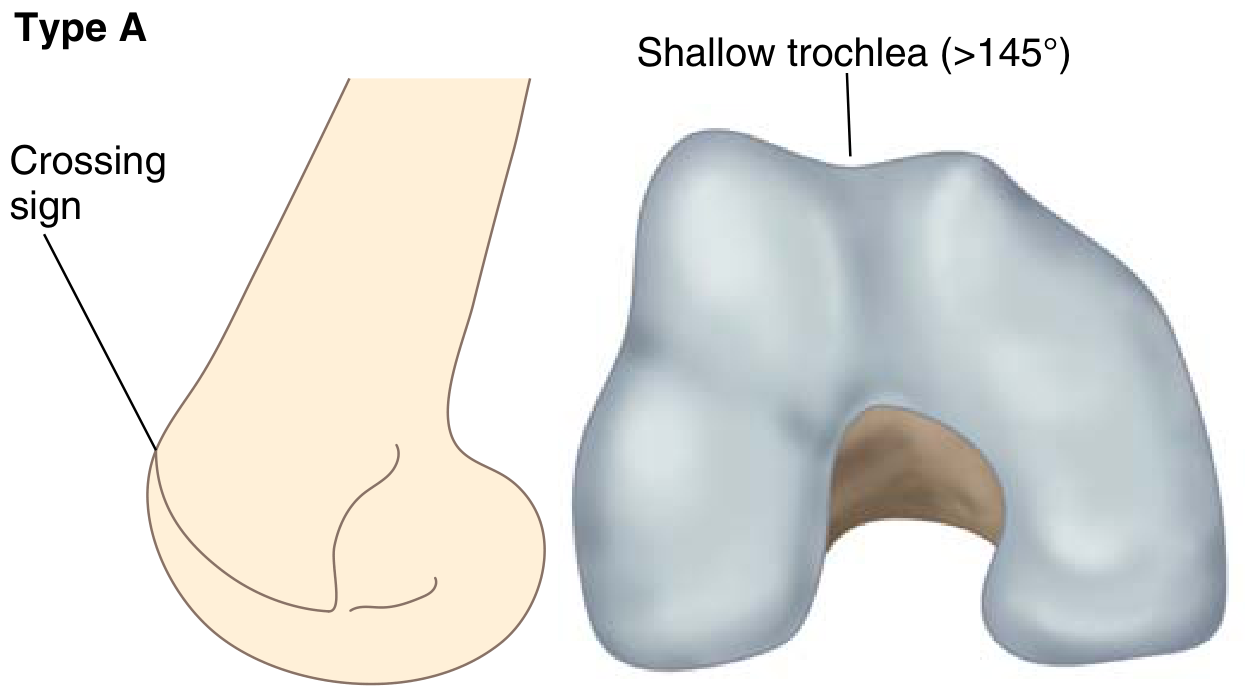
Dejour Classification (identified on lateral radiograph and CT/MRI):
| Type | Lateral Radiograph | 3D Morphology |
|---|---|---|
| A | Crossing sign only | Shallow trochlea (sulcus angle >145°) |
| B | Crossing sign + supratrochlear spur | Flat trochlea |
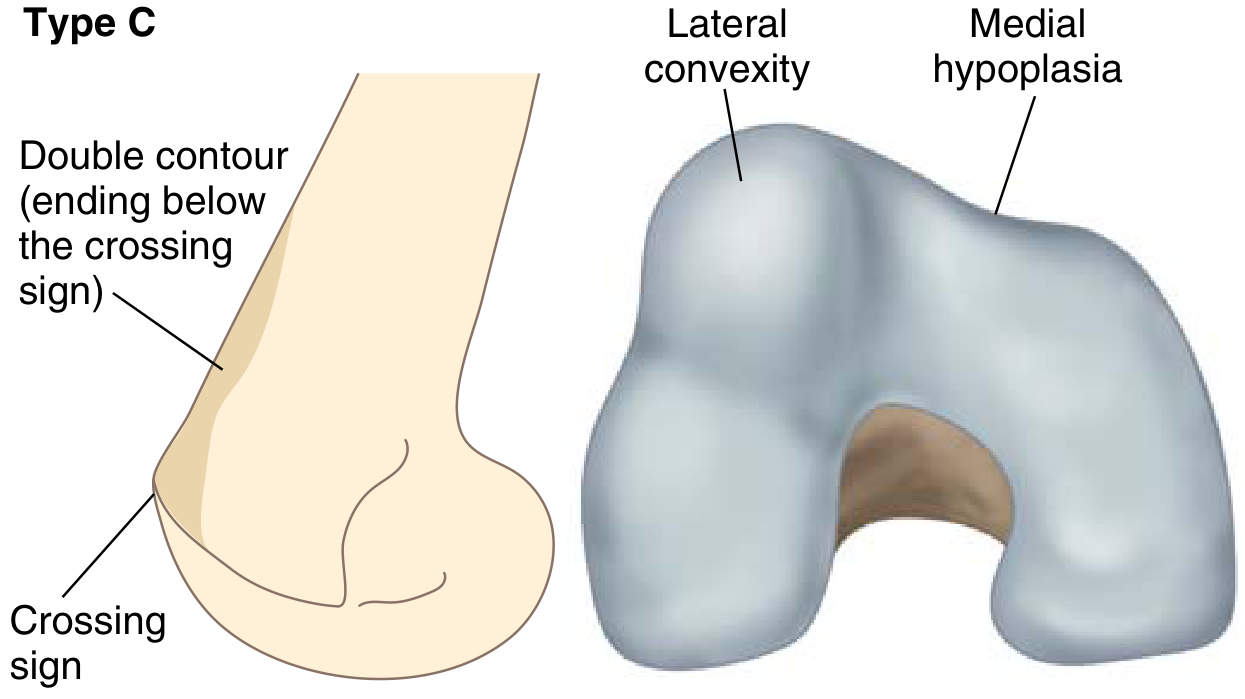
| C | Double contour ending below crossing sign | Lateral convexity + medial hypoplasia |
| D | Double contour + supratrochlear spur | Cliff pattern - asymmetric trochlea |
- Crossing sign: The trochlear groove floor line crosses the anterior femoral condyle on a true lateral radiograph (normally intersects the anterior femoral cortex, not the condyle)
- Supratrochlear spur: a bony prominence at the proximal trochlea
- Types C and D are the most severe forms
B. TT-TG Distance (Tibial Tubercle - Trochlear Groove Offset)
Measures the lateral offset of the tibial tubercle relative to the deepest point of the trochlear groove. Measured on CT (MRI underestimates).
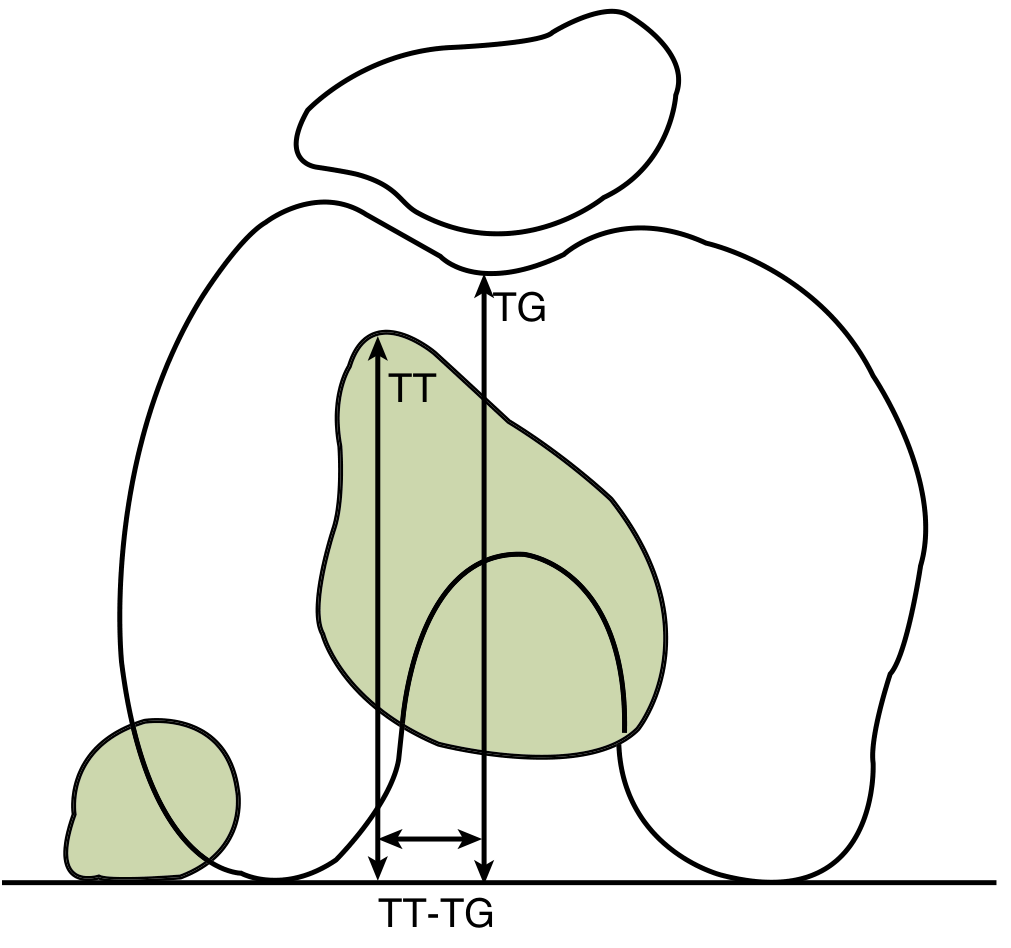
| TT-TG Value | Interpretation |
|---|---|
| 9-13 mm | Normal |
| 15-20 mm | Questionably abnormal |
| >20 mm | Highly associated with patellar instability → surgical threshold for distal realignment |
C. Patella Alta
High-riding patella means the patella does not engage the trochlear groove until late in flexion, spending more time in an unstable position.
- Measured by the Caton-Deschamps or Insall-Salvati ratio
- A component of the "Dejour triad" of pathoanatomy (trochlear dysplasia + patella alta + increased TT-TG)
D. MPFL Disruption (Soft Tissue)
The Medial Patellofemoral Ligament (MPFL) is the primary passive restraint to lateral patellar translation, providing ~50-60% of medial restraining force.
- In an acute dislocation: MPFL is disrupted in virtually all cases, most frequently at its patellar insertion
- MRI finding after dislocation: bone bruise pattern on the lateral femoral condyle and medial patellar facet (pathognomonic kissing contusions)
- Chronic MPFL insufficiency → recurrent lateral dislocation
E. Q Angle / Lower Limb Alignment
Increased Q angle (lateral pull of quadriceps on patella) contributes to lateral instability. Associated alignment problems:
- Femoral anteversion
- Genu valgum
- External tibial torsion (planted-foot mechanism)
- Pronated feet
- When all present together: "Miserable Malalignment Syndrome" - especially symptomatic in adolescents
F. VMO Insufficiency
Weakness of the vastus medialis obliquus (VMO) removes the main dynamic medial stabilizer, allowing lateral drift of the patella.
3. Clinical Features
| Feature | Detail |
|---|---|
| Mechanism | External tibial rotation with planted foot OR direct blow to medial knee |
| Pop | Often felt at time of dislocation (can mimic ACL tear) |
| Spontaneous reduction | Common - patella often self-reduces with knee extension |
| Hemarthrosis | Common cause of knee hemarthrosis |
| J sign | Patella tracks laterally in extension and snaps into the groove at ~30° of flexion |
| Patellar apprehension test | Lateral pressure on patella in extension elicits fear/quadriceps guarding |
| Lateral patellar glide | Three to four quadrants of lateral glide = significant laxity |
| Articular cartilage damage | Medial facet of patella is most commonly injured (shear forces during reduction); loose bodies may result |
4. Investigations
Radiographs
- AP, lateral, and Merchant (axial/skyline) views
- Identify: fractures, loose bodies, patella alta, malalignment, trochlear morphology
- Crossing sign and supratrochlear spur for trochlear dysplasia on the lateral view
- Congruence angle and sulcus angle on the axial view
- Normal sulcus angle: ~138° (>150° = abnormally shallow groove)
- Normal congruence angle: ~-6° (lateral displacement of ridge = positive)
CT
- Gold standard for TT-TG measurement (MRI underestimates)
- Evaluates trochlear morphology (Dejour classification)
- Assesses patellar tilt and subluxation
MRI
- Bone bruise pattern: lateral femoral condyle + medial patella = pathognomonic of lateral dislocation
- MPFL disruption - most often at patellar attachment
- Articular cartilage damage assessment
- TT-TG measurable but less accurate than CT
- Soft tissue anatomy (retinaculum, tendons)
5. Management
A. Acute First-Time Dislocation
- Traditionally managed non-operatively: patellar stabilizing brace + physiotherapy focused on VMO strengthening
- Surgery considered if: loose body present, significant chondral damage, or associated fracture
- Some advocate early arthroscopic MPFL repair at the medial epicondyle (controversial)
B. Recurrent Patellar Dislocation - Surgical Options
Surgery is directed at correcting the anatomical abnormality responsible:
Proximal Realignment - MPFL Reconstruction
- Primary surgical treatment for recurrent patellar instability
- Graft: usually gracilis or semitendinosus autograft (or allograft)
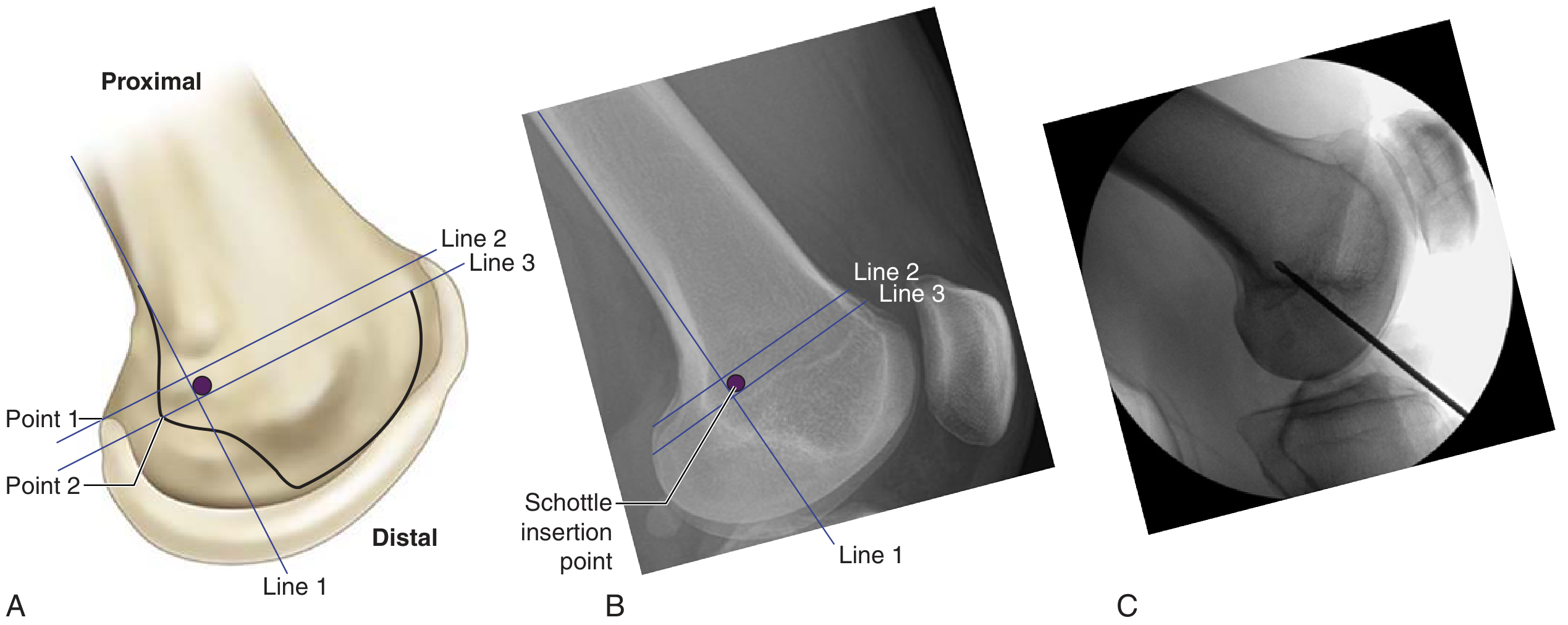
- Femoral attachment at the Schottle point (anatomic origin):
- 1 mm anterior to the posterior cortex extension line
- 2.5 mm distal to the posterior origin of the medial femoral condyle
- Proximal to the posterior point of the Blumensaat line on lateral radiograph
- Critical tunnel placement principle:
- Too proximal → graft tight in flexion (over-constrains)
- Too distal → graft loose in flexion (fails to stabilize)
- Complication: Medial patellar instability or medial patellar OA from overtightening
Techniques Now Largely Abandoned:
- VMO advancement (Green procedure)
- Isolated medial retinacular plication
- Isolated lateral release should NOT be performed for patellar instability (does not address the problem and can worsen medial instability)
Distal Realignment - Tibial Tubercle Osteotomy (TTO)
- Anterior medialization of the tibial tubercle (Fulkerson-type osteotomy)
- Indicated when Q angle is increased OR TT-TG distance >20 mm
- Contraindication: proximal arthrosis of the medial patellar facet (medialization will load the already damaged medial facet)
- Combined with MPFL reconstruction in many cases
Trochleoplasty
- Indicated for severe trochlear dysplasia (Dejour C or D) that cannot be adequately addressed by soft-tissue procedures alone
- Reshapes/deepens the trochlear groove
- Generally reserved for cases where other procedures have failed or severe dysplasia is the primary driver
6. Summary Algorithm
Recurrent Patellar Dislocation
↓
Evaluate anatomy:
- TT-TG (CT)
- Trochlear dysplasia (Dejour)
- Patella alta
- MPFL integrity (MRI)
↓
TT-TG <20 mm TT-TG >20 mm
No bony dysplasia OR increased Q angle
↓ ↓
MPFL reconstruction MPFL + distal TTO
(Fulkerson-type)
↓
Severe trochlear dysplasia (C/D)?
↓
Add trochleoplasty
Key Sources:
- Miller's Review of Orthopaedics, 9e (epidemiology, Dejour classification, TT-TG, MPFL reconstruction, Schottle point)
- Rheumatology 2e - Elsevier (hypermobility-related instability, prognosis)
- Roberts and Hedges' Clinical Procedures in Emergency Medicine (acute management)
Recurrent patellar dislocation
I just covered this topic in detail in my previous response. Here's a concise structured summary for quick reference:
Recurrent Patellar Dislocation - Quick Reference
Pathoanatomy (The "Dejour Triad")
| Factor | Threshold / Detail |
|---|---|
| Trochlear dysplasia | Dejour A-D; identified by crossing sign ± supratrochlear spur on lateral XR |
| Patella alta | Caton-Deschamps or Insall-Salvati ratio elevated |
| Increased TT-TG | >20 mm on CT = clearly pathological |
| MPFL rupture | At patellar insertion in virtually all dislocations |
| VMO weakness | Loss of dynamic medial stabilizer |
| Malalignment | Femoral anteversion + genu valgum + external tibial torsion + pronated feet = "Miserable malalignment syndrome" |
Recurrence Risk Factors
Younger age · Female sex · Patella alta · Trochlear dysplasia · Joint hypermobility (also predicts poor surgical outcome)
Dejour Trochlear Dysplasia Classification
| Type | Lateral XR Finding | Morphology |
|---|---|---|
| A | Crossing sign only | Shallow trochlea (sulcus >145°) |
| B | Crossing sign + supratrochlear spur | Flat trochlea |
| C | Double contour below crossing sign | Lateral convexity + medial hypoplasia |
| D | Double contour + spur | Cliff pattern (most severe) |
Key Imaging Findings
- MRI: Kissing bone bruise (lateral femoral condyle + medial patellar facet) - pathognomonic of lateral dislocation; MPFL tear most often at patellar insertion
- CT: Gold standard for TT-TG measurement; trochlear morphology
- Lateral XR: Crossing sign, supratrochlear spur, sulcus angle
- Axial XR: Sulcus angle (normal ~138°; >150° = shallow groove); congruence angle (normal ~-6°)
TT-TG Distance
| Value | Significance |
|---|---|
| 9-13 mm | Normal |
| 15-20 mm | Borderline |
| >20 mm | Highly associated with instability → surgical indication for distal realignment |
Surgical Decision Framework
Recurrent instability confirmed
↓
TT-TG ≤20 mm? TT-TG >20 mm / increased Q angle?
↓ ↓
MPFL reconstruction MPFL + Tibial Tubercle Osteotomy
(gracilis/ST graft at (Fulkerson anteromedialization)
Schottle point)
↓
Severe dysplasia (C/D) driving instability?
↓
Add trochleoplasty
MPFL Reconstruction - Key Technical Points
- Graft: gracilis or semitendinosus (auto or allograft)
- Femoral tunnel at Schottle point (1 mm anterior to posterior cortex line; 2.5 mm distal to posterior MFC origin; proximal to Blumensaat line)
- Too proximal = tight in flexion; Too distal = loose in flexion
- Patellar attachment: dual-tunnel or transosseous technique
- Complication: Medial patellar instability / OA from overtightening
Tibial Tubercle Osteotomy (TTO)
- Anteromedialization (Fulkerson) for increased TT-TG or Q angle
- Contraindication: proximal/medial patellar arthrosis (medialization loads damaged cartilage)
Abandoned / Deprecated Procedures
- Isolated lateral release - should NOT be performed for instability
- VMO advancement (Green procedure)
- Isolated medial retinacular plication
Non-Operative Treatment
First-time dislocation: patellar stabilizing brace + physiotherapy (VMO + hip abductor strengthening). Surgery only if loose body, chondral fracture, or recurrence despite rehab. In hypermobile patients, non-operative treatment is preferred as surgery has poor outcomes.
This is a shared conversation. Sign in to Orris to start your own chat.