AION
AION is the personification of eternity, cyclical time, and the zodiac in Greco-Roman religion and philosophy. Here's a concise overview:
AION (Αἰών)
Nature & Meaning
- The name means "age," "eternity," or "vital force" in Greek
- Represented unbounded, cyclical time — distinct from Chronos (sequential, linear time) and Kairos (the opportune moment)
- Associated with the eternal, ever-renewing cosmos rather than finite duration
Iconography
- Depicted as a nude or semi-nude male figure standing inside or entwined by a zodiac wheel (ouroboros)
- Often shown with lion's head, four wings, and a serpent coiled around his body — especially in Mithraic art (called Leontocephaline or Arimanius)
- Sometimes portrayed as a young, radiant figure (related to the eternal youth of the cosmos)
Religious & Philosophical Contexts
| Context | Role |
|---|---|
| Orphic tradition | Primordial deity of time and eternity, born from the cosmic egg |
| Mithraic mysteries | Central enigmatic figure — the lion-headed god of boundless time |
| Neoplatonism | Aion is the eternal now — the timeless realm of the Intellect (Nous) |
| Gnostic texts | "Aeons" are divine emanations or cosmic powers radiating from the supreme being |
| Alexandria (238 CE) | A formal mystery cult celebrated Aion's birth on January 6th — possibly influencing later Christian Epiphany traditions |
Philosophical Significance
- Plato (Timaeus) contrasted Aion (eternity) with Chronos (moving image of eternity) — the cosmos is a temporal reflection of the eternal Aion
- Plotinus placed Aion in the realm of pure Being and Intellect — beyond time, self-contained and complete
- Heraclitus is sometimes linked to the concept: "Aion is a child playing draughts; the kingdom belongs to a child" (Fragment 52)
Legacy
- The word survives in "eon/aeon" (a vast span of time)
- Carl Jung used "Aion" as the title of a 1951 work examining the archetype of the self across two thousand years of Christian symbolism
- The concept deeply influenced Gnostic Christianity, Hermeticism, and Neoplatonic theology
Is there a specific aspect of Aion you'd like to explore further — mythological, philosophical, artistic, or historical?
AION EYE
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Here is a comprehensive clinical overview of Anterior Ischemic Optic Neuropathy (AION):
Anterior Ischemic Optic Neuropathy (AION)
What Is It?
AION is ischemic injury to the optic nerve head caused by insufficient blood flow through the posterior ciliary arteries that supply the optic disc. It is the most frequent cause of optic disc swelling in adults over 50 and is conceptually analogous to a stroke of the optic nerve — ranging from transient ischemia to frank infarction.
Two Main Types
| Feature | Nonarteritic AION (NA-AION) | Arteritic AION (A-AION) |
|---|---|---|
| Cause | Noninflammatory vascular disease (atherosclerosis) | Giant cell (temporal) arteritis |
| Age | Usually >40 years | Usually >60–70 years |
| Frequency | Much more common | Less common but more severe |
| Visual loss | Variable; may improve slightly (~32%) | More profound; often permanent |
| Disc appearance | Swollen, pale, peripapillary hemorrhages | Same, but pallor more striking |
| Premonitory symptoms | Absent | Amaurosis fugax in ~10% |
| Systemic symptoms | Absent | Headache, jaw claudication, scalp tenderness, polymyalgia rheumatica |
| ESR/CRP | Normal | Elevated |
| Treatment | None proven effective; steroids NOT indicated | High-dose corticosteroids urgently (protects fellow eye) |
Pathophysiology
- Occlusion of the posterior ciliary artery (by atherosclerosis or vasculitis) reduces perfusion to the optic disc
- Zones of relative ischemia may surround segmental infarcts — some function may recover; infarcted tissue does not regenerate
- A small cup-to-disc ratio ("disc at risk") — crowded optic nerve architecture — is a key structural predisposing factor
- AION in one eye significantly increases risk in the fellow eye
Clinical Features (NA-AION)
- Sudden, painless monocular visual loss — may show stuttering progression
- Visual field defect: typically altitudinal (inferior > superior), but central, cecocentral, or arcuate defects also occur
- Relative afferent pupillary defect (RAPD) in unilateral or asymmetric cases
- Fundoscopy: swollen, pale optic disc with peripapillary flame-shaped (splinter) hemorrhages
- End-stage: segmental or diffuse optic atrophy without significant cupping (distinguishes from glaucoma)
Risk Factors (NA-AION)
- Hypertension, diabetes mellitus, hypercholesterolemia
- Smoking, ischemic heart disease
- Renal failure
- Collagen vascular disease, antiphospholipid antibody syndrome, migraine
- Acute blood loss or perioperative hypotension
- Post-cataract extraction
- Small cup-to-disc ratio ("disc at risk")
Fundoscopic Appearance
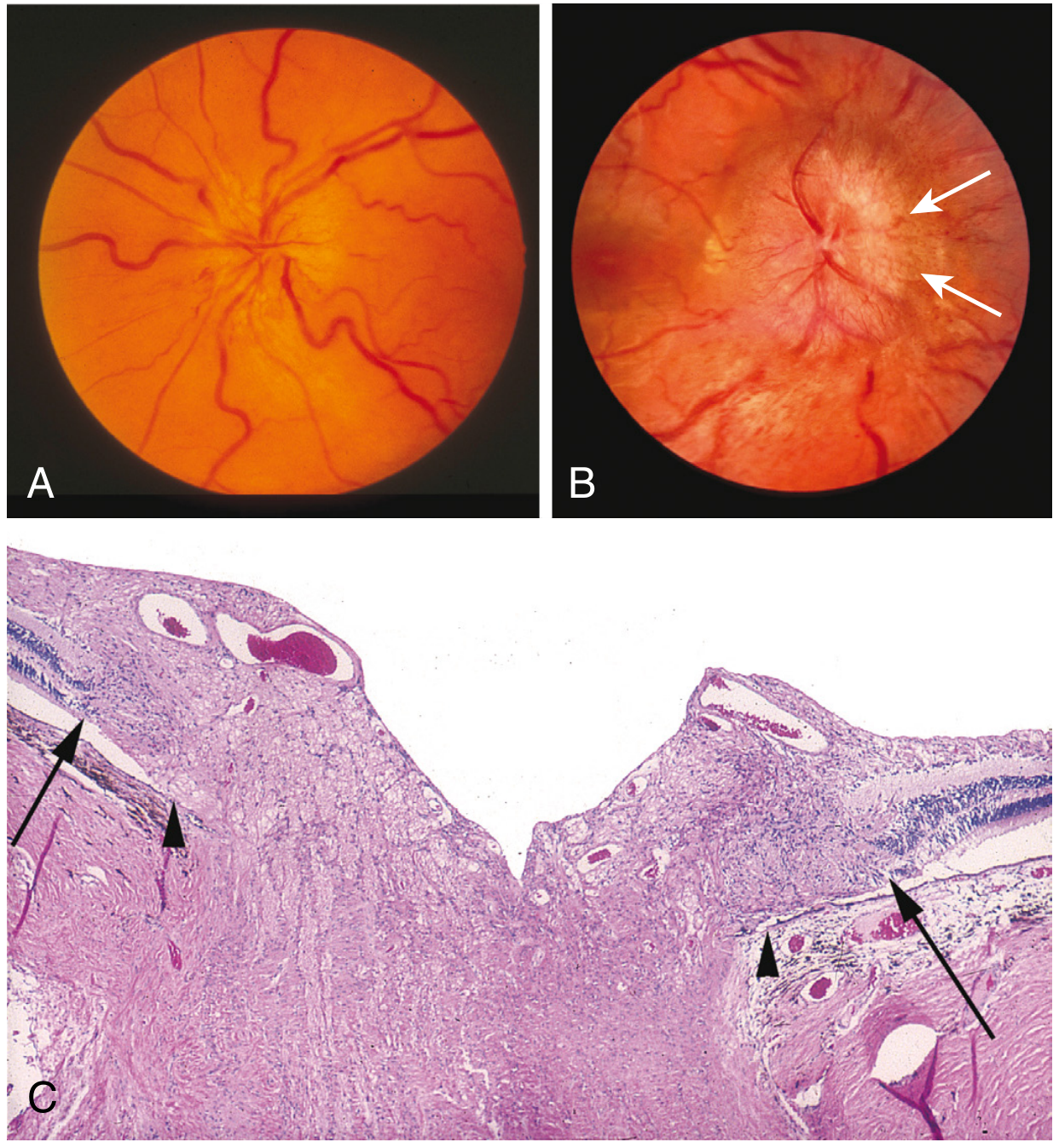
Fig: (A) Normal optic disc. (B) In acute AION, the optic nerve head is swollen and pale due to decreased perfusion. (C) Histological section showing the optic nerve head architecture. — Robbins, Cotran & Kumar Pathologic Basis of Disease
Key Distinguishing Points
- AION vs Optic Neuritis (ON): AION is usually permanent; ON often recovers. AION is painless; ON is painful. AION is more common in older patients with vascular risk factors.
- AION vs Papilledema: In AION the disc is pale and swollen (ischemia); in papilledema the disc is hyperemic and swollen (venous congestion from raised ICP).
- AION vs Glaucoma: End-stage AION shows optic atrophy without cupping; glaucoma shows cupping with atrophy.
- Posterior ION (PION): Ischemia of the retrobulbar optic nerve with no disc swelling — when seen, always suspect giant cell arteritis.
Management
- NA-AION: No proven effective treatment. Modify vascular risk factors. Do not prescribe glucocorticoids.
- A-AION: Urgent high-dose IV/oral corticosteroids to prevent bilateral blindness. A temporal artery biopsy confirms the diagnosis but treatment must not be delayed.
Sources: Harrison's Principles of Internal Medicine 22E; Localization in Clinical Neurology 8e; Rosen's Emergency Medicine; Robbins, Cotran & Kumar Pathologic Basis of Disease; Neuroanatomy Through Clinical Cases 3e
This is a shared conversation. Sign in to Orris to start your own chat.