Instrumental diagnostic methods of the gastrointestinal tract (X-ray, esophagogastroduodenoscopy, colonoscopy, rectosigmoidoscopy). Gastric juice and stool examination. Coprogram interpretation
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Now I have comprehensive material. Let me compile a thorough, well-structured answer.
Instrumental Diagnostic Methods of the Gastrointestinal Tract
1. Plain and Contrast Radiography (X-Ray)
Plain Abdominal X-Ray
Used to detect free air under the diaphragm (perforation), intestinal obstruction (air-fluid levels, dilated loops), and foreign bodies.
Barium Studies
Barium Esophagogram
The barium esophagogram is an inexpensive, readily available, and noninvasive test. It is most useful in demonstrating anatomic narrowing of the esophagus and assessing the presence and reducibility of a hiatal hernia. Schatzki's rings, webs, or minimally narrowed peptic strictures may be detected that are sometimes missed by endoscopy (which may not adequately distend the esophagus). Giving a 13-mm radiopaque pill or marshmallow along with barium liquid helps identify subtle narrowings. The barium esophagogram allows good assessment of peristalsis and is helpful preoperatively in identifying a weak esophageal pump.
- Sensitivity for moderate-to-severe esophagitis: 79–100%; mild esophagitis is usually missed
- Spontaneous reflux of barium into the proximal esophagus is highly specific for GER, but not sensitive
- Provocative maneuvers (leg lifting, coughing, Valsalva, water siphon) improve sensitivity
Barium Enema (BE)
Detection of adenomas by barium enema (BE) depends on size:
- Polyps < 6 mm: detected in 32% of cases
- 6–10 mm: 53%
-
10 mm: 48%
Common sources of error include inadequate bowel preparation (5–10% false-positive rate) and diagnostic difficulty from diverticulosis, redundant bowel, or poor mucosal coating (10% false-negative rate). Because BE was never formally tested as a colon cancer screening tool, its use for CRC screening has largely been abandoned in favor of colonoscopy or CT colonography. In acute lower GI bleeding, emergency barium enema has no role — it cannot demonstrate vascular lesions, may be misleading if only diverticula are seen, and can interfere with urgent colonoscopy or angiography.
— Sleisenger and Fordtran's Gastrointestinal and Liver Disease
2. Esophagogastroduodenoscopy (EGD / Upper GI Endoscopy)
The three major applications of GI endoscopy are:
- Diagnostic — defining the source of GI bleeding, staging GI cancers, obtaining samples for histology or culture
- Therapeutic — hemostasis, lesion resection, remodeling of the GI tract (obesity management, creating passages between lumens)
- Combined modality — with interventional radiology or surgery
Instrument
Flexible endoscopes are equipped with a high-resolution video chip at the end of a flexible tube and two fiberoptic light bundles. The endoscope has a water channel for lens irrigation and a suction/instrument channel through which biopsy forceps, cytology brushes, polypectomy snares, bipolar cautery probes, and other accessories can be passed.
Preparation
- Fasting for at least 6 hours prior to the procedure
- Patients with achalasia (POEM): clear liquids for 2 days
- Anticoagulants and antiplatelet agents should be discontinued in advance (see table below)
- Sedation: typically deep sedation with propofol in the USA; alternatively midazolam + fentanyl; or no sedation in selected patients
Scope of Examination
Upper endoscopy visualizes:
- Posterior pharynx, epiglottis, upper esophageal sphincter, larynx, vallecula
- Entire esophagus and stomach
- Duodenal bulb and first and second portions of the duodenum
Endoscopic Images — Upper GI Abnormalities
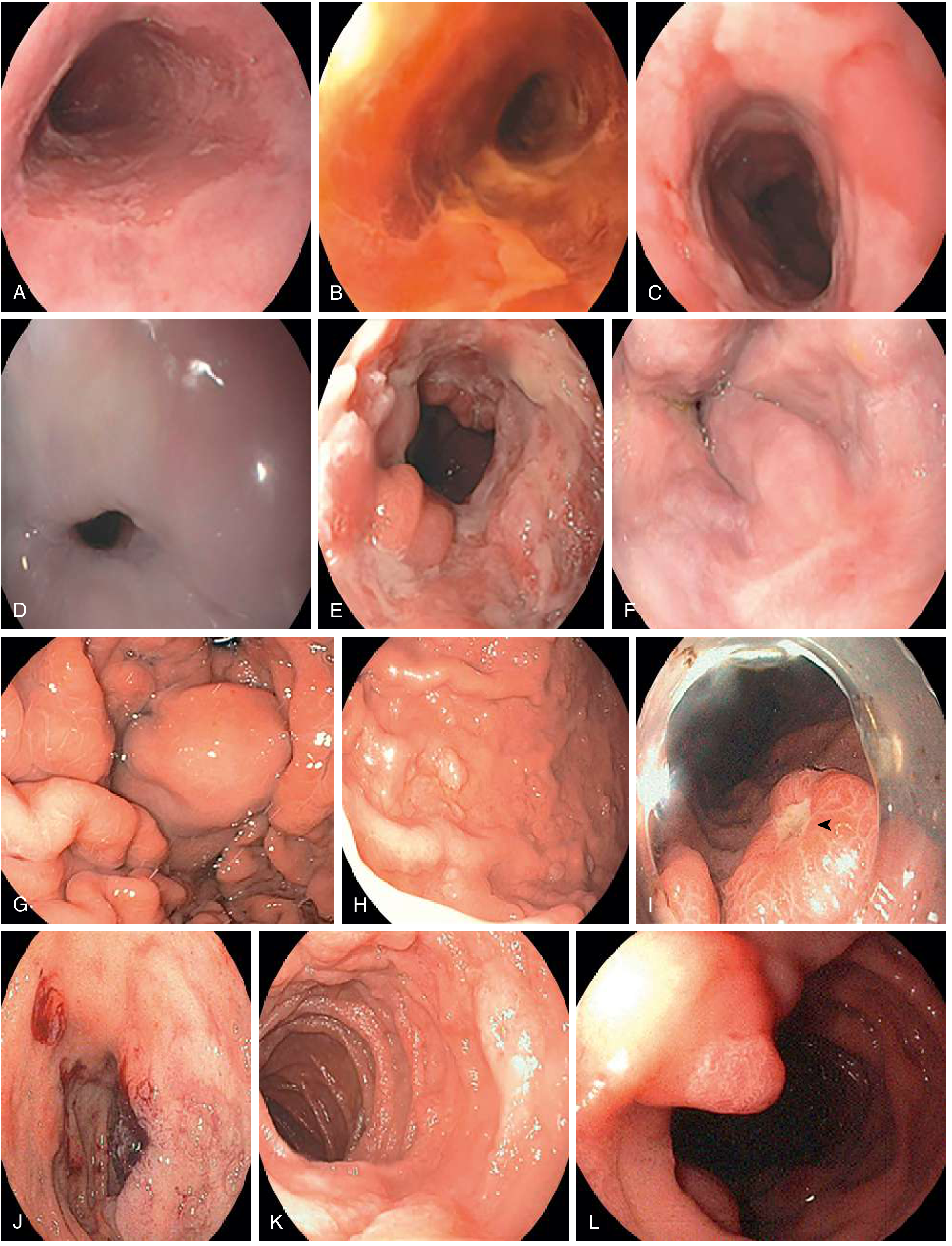
A. Barrett esophagus (salmon-colored intestinal metaplasia) | B. Post-Lugol solution — whitish areas (no iodine uptake) = dysplasia | C. Erosive esophagitis | D. Esophageal stricture | E. Excavating distal esophageal cancer | F. Submucosal esophageal varices | G. Rugal folds with gastric varix | H. Hyperplastic polyp (benign, PPI-associated) | I. Gastric ulcer (black arrow) | J. Duodenal ulcer in the bulb | K. Duodenal adenoma | L. Normal ampulla of Vater
— Goldman-Cecil Medicine
3. Colonoscopy
Colonoscopy is preferred over sigmoidoscopy because it enables examination of the entire colon, and is superior to double-contrast barium enema because of enhanced diagnostic accuracy and therapeutic capability.
Indications
- Colorectal cancer (CRC) screening and surveillance
- Evaluation of lower GI bleeding, change in bowel habits, or iron deficiency anemia
- Diagnosis and monitoring of inflammatory bowel disease (IBD)
- Polypectomy (definitive therapeutic removal)
- Biopsy of suspicious lesions
Technique
- Requires bowel preparation (oral laxatives; polyethylene glycol-based solutions)
- Performed under sedation (propofol preferred; or midazolam + fentanyl)
- Anticoagulants/antiplatelet agents stopped before therapeutic procedures
- Cecum and terminal ileum are intubated; examination of the entire colon is performed
- Polypectomy uses wire snares; flat polyps may be removed by submucosal injection of hypotonic fluid followed by snare
Limitations
- Fails to reach the cecum in up to 10% of cases
- May miss small lesions located at flexures or behind folds
- Requires sedation and bowel preparation (more costly and invasive than FOBT/FIT)
- Post-polypectomy bleeding risk
Colonoscopy Findings
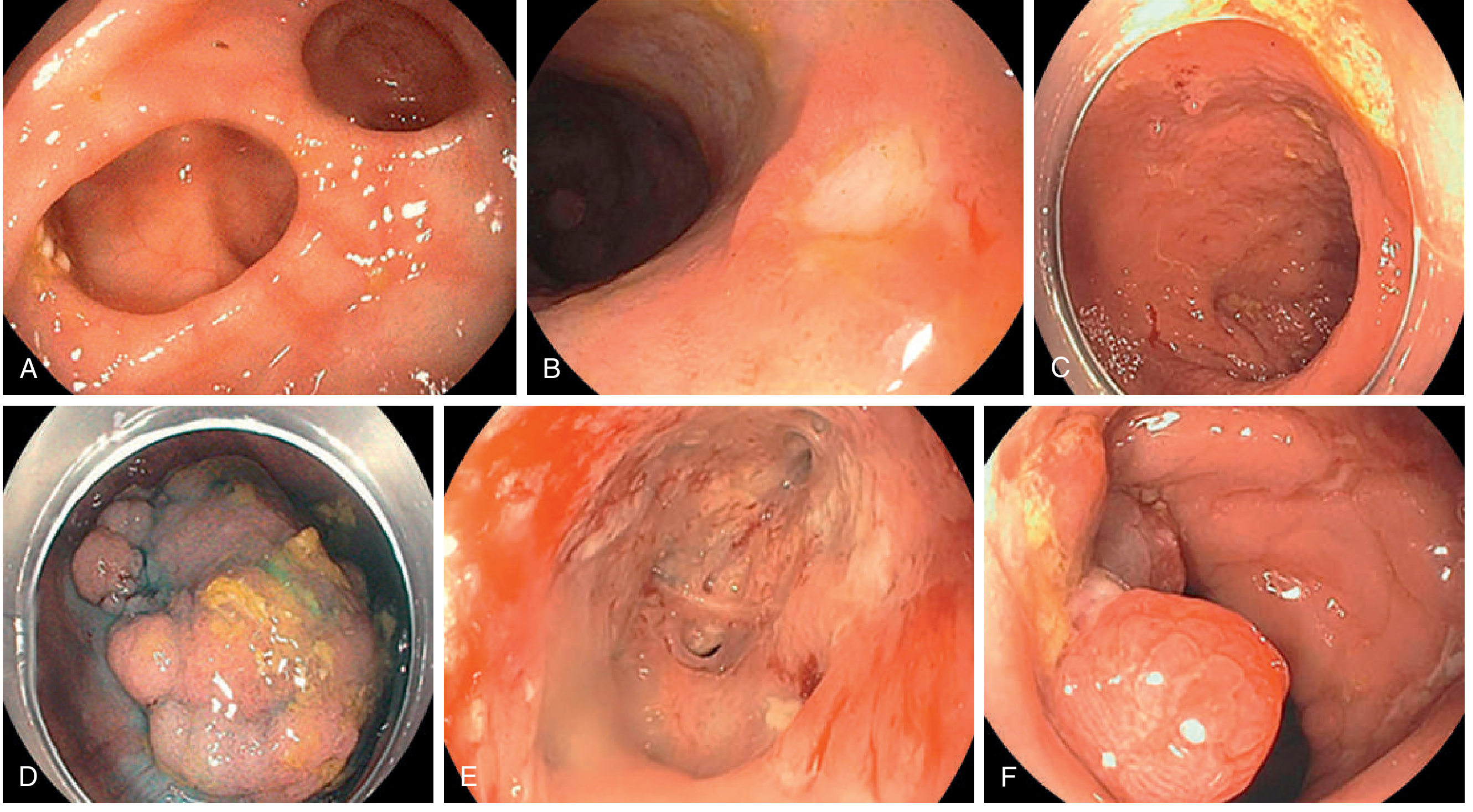
A. Large-mouthed colonic diverticula | B. Colonic ulcer (IBD/Crohn disease) | C. Chronic ulcerative colitis with pseudopolyps | D. Large adenomatous polyp | E. Colonic ulcer with fistula | F. Ulcerated polyp suspicious for malignant transformation
— Goldman-Cecil Medicine
4. Rectosigmoidoscopy (Sigmoidoscopy / Proctoscopy)
Rigid Sigmoidoscopy
For several decades, rigid sigmoidoscopy was the mainstay of endoscopic CRC screening. It detects polyps of all histologic types in 10–15% of asymptomatic persons over age 40. Large-scale prospective studies showed that screening sigmoidoscopy was associated with a 21–38% reduction in mortality from distal CRCs.
Flexible Sigmoidoscopy
Examines the rectum and sigmoid colon (approximately 60 cm from the anus). Requires less bowel preparation than full colonoscopy (enema or low-volume laxative is sufficient). Can be performed without sedation.
Role in Current Practice
Increasing use of full colonoscopy has resulted in a marked reduction in sigmoidoscopy as a primary polyp screening modality in the USA. Sigmoidoscopy is still used for:
- Evaluation of distal symptoms (rectal bleeding, urgency, tenesmus)
- Surveillance in left-sided IBD
- Confirming perianal/rectal pathology (hemorrhoids, proctitis, polyps, fistulas, intussusception)
Proctoscopy
Proctoscopy has an important role in evaluating fecal incontinence. It can detect anorectal pathology such as prolapsing hemorrhoids, intussusception, ulcerative or radiation proctitis. It can be performed independently or during colonoscopy.
— Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Berek & Novak's Gynecology
5. Gastric Juice Examination
Physiology of Gastric Secretion
HCl and pepsinogen are the two principal gastric secretory products. Gastric acid and pepsinogen play a physiologic role in protein digestion; absorption of iron, magnesium, and vitamin B12; and killing ingested bacteria. Acid secretion occurs under:
- Basal conditions — circadian pattern, highest at night, lowest in the morning; regulated by cholinergic (vagal) and histamine input
- Stimulated conditions — three phases:
- Cephalic phase: sight, smell, and taste of food → vagal stimulation
- Gastric phase: nutrients/amino acids → G cell → gastrin → parietal cell activation; stomach distension also stimulates gastrin release
- Intestinal phase: food entering the intestine → luminal distension and nutrient assimilation
Somatostatin (from D cells) inhibits acid secretion by both direct (pericellular) and indirect mechanisms (decreased histamine release from ECL cells, decreased gastrin release from G cells).
Gastric Juice Analysis (Clinical Use)
Gastric juice analysis measures basal acid output (BAO) and peak/maximal acid output (PAO/MAO) after stimulation with pentagastrin. Clinically relevant findings include:
| Parameter | Significance |
|---|---|
| Achlorhydria | Pernicious anemia, atrophic gastritis, gastric cancer |
| Elevated BAO | Zollinger-Ellison syndrome (ZES), duodenal ulcer disease |
| Elevated pentagastrin-stimulated output | Increased secretory capacity (ZES, duodenal ulcer) |
| BAO:MAO ratio > 0.6 | Suggests ZES (autonomous gastrin-driven secretion) |
— Harrison's Principles of Internal Medicine, 22e; Mulholland & Greenfield's Surgery
6. Stool Examination (Coprogram)
Collection
Stool specimens are required for evaluation of diarrhea, malabsorption, detection of infectious agents and occult blood, and diagnosis of many GI conditions. Patient preparation, specimen number, collection frequency, and containers vary by indication.
Macroscopic Examination
| Finding | Clinical significance |
|---|---|
| Normal quantity | 100–200 g/day |
| Large, mushy, foul-smelling, gray, floating stool | Steatorrhea (fat malabsorption) |
| Small, firm, spherical masses (scybala) | Constipation |
| Clay/pale color | Diminished/absent bile (cholestasis), or barium |
| Red stool | Lower GI bleeding; beets can mimic |
| Black, tarry stool (melena) | Upper GI bleeding; also bismuth, iron, charcoal |
| Translucent mucus on formed stool | Spastic constipation, mucous colitis |
| Bloody mucus | Neoplasm or inflammatory processes of the rectum |
| Mucus + pus + blood | Ulcerative colitis, bacillary dysentery, pseudomembranous colitis, intestinal TB |
| Large quantities of mucus (3–4 L/day) | Villous adenoma of the colon |
| Pus (large quantities) | Chronic UC, infectious proctitis, bacillary dysentery; NOT typical of amebiasis |
Microscopic Examination
Fat (Sudan Stain for Steatorrhea)
- A stool aliquot is mixed with 95% ethanol + Sudan III stain
- Neutral fats appear as large orange or red droplets
- ≥60 stained droplets per high-power field (HPF) = steatorrhea
- Procedure is repeated with acetic acid + heat to convert soaps/fatty acids → droplets; up to 100 droplets/HPF after this step is normal
- Patients with pancreatic steatorrhea show greater increases in fatty acids and soaps
Meat Fibers (Creatorrhea)
- Stool + eosin in 10% ethanol
- Rectangular fibers with clearly evident cross-striations
-
10 fibers/HPF suggests maldigestion or hypermotility
Leukocytes
- Small fleck of mucus/liquid stool + methylene blue → differential count
- PMN-predominant: infectious colitis (Salmonella, Campylobacter, Shigella), IBD
- Mononuclear: viral gastroenteritis, early amebiasis
- Fecal calprotectin is a modern alternative marker of intestinal inflammation (used in IBD screening)
Chemical / Immunologic Examination
| Test | Principle | Indication |
|---|---|---|
| Guaiac-based fecal occult blood test (gFOBT) | Peroxidase reaction detects heme | CRC screening; requires dietary restriction |
| Fecal immunochemical test (FIT) | Antibody-based detection of human hemoglobin | CRC screening; no dietary restriction; sensitivity for CRC 79%, specificity 94% |
| Fecal elastase-1 | Enzyme immunoassay | Exocrine pancreatic insufficiency |
| Fecal fat (72-h quantitative) | Chemical extraction | Steatorrhea (gold standard) |
| Fecal calprotectin/lactoferrin | Markers of neutrophil infiltration | IBD vs. IBS differentiation |
| Stool culture | Bacterial growth | Salmonella, Campylobacter, Shigella, C. difficile, E. coli O157:H7 |
| Stool PCR panel | Molecular detection | Simultaneous bacteria, viruses, parasites; results in 1–5 hours |
| Stool Helicobacter pylori antigen | Immunoassay | Diagnosis/eradication confirmation of H. pylori |
| Ova and parasite (O&P) examination | Microscopy | Giardia, Entamoeba histolytica, helminths |
| Stool electrolytes (Na, K) | Osmotic gap = 290 – 2×(Na + K) | Osmotic vs. secretory diarrhea: osmotic gap > 125 mOsm/kg = osmotic cause |
— Goldman-Cecil Medicine; Henry's Clinical Diagnosis and Management by Laboratory Methods
Coprogram Summary Table
| Parameter | Normal | Abnormal finding | Interpretation |
|---|---|---|---|
| Quantity | 100–200 g/day | >300 g | Malabsorption, secretory diarrhea |
| Consistency | Formed | Watery | Infection, osmotic diarrhea |
| Color | Brown | Black/tarry | Upper GI bleed |
| Clay/pale | Cholestasis | ||
| Red | Lower GI bleed | ||
| Mucus | Absent | Present | IBD, infection, IBS, neoplasm |
| Blood | Absent | Overt/occult | Neoplasm, IBD, infection, vascular |
| Odor | Normal | Foul/rancid | Steatorrhea |
| Fat (Sudan III) | < 60 droplets/HPF | ≥ 60 droplets/HPF neutral fat | Steatorrhea |
| Leukocytes | Absent | PMNs present | Invasive bacterial infection, IBD |
| Muscle fibers | Absent | > 10/HPF | Exocrine pancreatic insufficiency |
| pH | 6.0–8.0 | < 5.5 | Carbohydrate malabsorption (fermentation) |
| Occult blood | Negative | Positive | GI bleeding (see above) |
Key References:
- Goldman-Cecil Medicine International Edition, 2-Volume Set (Chapter 120 — GI Endoscopy; Chapter on Stool Examination)
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease (Barium Esophagogram, Barium Enema, Colonoscopy, Sigmoidoscopy)
- Henry's Clinical Diagnosis and Management by Laboratory Methods (Stool Collection and Examination)
- Harrison's Principles of Internal Medicine, 22e (Gastric Acid Secretion Physiology)
Hypoxia
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full answer.
Hypoxia
Definition
Hypoxia is O₂ deficiency at the tissue level — a state in which the oxygen supply to tissues is insufficient for normal metabolic needs. The term is more precise than anoxia (complete absence of O₂), since tissue O₂ is rarely zero. Hypoxemia is a related but distinct term: it refers specifically to a reduced arterial PaO₂. Hypoxemia is a major cause of hypoxia, but not the only one.
Hypoxia may be thought of as the functional equivalent of ischemia. It refers to a lack of or misuse of oxygen at the tissue level. Hypoxemia refers to the blood's oxygen content — when a patient's PaO₂ and SaO₂ are low, the patient is hypoxemic. — Fishman's Pulmonary Diseases and Disorders
Classification — Four Traditional Types
| Type | Alternative name | PaO₂ | Mechanism |
|---|---|---|---|
| Hypoxemic (hypoxic) hypoxia | Hypoxemia | ↓ | Reduced arterial PO₂ — less O₂ loaded onto hemoglobin |
| Anemic hypoxia | — | Normal | Normal PaO₂, but hemoglobin quantity or function reduced → ↓ O₂ content |
| Ischemic (stagnant) hypoxia | Circulatory hypoxia | Normal | Blood flow to tissue so low that O₂ delivery is inadequate despite normal PaO₂ and Hb |
| Histotoxic hypoxia | — | Normal | O₂ delivery adequate, but cells cannot utilize O₂ (e.g., cyanide poisoning) |
The four categories are: (1) hypoxemia, in which the PO₂ of the arterial blood is reduced; (2) anemic hypoxia, in which the arterial PO₂ is normal but the amount of hemoglobin available to carry O₂ is reduced; (3) ischemic or stagnant hypoxia, in which the blood flow to a tissue is so low that adequate O₂ is not delivered despite a normal PO₂ and Hb concentration; and (4) histotoxic hypoxia, in which the amount of O₂ delivered is adequate but, because of a toxic agent, the tissue cells cannot make use of the O₂ supplied. — Ganong's Review of Medical Physiology, 26th Edition
Causes of Hypoxemia (Type 1 — Hypoxic Hypoxia)
The driving force for O₂ diffusion across the alveolar-capillary barrier depends on the alveolar PO₂ (PAO₂). Arterial hypoxemia results from five pathophysiologic mechanisms:
1. Reduced Inspired O₂ Tension (↓FiO₂)
- High altitude (↓barometric pressure → ↓PO₂)
- Confined spaces, smoke-filled rooms
2. Alveolar Hypoventilation
- ↓PAO₂ and resultant ↓PaO₂, with accompanying hypercapnia
- Examples: narcotic/sedative overdose (↓central drive), obesity-hypoventilation syndrome, obstructive sleep apnea, neuromuscular disease, abdominal compartment syndrome
3. Diffusion Impairment
- Increased barrier across alveolar-capillary membrane → detected as ↓DLco
- Examples: pulmonary fibrosis, interstitial pneumonias
- Often coexists with V̇/Q̇ mismatch; most prominent during exercise or at altitude
4. Ventilation-Perfusion (V̇/Q̇) Mismatch
- Focal areas of diminished ventilation with preserved perfusion
- Most common mechanism in clinical practice
- Examples: COPD, asthma, interstitial edema, pneumonia
- Responds to supplemental oxygen (FiO₂ titration corrects hypoxemia)
- Reflex hypoxic pulmonary vasoconstriction (HPV) reduces mismatch; widespread HPV → pulmonary hypertension → cor pulmonale
5. Right-to-Left Shunt
- Fraction of pulmonary blood bypasses ventilated alveoli
- Examples: alveolar filling (cardiogenic edema, pneumonia, drowning, atelectasis), anatomic shunts (ASD, pulmonary AV malformations)
- Key feature: hypoxemia persists despite 100% FiO₂ (when shunt fraction >20–25%)
— Fishman's Pulmonary Diseases and Disorders; Costanzo Physiology, 7th Edition
Causes Summary Table
| Cause | Mechanism | PaO₂ | Notes |
|---|---|---|---|
| Low FiO₂ / altitude | ↓ Inspired O₂ | ↓ | Corrects with supplemental O₂ |
| Hypoventilation | ↓ PAO₂ | ↓ | + Hypercapnia |
| Diffusion impairment | ↓ Membrane transfer | ↓ | Worsens with exercise |
| V̇/Q̇ mismatch | Uneven ventilation | ↓ | Most common clinical cause |
| Shunt (R→L) | Bypassed ventilation | ↓ | Minimal O₂ response |
| ↓ Cardiac output | ↓ Tissue blood flow | Normal | Stagnant hypoxia |
| Anemia | ↓ Hb concentration | Normal | ↓ O₂-carrying capacity |
| CO poisoning | CO occupies Hb binding sites | Normal | ↓ O₂ content; left shift of curve |
| Cyanide poisoning | ↓ O₂ utilization | Normal | Histotoxic; normal venous O₂ |
Cellular Response to Hypoxia — Hypoxia-Inducible Factors (HIFs)
Hypoxia activates a fundamental transcriptional program mediated by HIF (hypoxia-inducible factors) — a "master switch" for the body's response to oxygen deprivation.
Mechanism
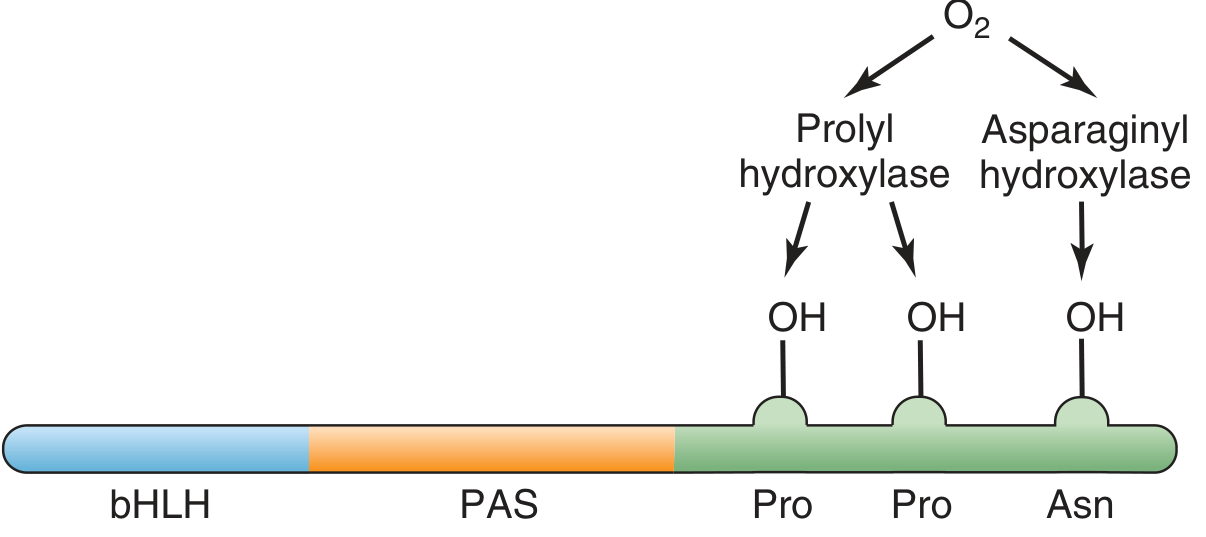
- HIFs are heterodimers of HIF-α and HIF-β subunits
- Under normoxia: HIF-1α is hydroxylated (prolyl and asparaginyl hydroxylases require O₂) → recognized by VHL protein → ubiquitinated and rapidly degraded
- Under hypoxia: hydroxylases are inactive → HIF-1α accumulates → dimerizes with HIF-1β → complex translocates to nucleus → binds hypoxia response elements (HREs) on target genes
Genes Activated by HIF-1
| Gene product | Effect |
|---|---|
| VEGF (vascular endothelial growth factor) | Stimulates angiogenesis — new capillary formation |
| Erythropoietin (EPO) | Stimulates red cell production in bone marrow |
| Glycolytic enzymes | Switch from oxidative phosphorylation to anaerobic glycolysis |
| Nitric oxide synthase | Increases NO → pulmonary vasodilation |
| Mitochondrial regulators | Optimize O₂ utilization under hypoxic conditions |
HIFs are found in virtually all oxygen-breathing species. The HIFs serve as a "master switch" that permits the body to respond appropriately to hypoxia. — Guyton and Hall Textbook of Medical Physiology
Clinical Manifestations
Acute Hypoxia
| System | Signs and Symptoms |
|---|---|
| Neurological | Impaired judgment, drowsiness, disorientation, loss of time sense, excitement, headache, dulled pain sensation — resembles alcohol intoxication |
| Respiratory | Tachypnea, dyspnea, hyperpnea (↑ depth and rate of breathing via carotid body chemoreceptors) |
| Cardiovascular | Tachycardia, ↑ cardiac output, hypertension (severe hypoxia); later hypotension and bradycardia |
| GI | Anorexia, nausea, vomiting |
| Cyanosis | Central cyanosis (bluish mucous membranes, lips) when SaO₂ <85–90% |
The brain is affected first. A sudden drop in inspired PO₂ to <20 mmHg (e.g., rapid cabin decompression above 16,000 m) causes loss of consciousness in 10–20 seconds and death in 4–5 minutes.
Chronic Hypoxia
Patients with chronic hypoxia often have minimal symptoms due to compensatory mechanisms:
- Polycythemia (↑ erythropoietin → ↑ red cell mass)
- Right heart strain → cor pulmonale
- Finger clubbing (chronic tissue ischemia)
- Peripheral cyanosis
EEG in Severe Hypoxia (Neurological)
- Alpha coma: monorhythmic alpha-frequency EEG in comatose patient; unreactive to stimuli; frontal predominance — poor prognosis
- Burst suppression: bursts of mixed-frequency activity with intervening flat periods
- Periodic pattern: generalized spikes recurring at ~1–2/second; often with myoclonic jerks
— Ganong's Review of Medical Physiology; Bradley and Daroff's Neurology in Clinical Practice; Fishman's Pulmonary Diseases and Disorders
Physiological Responses and Compensation
Immediate (seconds–minutes)
- Chemoreceptor (carotid body) activation → ↑ ventilation
- ↑ Heart rate and cardiac output
- Sympathoadrenal stimulation
Short-term (hours–days)
- Hypoxic pulmonary vasoconstriction (HPV) — redirects blood from poorly ventilated to well-ventilated lung regions
- HIF-1 pathway activation
Long-term Acclimatization (days–weeks)
- ↑ Erythropoietin → ↑ red cell production → polycythemia → ↑ O₂-carrying capacity
- ↑ 2,3-DPG in erythrocytes → right shift of Hb-O₂ dissociation curve → ↑ O₂ unloading to tissues
- ↑ Capillary density (angiogenesis via VEGF)
- ↑ Respiratory alkalosis (hyperventilation-driven)
Effects of Altitude
| Altitude | Alveolar PO₂ | Effect |
|---|---|---|
| Sea level | ~100 mmHg | Normal |
| 3,000 m (10,000 ft) | ~60 mmHg | Sufficient hypoxic drive to ↑ ventilation |
| 3,700 m | — | Mental symptoms (irritability) in unacclimatized persons |
| 3,500 m | — | Severe hypoxic symptoms |
| >6,100 m (20,000 ft) | — | Consciousness usually lost |
Oxygen Therapy
Indications (Acute)
- Documented hypoxemia: PaO₂ <60 mmHg or SaO₂ <90%
- Acute situation where hypoxemia is suspected (respiratory distress)
- Severe trauma, severe acute anemia, acute MI with hypoxemia
- Low cardiac output with metabolic acidosis
- Hypotension (systolic BP <100 mmHg)
Targets
- SaO₂ 92–96% is reasonable for most hypoxemic patients at sea level with normal baseline lung function
- Higher targets may be appropriate in profound anemia (maximize O₂ content before transfusion)
- In COPD with CO₂ retention: lower target (SaO₂ 88–92%) to avoid suppressing hypoxic drive
Response to Supplemental O₂ by Mechanism
| Mechanism | Response to O₂ |
|---|---|
| Hypoventilation | Good, but hypercapnia persists — must restore ventilation |
| V̇/Q̇ mismatch | Responds well |
| Diffusion impairment | Responds well |
| Shunt (R→L) | Poor — hypoxemia persists when shunt >20–25% |
| Anemic hypoxia | Modest benefit only (dissolved O₂ slightly increases content) |
| Histotoxic (cyanide) | No benefit — cells cannot utilize O₂ |
Key References:
- Ganong's Review of Medical Physiology, 26th Edition — Classification and types of hypoxia; effects on brain; effects of altitude
- Guyton and Hall Textbook of Medical Physiology — HIF master switch; acclimatization
- Fishman's Pulmonary Diseases and Disorders — Pathophysiology of arterial hypoxemia; clinical manifestations; oxygen therapy
- Costanzo Physiology, 7th Edition — Causes of hypoxia table; CO/cyanide mechanisms
- Medical Physiology (Boron & Boulpaep) — HIF-1α molecular mechanism and hydroxylation
- Bradley and Daroff's Neurology in Clinical Practice — EEG patterns in hypoxic brain injury
Questions 1. Female reproductive diseases. A) Congenital (developmental) disorders B) Inflammatory diseases (Infections) C) Hormonal / functional disorders 2. Gestational and placental disorders a) Implantation and early pregnancy disorders b) Hypertensive disorders of pregnancy c) Metabolic / systemic gestational disorders d) Fetal growth and development disorders
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
This is a shared conversation. Sign in to Orris to start your own chat.