Here is a comprehensive guide to 10 common heart diseases with their characteristic ECG changes and illustrative ECG images.
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is the comprehensive guide, drawn directly from Harrison's Principles of Internal Medicine (22nd ed.), Tintinalli's Emergency Medicine, Braunwald's Heart Disease, The Washington Manual, Fuster and Hurst's The Heart, and Goldman-Cecil Medicine.
A Guide to ECG Changes in 10 Common Heart Diseases
1. ST-Elevation Myocardial Infarction (STEMI)
Mechanism
Acute transmural ischemia shifts the ST vector toward the outer (epicardial) layer of the affected zone, creating a "current of injury." This produces ST elevations and, in the earliest phase, tall hyperacute T waves over the ischemic zone.
Characteristic ECG Changes
- Hyperacute T waves - tall, broad, peaked; earliest finding (minutes after onset)
- ST elevation - convex ("tombstone") shape in the territory of occlusion
- Reciprocal ST depression - in leads opposite the infarct territory
- Pathologic Q waves - develop within hours to days; indicate necrosis of sufficient myocardial tissue
- T-wave inversions - follow ST elevation as infarct evolves
Localization by Lead
| Territory | Culprit Artery | Leads with ST Elevation |
|---|---|---|
| Anterior | LAD | V1-V4, I, aVL |
| Inferior | RCA or LCx | II, III, aVF |
| Lateral | LCx | I, aVL, V5-V6 |
| Posterior | RCA or LCx | Reciprocal changes V1-V3 (tall R, ST depression) |
| Right ventricular | Proximal RCA | V1, V4R |
ECG Images
Anterior STEMI (acute and evolving) - leads I, II, III, aVR, aVL, aVF, V2, V4, V6:
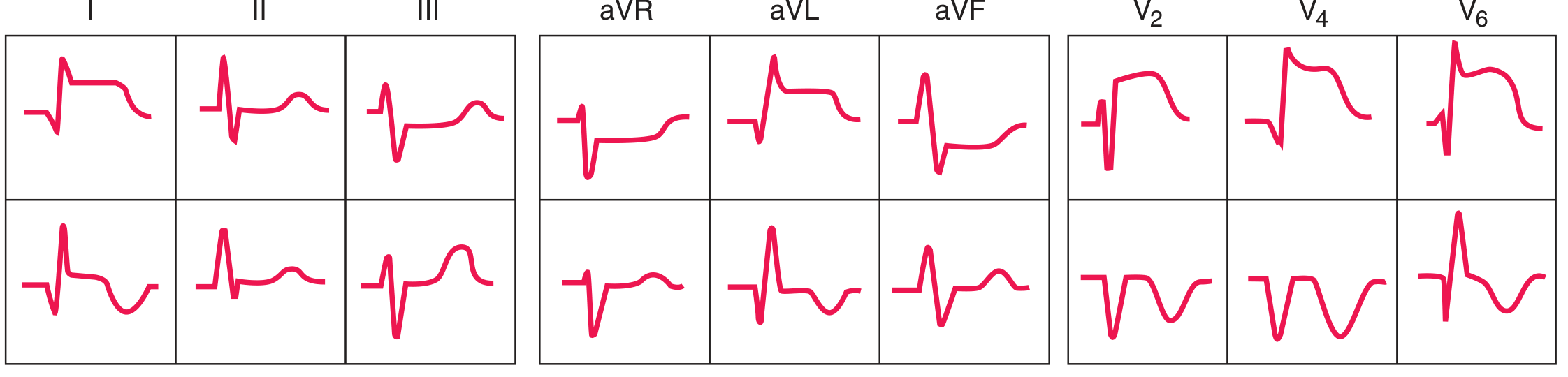
Acute (top row) and evolving (bottom row) anterior STEMI. Note ST elevation in I, aVL and precordial leads, with reciprocal ST depressions in II, III, aVF. - Harrison's Principles of Internal Medicine, 22nd ed.
Inferior STEMI (acute and evolving):
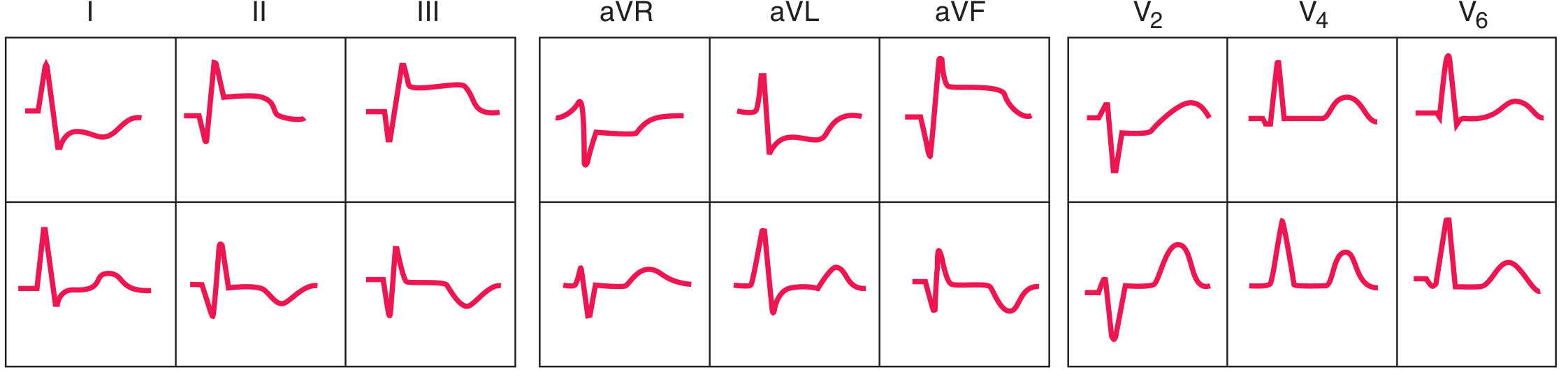
Acute (top row) and evolving (bottom row) inferior STEMI. ST elevation in II, III, aVF with reciprocal ST depression in I, aVL and anterior precordial leads. - Harrison's Principles of Internal Medicine, 22nd ed.
Subendocardial vs. transmural ischemia diagram:

Panel A: subendocardial ischemia - ST vector points inward, overlying leads record ST depression. Panel B: transmural/epicardial ischemia - ST vector points outward, overlying leads record ST elevation. - Harrison's Principles of Internal Medicine, 22nd ed.
Wellens T-wave sign (severe LAD stenosis):

Deep, symmetric T-wave inversions in V1-V6 (Wellens sign). This pattern indicates high-grade LAD stenosis and carries high risk of impending anterior STEMI. - Harrison's Principles of Internal Medicine, 22nd ed.
2. Atrial Fibrillation (AF)
Mechanism
Multiple small, chaotic atrial re-entry circuits fire at rates >600 bpm. There is no coordinated atrial depolarization. The AV node acts as a filter, passing impulses irregularly to the ventricles.
Characteristic ECG Changes
- Absent P waves - replaced by chaotic, irregular fibrillatory baseline (best seen in V1)
- Irregularly irregular ventricular rhythm - the hallmark; no two R-R intervals are equal
- Variable ventricular rate - typically 120-170 bpm when AV node is unaffected; can exceed 200 bpm with accessory pathway
- Narrow QRS complexes - unless pre-existing bundle branch block or accessory pathway
ECG Features Table (from Tintinalli's Emergency Medicine)
- Absence of discernible P waves with flat or chaotic isoelectric baseline
- QRS complexes narrow unless pre-existing bundle branch block or preexcitation syndrome
- Irregularly irregular ventricular rhythm
ECG Image
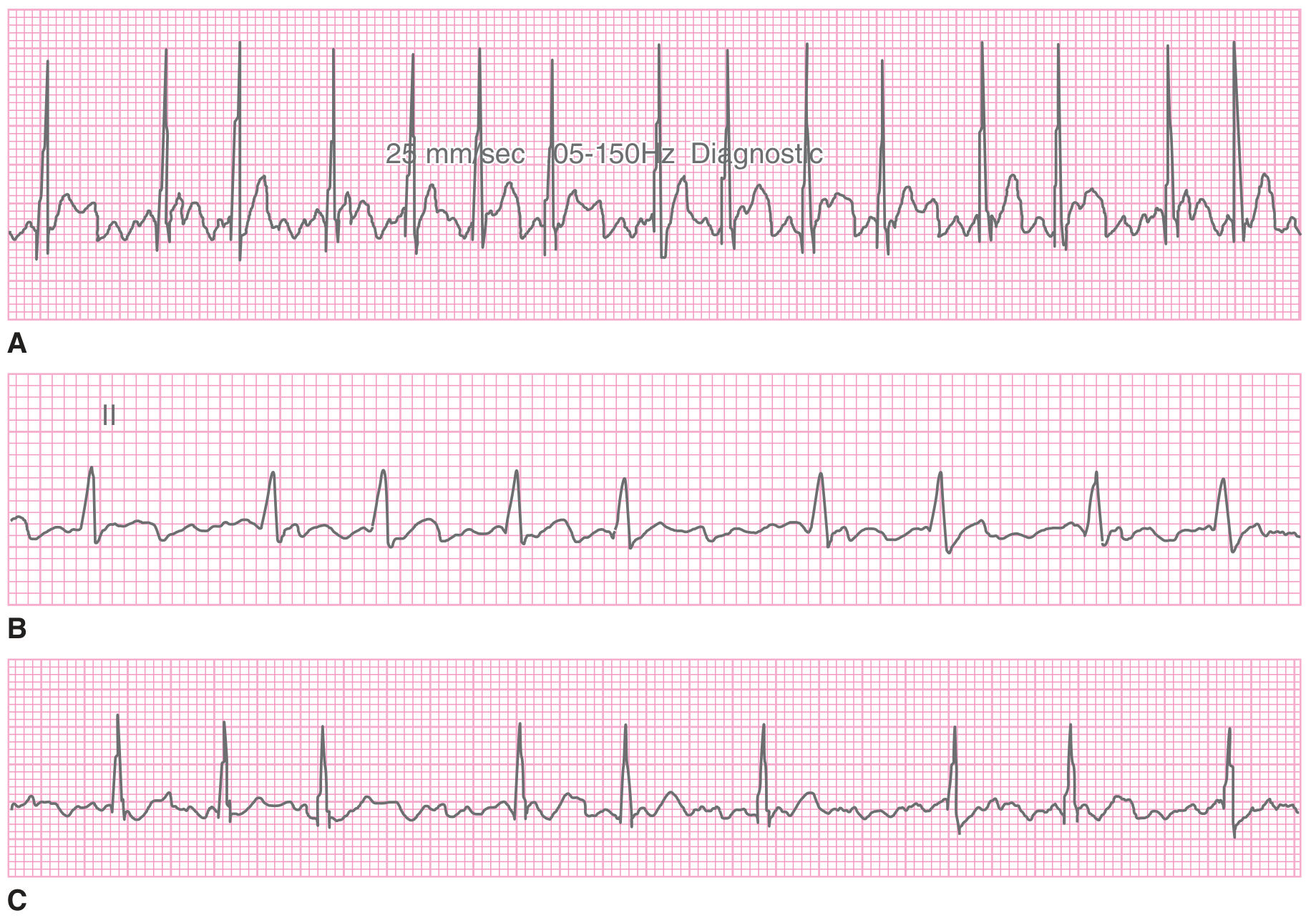
Three examples of atrial fibrillation. All show the hallmark irregularly irregular ventricular response with absent P waves. Strip A has rapid ventricular response; B and C show slower rates, possibly from AV nodal disease or medications. - Tintinalli's Emergency Medicine, 9th ed.
3. Atrial Flutter
Mechanism
A single, large macroreentrant circuit in the right atrium circles continuously at ~300 bpm, producing uniform flutter waves. Conduction to the ventricles is filtered by the AV node in fixed or variable ratios.
Characteristic ECG Changes
- Sawtooth flutter waves - uniform, negatively directed "F waves" at ~300 bpm, best seen in leads II, III, aVF and V1
- Regular ventricular rhythm - determined by the AV conduction ratio
- 2:1 AV block - most common; ventricular rate ~150 bpm (a regular narrow-complex tachycardia at 150 bpm should immediately raise suspicion for flutter)
- 3:1 or 4:1 AV block - ventricular rates of ~100 and ~75 bpm respectively
- No isoelectric baseline between flutter waves - they merge continuously
Key Point
A regular narrow-complex tachycardia at exactly 150 bpm (±5 bpm) is atrial flutter with 2:1 block until proven otherwise.
4. AV Heart Blocks (1st, 2nd, 3rd Degree)
Mechanism
Delay or interruption of conduction between the atria and ventricles at or below the AV node.
First-Degree AV Block
- PR interval >200 ms on every beat; all P waves conduct
- No dropped beats
- Usually benign; may occur in trained athletes, vagal tone, digoxin, or inferior MI
Second-Degree AV Block
Mobitz Type I (Wenckebach):
- Progressive PR prolongation with each successive beat until a P wave fails to conduct (dropped QRS)
- RR intervals shorten progressively before the dropped beat
- Group beating pattern on the rhythm strip
- Block usually within the AV node; benign prognosis; rarely progresses to complete block
Mobitz Type II:
- Abrupt failure to conduct without prior PR lengthening
- PR interval constant before the dropped beat
- Often associated with bundle branch block
- Block below the AV node; unpredictable - may progress suddenly to complete heart block
2:1 AV Block:
- Every other P wave fails to conduct; difficult to distinguish Mobitz I from II
- Presence of bundle branch block on conducted beats favors Mobitz II (infranodal)
Third-Degree (Complete) AV Block
- Complete dissociation between atria and ventricles
- P waves and QRS complexes march independently ("AV dissociation, A > V rate")
- QRS complex morphology depends on escape pacemaker location:
- Junctional escape (narrow QRS, 40-60 bpm) if block at AV node level
- Ventricular escape (wide QRS, 20-40 bpm) if block at bundle branch level
ECG Image

A: First-degree AV block - PR >200 ms, no dropped beats. B: Second-degree Mobitz I (Wenckebach) - progressive PR prolongation then dropped beat, "group beating." C: Second-degree Mobitz II - abrupt dropped beat, constant PR. D: Advanced AV block with multiple consecutive non-conducted P waves. E: Third-degree complete heart block (V1) - complete AV dissociation with independent atrial and ventricular activity. - Washington Manual of Medical Therapeutics.
5. Acute Pericarditis
Mechanism
The pericardium itself is electrically silent. ECG changes reflect subepicardial myocardial inflammation, causing diffuse repolarization abnormalities. PR depression results from atrial epicardial involvement and augmented atrial repolarization.
Characteristic ECG Changes (4 Stages)
| Stage | Timing | ECG Finding |
|---|---|---|
| 1 | Hours of onset | Diffuse ST elevation (concave, saddle-shaped) in all leads except aVR and V1; PR depression in most leads; PR elevation in aVR ("knuckle sign") |
| 2 | Days | ST and PR segments return to baseline |
| 3 | Days-weeks | Diffuse T-wave inversions (without Q waves) |
| 4 | Weeks-months | ECG normalizes |
Distinguishing from STEMI
- ST elevation in pericarditis is diffuse (nearly all leads), concave/saddle-shaped, with PR depression
- STEMI shows focal, convex ST elevation in a coronary territory with reciprocal ST depression in opposite leads and may form Q waves
- Pericarditis does not cause reciprocal ST depression (except in aVR, which shows ST depression)
- Less than 60% of patients progress through all four stages; a normal ECG does not exclude pericarditis
ECG Image
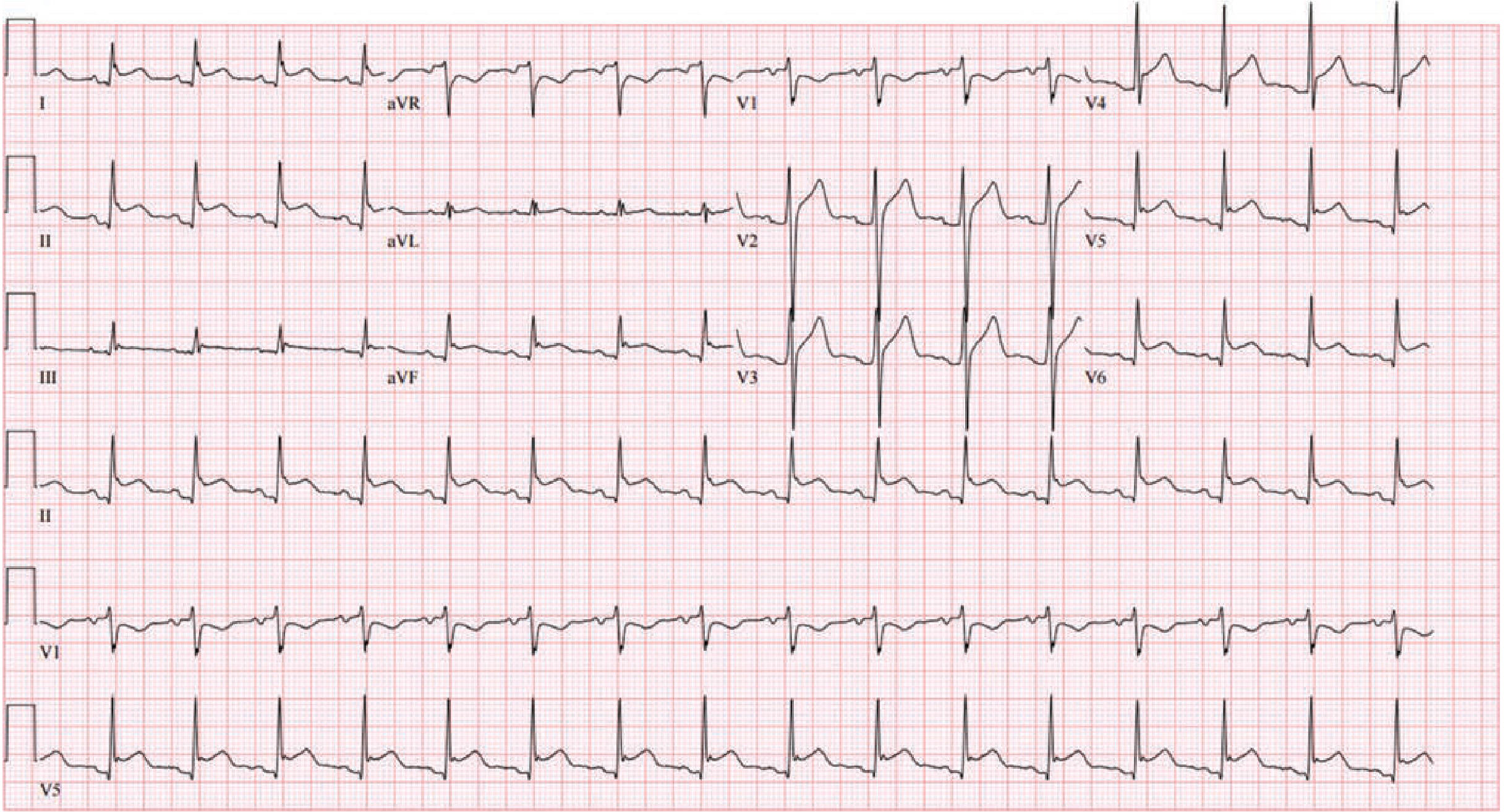
Stage 1 acute pericarditis: diffuse, concave ST elevation across non-contiguous leads in a non-coronary distribution. PR-segment depression is visible in leads II, V5, and V6. Lead aVR shows the characteristic PR elevation ("knuckle sign") with ST depression. Note the absence of Q waves or reciprocal changes as would be expected with STEMI. - Fuster and Hurst's The Heart, 15th ed.
6. Ventricular Tachycardia (VT)
Mechanism
A reentrant circuit or abnormal automaticity arises within the ventricular myocardium, below the bundle of His. Activation spreads through abnormal (non-Purkinje) pathways, producing a wide QRS.
Characteristic ECG Changes
- Wide QRS complex (≥120 ms), typically >140 ms
- Regular tachycardia at 100-250 bpm
- AV dissociation - P waves march at a different rate from QRS; pathognomonic when present
- Fusion beats - hybrid QRS from simultaneous sinus and ventricular activation; confirms VT
- Capture beats - rare narrow QRS during tachycardia when sinus impulse captures ventricle; confirms VT
- Concordance - all precordial leads with QRS deflection in same direction (positive or negative concordance); strongly favors VT
- Extreme axis deviation ("northwest axis," -90° to ±180°)
- QRS morphology: RBBB-like pattern with monophasic R or QR in V1; LBBB-like pattern with R>S in V1
Distinguishing VT from SVT with Aberrancy (Brugada Criteria)
VT is diagnosed if ANY one of these four criteria is present (checked in sequence):
- Absence of RS complexes in all precordial leads
- R-to-S nadir interval >100 ms in any precordial lead
- AV dissociation present
- Morphologic criteria for VT in V1/V6
Clinical rule: Any hemodynamically unstable wide-complex tachycardia should be treated as VT.
7. Ventricular Fibrillation (VF)
Mechanism
Completely disorganized depolarization of multiple small ventricular areas without any coordinated mechanical activity. Results in immediate loss of cardiac output.
Characteristic ECG Changes
- Completely chaotic, irregular waveform with no identifiable P waves, QRS complexes, or T waves
- No discernible organized rhythm of any kind
- Variable amplitude: described as fine (low amplitude), intermediate, or coarse (higher amplitude, sometimes resembling VT)
ECG Image
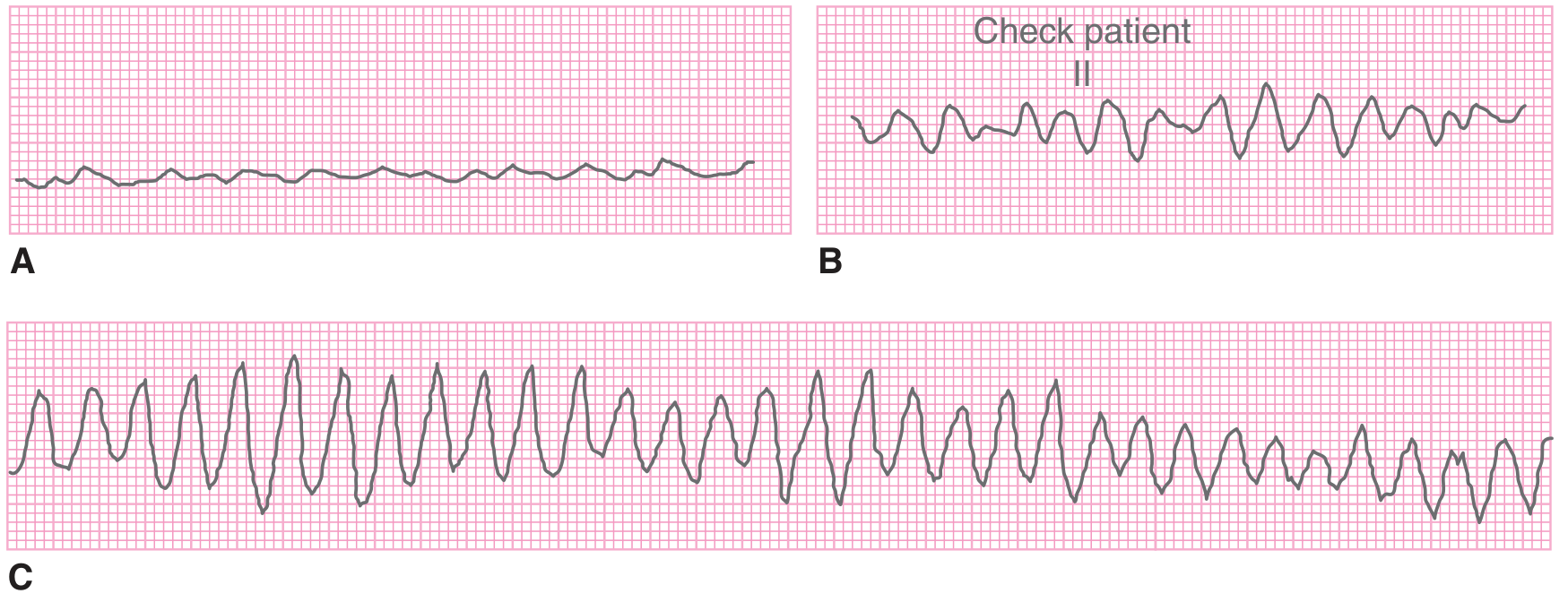
Three examples of ventricular fibrillation. A: Fine amplitude VF - low-amplitude chaotic undulations with no organized activity. B: Coarse amplitude VF - higher amplitude, may be mistaken for a rhythm. C: Coarse VF that mimics ventricular tachycardia. Immediate defibrillation is required regardless of amplitude. - Tintinalli's Emergency Medicine, 9th ed.
8. Wolff-Parkinson-White (WPW) Syndrome
Mechanism
An accessory conduction pathway (Bundle of Kent) bypasses the AV node, creating a direct atria-to-ventricle connection. During sinus rhythm, the ventricle is activated simultaneously via both the accessory pathway (earlier, slower cell-to-cell conduction) and the normal AV node/His-Purkinje system. The resulting QRS is a fusion of both.
Characteristic ECG Changes During Sinus Rhythm (Classic Triad)
| Feature | Finding | Mechanism |
|---|---|---|
| Short PR interval | <120 ms | Accessory pathway bypasses AV nodal delay |
| Delta wave | Slurred initial QRS upstroke | Early ventricular activation via accessory pathway |
| Wide QRS | Slightly prolonged (fused complex) | Combination of accessory + normal activation |
- Secondary ST-T changes discordant (opposite) to the delta wave and QRS direction
- Delta waves may mimic Q waves, simulating myocardial infarction
Tachyarrhythmias in WPW
- Orthodromic AVRT (65%) - narrow QRS, 160-220 bpm, no delta wave during tachycardia; indistinguishable from AVNRT
- Antidromic AVRT (5-10%) - wide QRS, 160-220 bpm; mimics VT
- AF with WPW (25%) - irregular, very rapid (>200 bpm), wide QRS with varying morphology and delta waves; life-threatening
Critical Note
AV nodal blocking agents (adenosine, beta-blockers, calcium channel blockers, digoxin, amiodarone) are contraindicated in AF with WPW - they may enhance accessory pathway conduction, precipitating VF.
9. Hypertrophic Cardiomyopathy (HCM)
Mechanism
Massive myocardial hypertrophy (particularly septal) increases total myocardial mass, altering depolarization vectors and repolarization patterns. The ECG is abnormal in the vast majority of patients with HCM.
Characteristic ECG Changes
- Left ventricular hypertrophy (LVH) voltage criteria - tall R waves in lateral leads (I, aVL, V5-V6) and/or deep S waves in right precordial leads (V1-V3); Sokolow-Lyon criteria: S in V1 + R in V5 or V6 >35 mm
- Deep, narrow ("dagger-like") Q waves in lateral leads (I, aVL, V5-V6) and/or inferior leads - due to septal hypertrophy and abnormal septal depolarization (not infarction); a classic finding
- Left axis deviation
- ST depression and T-wave inversions in lateral leads
- Left atrial enlargement - broad, bifid P wave (P mitrale) in II; biphasic P wave in V1
- Giant T-wave inversions in apical HCM (Yamaguchi syndrome) - massive, symmetric T-wave inversions across all precordial leads, sometimes with tall R waves
Key Point
The combination of LVH voltage and deep narrow Q waves in the lateral leads in a young patient without prior MI is highly suggestive of HCM. The ECG is abnormal in >90% of HCM patients.
10. Pulmonary Embolism (PE)
Mechanism
Acute right ventricular pressure overload from obstruction of the pulmonary vasculature causes right heart strain. This shifts the cardiac electrical axis rightward and anteriorly, altering depolarization and repolarization.
Characteristic ECG Changes
Most common (but nonspecific):
- Sinus tachycardia - most frequent ECG finding in PE
- Non-specific ST-T wave changes - present in the majority
Classic (but uncommon, ~20% of cases):
- S1Q3T3 pattern - deep S wave in lead I, Q wave in lead III, inverted T wave in lead III; indicates acute right heart strain
- New right bundle branch block (RBBB) - complete or incomplete; new onset in clinical context of PE
- Right axis deviation
Other right heart strain findings:
- T-wave inversions in V1-V4 (anterior right ventricular ischemia pattern) - more common than S1Q3T3 in massive PE
- Right atrial enlargement - tall peaked P waves (P pulmonale) in lead II
- Low voltage or electrical alternans if pericardial effusion is also present
- Sinus tachycardia remains the most sensitive ECG abnormality
Key Point
A normal ECG does not exclude PE. Sinus tachycardia alone with the right clinical scenario should prompt immediate evaluation. The S1Q3T3 pattern, while classic in textbooks, is present in only ~20% of confirmed PE cases. T-wave inversions in V1-V4 in the context of acute dyspnea and hypoxia are actually a more sensitive marker of right ventricular strain.
Summary Table
| Condition | Key ECG Finding(s) | Hallmark Feature |
|---|---|---|
| STEMI | Focal convex ST elevation + reciprocal ST depression | Territory-specific; evolves to Q waves |
| Atrial Fibrillation | No P waves, irregularly irregular RR | Chaotic baseline, no two RR intervals equal |
| Atrial Flutter | Sawtooth flutter waves ~300 bpm | Regular 2:1 rate ~150 bpm |
| 1st-degree AV block | PR >200 ms, all beats conduct | Prolonged PR, no dropped beats |
| 2nd-degree Mobitz I | Progressive PR lengthening then dropped beat | Group beating, Wenckebach cycles |
| 2nd-degree Mobitz II | Constant PR then sudden dropped beat | Abrupt block, often with BBB |
| 3rd-degree AV block | Complete AV dissociation | P and QRS march independently |
| Acute Pericarditis | Diffuse concave ST elevation + PR depression | Saddle-shaped, all leads except aVR |
| Ventricular Tachycardia | Wide QRS tachycardia + AV dissociation | Fusion/capture beats pathognomonic |
| Ventricular Fibrillation | Chaotic, no QRS, immediate cardiac arrest | No organized waveform of any kind |
| WPW | Short PR + delta wave + wide QRS | Pre-excitation triad in sinus rhythm |
| HCM | LVH + deep narrow lateral Q waves | "Dagger" Q waves without prior MI |
| Pulmonary Embolism | Sinus tachycardia; S1Q3T3; T inversions V1-V4 | Right heart strain pattern |
Sources: Harrison's Principles of Internal Medicine 22nd ed. | Tintinalli's Emergency Medicine 9th ed. | Braunwald's Heart Disease | The Washington Manual of Medical Therapeutics | Fuster and Hurst's The Heart, 15th ed. | Goldman-Cecil Medicine
Make a quick-reference PDF card of ECG changes
Reading File
Running Command
ls /home/daytona/workspace/ 2>/dev/null || echo "workspace empty or missing"
Running Command
mkdir -p /home/daytona/workspace/ecg-reference && python3 -c "import reportlab; print('reportlab ok')" && python3 -c "from reportlab.lib import colors; print('colors ok')"
Writing File
~/ecg-reference/build_ecg_card.py
"""
ECG Quick-Reference Card Generator
Two-page A4 landscape PDF
"""
from reportlab.lib.pagesizes import A4, landscape
from reportlab.lib import colors
from reportlab.lib.units import mm
from reportlab.platypus import (
SimpleDocTemplate, Table, TableStyle, Paragraph, Spacer,
HRFlowable, KeepTogether
)
from reportlab.lib.styles import ParagraphStyle
from reportlab.lib.enums import TA_CENTER, TA_LEFT
from reportlab.pdfbase import pdfmetrics
from reportlab.pdfbase.ttfonts import TTFont
import os
OUTPUT = "/home/daytona/workspace/ecg-reference/ECG_Quick_Reference.pdf"
# ── Colour palette ──────────────────────────────────────────────────────────
NAVY = colors.HexColor("#0D2B55")
CRIMSON = colors.HexColor("#C0392B")
TEAL = colors.HexColor("#117A8B")
AMBER = colors.HexColor("#D4860B")
GREEN = colors.HexColor("#1A7A4A")
PURPLE = colors.HexColor("#6C3483")
SLATE = colors.HexColor("#2C3E50")
LTGREY = colors.HexColor("#F0F3F6")
MIDGREY = colors.HexColor("#D5D8DC")
WHITE = colors.white
BLACK = colors.black
# ── Styles ───────────────────────────────────────────────────────────────────
def make_styles():
base = {"fontName": "Helvetica", "leading": 10}
return {
"title": ParagraphStyle("title", fontName="Helvetica-Bold",
fontSize=17, textColor=WHITE,
alignment=TA_CENTER, leading=22),
"subtitle": ParagraphStyle("subtitle", fontName="Helvetica",
fontSize=8.5, textColor=colors.HexColor("#A9CCE3"),
alignment=TA_CENTER, leading=11),
"section_hdr": ParagraphStyle("section_hdr", fontName="Helvetica-Bold",
fontSize=9, textColor=WHITE,
alignment=TA_CENTER, leading=11),
"condition": ParagraphStyle("condition", fontName="Helvetica-Bold",
fontSize=8.2, textColor=NAVY, leading=10),
"body": ParagraphStyle("body", fontName="Helvetica",
fontSize=7.2, textColor=SLATE, leading=9.5),
"bold_body": ParagraphStyle("bold_body", fontName="Helvetica-Bold",
fontSize=7.2, textColor=SLATE, leading=9.5),
"highlight": ParagraphStyle("highlight", fontName="Helvetica-BoldOblique",
fontSize=7, textColor=CRIMSON, leading=9),
"footer": ParagraphStyle("footer", fontName="Helvetica",
fontSize=6.5, textColor=colors.grey,
alignment=TA_CENTER, leading=9),
"col_hdr": ParagraphStyle("col_hdr", fontName="Helvetica-Bold",
fontSize=7.5, textColor=WHITE,
alignment=TA_CENTER, leading=9),
}
S = make_styles()
def p(text, style="body"):
return Paragraph(text, S[style])
def bullet(items, style="body"):
"""Render a list of strings as bullet paragraphs joined by line breaks."""
lines = "<br/>".join(f"• {i}" for i in items)
return Paragraph(lines, S[style])
# ── Data ─────────────────────────────────────────────────────────────────────
CONDITIONS = [
{
"no": "01",
"name": "STEMI",
"full": "ST-Elevation MI",
"color": CRIMSON,
"rhythm": "Sinus (any rate)",
"pr": "Normal",
"qrs": "Normal (narrow)",
"st_t": "Focal convex ST↑; hyperacute T; reciprocal ST↓",
"other": "Pathologic Q waves evolve within hours",
"hallmark": "Territory-specific ST↑ with mirror-image ST↓",
"leads": "V1–V4 (ant) · II,III,aVF (inf) · I,aVL (lat)",
},
{
"no": "02",
"name": "NSTEMI / UA",
"full": "Non-ST-Elevation ACS",
"color": colors.HexColor("#A93226"),
"rhythm": "Sinus ± tachycardia",
"pr": "Normal",
"qrs": "Normal (narrow)",
"st_t": "ST depression ± T-wave inversions; no ST elevation",
"other": "Wellens sign: deep symmetric T↓ V1–V4 → critical LAD stenosis",
"hallmark": "ST↓ in ≥2 contiguous leads (≥0.5 mm)",
"leads": "V1–V6, I, aVL",
},
{
"no": "03",
"name": "Atrial Fibrillation",
"full": "AF",
"color": TEAL,
"rhythm": "Irregularly irregular, 60–170 bpm (uncontrolled >170)",
"pr": "Absent (no P waves)",
"qrs": "Narrow (unless BBB/WPW)",
"st_t": "No specific changes",
"other": "Fibrillatory baseline (chaotic) best in V1",
"hallmark": "Absent P waves + irregularly irregular RR intervals",
"leads": "All leads",
},
{
"no": "04",
"name": "Atrial Flutter",
"full": "AFL",
"color": colors.HexColor("#148F77"),
"rhythm": "Regular 150 bpm (2:1); 100 bpm (3:1)",
"pr": "Not measurable (flutter waves)",
"qrs": "Narrow (unless BBB)",
"st_t": "No specific changes",
"other": "Atrial rate 250–350 bpm; 2:1 block commonest",
"hallmark": "Sawtooth flutter waves in II, III, aVF, V1",
"leads": "II, III, aVF, V1",
},
{
"no": "05",
"name": "1° AV Block",
"full": "First-Degree Heart Block",
"color": PURPLE,
"rhythm": "Regular sinus",
"pr": "Prolonged >200 ms; every P conducts",
"qrs": "Normal (narrow)",
"st_t": "Normal",
"other": "Usually benign; may occur with digoxin, inferior MI, vagal tone",
"hallmark": "PR >200 ms, no dropped beats",
"leads": "All leads",
},
{
"no": "06",
"name": "2° AV Block",
"full": "Mobitz I & II",
"color": colors.HexColor("#7D3C98"),
"rhythm": "Regularly irregular (group beating in Mobitz I)",
"pr": "Mobitz I: progressively lengthens → dropped QRS\nMobitz II: fixed PR → sudden dropped QRS",
"qrs": "Normal (Mobitz I); may be wide with BBB (Mobitz II)",
"st_t": "Normal",
"other": "Mobitz II → high risk of progression to complete block",
"hallmark": "Mobitz I: Wenckebach cycles · Mobitz II: abrupt dropped beat",
"leads": "Rhythm strip (II or V1)",
},
{
"no": "07",
"name": "3° AV Block",
"full": "Complete Heart Block",
"color": colors.HexColor("#512E5F"),
"rhythm": "P rate > QRS rate; complete AV dissociation",
"pr": "Variable (no relationship between P and QRS)",
"qrs": "Narrow (junctional escape 40–60 bpm)\nor Wide (ventricular escape 20–40 bpm)",
"st_t": "Normal (unless underlying ischemia)",
"other": "Fusion/capture beats absent (unlike VT). Syncope/Stokes-Adams attacks",
"hallmark": "P waves and QRS march independently",
"leads": "All leads",
},
{
"no": "08",
"name": "Acute Pericarditis",
"full": "Pericarditis (Stage 1–4)",
"color": AMBER,
"rhythm": "Sinus tachycardia (pain-driven)",
"pr": "PR depression in most leads; PR elevation in aVR ('knuckle sign')",
"qrs": "Normal",
"st_t": "Diffuse concave (saddle-shaped) ST↑ in ALL leads except aVR\nStage 3: diffuse T-wave inversions",
"other": "No reciprocal ST↓; no Q waves; ST elevation <5 mm",
"hallmark": "Diffuse concave ST↑ + PR depression (≠ focal STEMI)",
"leads": "I, II, III, aVF, V2–V6 (spares aVR/V1)",
},
{
"no": "09",
"name": "Ventricular Tachycardia",
"full": "VT (Monomorphic)",
"color": colors.HexColor("#CB4335"),
"rhythm": "Regular, 100–250 bpm",
"pr": "Dissociated (P waves unrelated to QRS)",
"qrs": "Wide ≥120 ms (usually >140 ms); LBBB or RBBB morphology",
"st_t": "Discordant (opposite to QRS main deflection)",
"other": "AV dissociation + fusion/capture beats = diagnostic of VT\nConcordance in precordial leads strongly favours VT",
"hallmark": "Wide QRS tachycardia + AV dissociation",
"leads": "All leads; aVR, V1 most diagnostic",
},
{
"no": "10",
"name": "Ventricular Fibrillation",
"full": "VF",
"color": colors.HexColor("#922B21"),
"rhythm": "Absent — chaotic undulations",
"pr": "None",
"qrs": "None — no organised complexes",
"st_t": "None",
"other": "May be fine (low amplitude) or coarse (higher amplitude)\nImmediate defibrillation + CPR",
"hallmark": "Completely chaotic waveform; no P, QRS or T",
"leads": "All leads",
},
{
"no": "11",
"name": "WPW Syndrome",
"full": "Wolff-Parkinson-White",
"color": GREEN,
"rhythm": "Sinus (normal rate in baseline)",
"pr": "Short PR <120 ms",
"qrs": "Slightly wide; slurred delta wave at QRS onset",
"st_t": "Discordant ST-T changes (opposite to delta/QRS direction)\nDelta waves may mimic Q-wave MI",
"other": "AVOID adenosine/β-blockers/CCBs/digoxin in AF+WPW (risk of VF)",
"hallmark": "Short PR + delta wave + wide QRS (pre-excitation triad)",
"leads": "Most prominent in leads with dominant QRS",
},
{
"no": "12",
"name": "Hypertrophic CM",
"full": "HCM",
"color": colors.HexColor("#1A5276"),
"rhythm": "Sinus; may have AF",
"pr": "Normal (may be short with LVH)",
"qrs": "Tall voltage (LVH criteria); deep narrow 'dagger' Q waves lateral leads",
"st_t": "Lateral ST depression + T-wave inversions\nApical HCM: massive T inversions V2–V5",
"other": "LVH voltage: S(V1) + R(V5/V6) >35 mm\nLeft atrial enlargement (bifid P); left axis deviation",
"hallmark": "LVH voltage + deep narrow Q waves lateral leads (not infarction)",
"leads": "I, aVL, V4–V6 (Q waves); V1–V4 (voltage)",
},
{
"no": "13",
"name": "Pulmonary Embolism",
"full": "Acute PE",
"color": colors.HexColor("#117864"),
"rhythm": "Sinus tachycardia (most common finding)",
"pr": "Normal",
"qrs": "Possible new RBBB (complete or incomplete)",
"st_t": "T-wave inversions V1–V4 (RV strain); S1Q3T3 pattern (~20%)",
"other": "Right axis deviation; P pulmonale (tall P in II)\nNormal ECG does not exclude PE",
"hallmark": "Sinus tachycardia ± S1Q3T3 ± T inversions V1–V4 (RV strain)",
"leads": "I, III, V1–V4",
},
]
# ── Column widths ─────────────────────────────────────────────────────────────
W = landscape(A4)
H = landscape(A4)[1]
PAGE_W = W - 20*mm # usable width after margins
# proportional column widths (total = 1.0):
# No | Condition | Rhythm | PR | QRS | ST/T | Other | Hallmark | Leads
COL_FRACTIONS = [0.028, 0.085, 0.115, 0.095, 0.115, 0.175, 0.185, 0.155, 0.047]
COL_WIDTHS = [PAGE_W * f for f in COL_FRACTIONS]
def build_header_row():
hdrs = ["#", "Condition", "Rhythm", "PR Interval",
"QRS Complex", "ST / T Changes", "Additional Features",
"Hallmark Finding", "Key Leads"]
return [p(h, "col_hdr") for h in hdrs]
def condition_cell(c):
return [
p(f"<b>{c['no']}</b>", "condition"),
p(f"<b>{c['name']}</b>", "condition"),
p(f"<i>{c['full']}</i>", "body"),
]
def build_data_row(c):
def wrap(txt):
return Paragraph(txt.replace("\n", "<br/>"), S["body"])
return [
p(f"<b>{c['no']}</b>", "bold_body"),
[p(f"<b>{c['name']}</b>", "condition"),
p(f"<i>{c['full']}</i>", "body")],
wrap(c["rhythm"]),
wrap(c["pr"]),
wrap(c["qrs"]),
wrap(c["st_t"]),
wrap(c["other"]),
Paragraph(f"<b>{c['hallmark']}</b>", S["highlight"]),
wrap(c["leads"]),
]
def row_style(i, color):
"""Return TableStyle commands for a single data row i (0-indexed, row 1 = first data row)."""
row = i + 1 # +1 for header
bg = LTGREY if i % 2 == 0 else WHITE
return [
("BACKGROUND", (0, row), (0, row), color),
("BACKGROUND", (1, row), (-1, row), bg),
("TEXTCOLOR", (0, row), (0, row), WHITE),
("FONTNAME", (0, row), (0, row), "Helvetica-Bold"),
]
def build_table(conditions):
rows = [build_header_row()] + [build_data_row(c) for c in conditions]
# Base style
style_cmds = [
# Header
("BACKGROUND", (0, 0), (-1, 0), NAVY),
("FONTNAME", (0, 0), (-1, 0), "Helvetica-Bold"),
("FONTSIZE", (0, 0), (-1, 0), 8),
("TEXTCOLOR", (0, 0), (-1, 0), WHITE),
("ALIGN", (0, 0), (-1, 0), "CENTER"),
("VALIGN", (0, 0), (-1, -1), "TOP"),
("FONTSIZE", (0, 1), (-1, -1), 7.2),
("ROWBACKGROUND", (0, 1), (-1, -1), [LTGREY, WHITE]),
("GRID", (0, 0), (-1, -1), 0.35, MIDGREY),
("LINEBELOW", (0, 0), (-1, 0), 1.2, NAVY),
("TOPPADDING", (0, 0), (-1, -1), 3),
("BOTTOMPADDING", (0, 0), (-1, -1), 3.5),
("LEFTPADDING", (0, 0), (-1, -1), 3),
("RIGHTPADDING", (0, 0), (-1, -1), 3),
# Hallmark column emphasis
("FONTNAME", (7, 1), (7, -1), "Helvetica-BoldOblique"),
("TEXTCOLOR", (7, 1), (7, -1), CRIMSON),
# Alternate row backgrounds
*[("BACKGROUND", (1, i+1), (-1, i+1), LTGREY if i % 2 == 0 else WHITE)
for i in range(len(conditions))],
# Color strip in column 0
*[("BACKGROUND", (0, i+1), (0, i+1), conditions[i]["color"])
for i in range(len(conditions))],
("TEXTCOLOR", (0, 1), (0, -1), WHITE),
("ALIGN", (0, 1), (0, -1), "CENTER"),
("FONTNAME", (0, 1), (0, -1), "Helvetica-Bold"),
]
t = Table(rows, colWidths=COL_WIDTHS, repeatRows=1)
t.setStyle(TableStyle(style_cmds))
return t
def build_legend():
"""Small footnote legend."""
text = (
"<b>Abbreviations:</b> "
"ACS = Acute Coronary Syndrome · AF = Atrial Fibrillation · AFL = Atrial Flutter · "
"AV = Atrioventricular · BBB = Bundle Branch Block · CCB = Calcium Channel Blocker · "
"CM = Cardiomyopathy · CPR = Cardiopulmonary Resuscitation · HCM = Hypertrophic Cardiomyopathy · "
"LAD = Left Anterior Descending · LBBB = Left Bundle Branch Block · LCx = Left Circumflex · "
"LVH = Left Ventricular Hypertrophy · MI = Myocardial Infarction · NSTEMI = Non-ST-Elevation MI · "
"PE = Pulmonary Embolism · RBBB = Right Bundle Branch Block · RCA = Right Coronary Artery · "
"RV = Right Ventricular · STEMI = ST-Elevation MI · UA = Unstable Angina · "
"VF = Ventricular Fibrillation · VT = Ventricular Tachycardia · WPW = Wolff-Parkinson-White | "
"<b>Sources:</b> Harrison's 22e · Tintinalli's 9e · Braunwald's Heart Disease · "
"Fuster & Hurst's The Heart 15e · Washington Manual · Goldman-Cecil Medicine"
)
return Paragraph(text, S["footer"])
def build_title_block():
title_data = [[
Paragraph("ECG QUICK-REFERENCE CARD", S["title"]),
]]
title_style = TableStyle([
("BACKGROUND", (0, 0), (-1, -1), NAVY),
("TOPPADDING", (0, 0), (-1, -1), 7),
("BOTTOMPADDING", (0, 0), (-1, -1), 4),
("LEFTPADDING", (0, 0), (-1, -1), 8),
("RIGHTPADDING", (0, 0), (-1, -1), 8),
])
subtitle_data = [[
Paragraph(
"13 Common Cardiac Conditions · Rhythm · PR · QRS · ST/T Changes · Hallmark Findings · Key Leads",
S["subtitle"]
)
]]
subtitle_style = TableStyle([
("BACKGROUND", (0, 0), (-1, -1), NAVY),
("TOPPADDING", (0, 0), (-1, -1), 0),
("BOTTOMPADDING", (0, 0), (-1, -1), 8),
("LEFTPADDING", (0, 0), (-1, -1), 8),
("RIGHTPADDING", (0, 0), (-1, -1), 8),
])
t1 = Table(title_data, colWidths=[PAGE_W])
t1.setStyle(title_style)
t2 = Table(subtitle_data, colWidths=[PAGE_W])
t2.setStyle(subtitle_style)
return [t1, t2]
# ── Build PDF ────────────────────────────────────────────────────────────────
def build():
doc = SimpleDocTemplate(
OUTPUT,
pagesize=landscape(A4),
leftMargin=10*mm, rightMargin=10*mm,
topMargin=8*mm, bottomMargin=8*mm,
)
story = []
story += build_title_block()
story.append(Spacer(1, 3*mm))
story.append(build_table(CONDITIONS))
story.append(Spacer(1, 2.5*mm))
story.append(HRFlowable(width="100%", thickness=0.5, color=MIDGREY))
story.append(Spacer(1, 1*mm))
story.append(build_legend())
doc.build(story)
print(f"PDF written to: {OUTPUT}")
if __name__ == "__main__":
build()
Running Command
cd /home/daytona/workspace/ecg-reference && python3 build_ecg_card.py 2>&1
Editing File
~/ecg-reference/build_ecg_card.py
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/ecg-reference/build_ecg_card.py'
Running Command
cd /home/daytona/workspace/ecg-reference && python3 build_ecg_card.py 2>&1
Running Command
ls -lh /home/daytona/workspace/ecg-reference/ECG_Quick_Reference.pdf
Your quick-reference PDF card is ready:
ECG Quick Reference
PDF Document · PDF
What's in the card:
- Single A4 landscape page - print-ready, compact enough to fit in a pocket folder or laminate
- 13 conditions covered: STEMI, NSTEMI/UA, AF, Atrial Flutter, 1°/2°/3° AV Block, Acute Pericarditis, VT, VF, WPW, HCM, and Acute PE
- 9 columns per condition:
- Numbered colour-coded strip (unique colour per condition)
- Condition name & abbreviation
- Rhythm
- PR interval findings
- QRS complex findings
- ST/T changes
- Additional features (including critical warnings, e.g. "AVOID adenosine in AF+WPW")
- Hallmark finding - highlighted in red bold italic for fast scanning
- Key leads
- Abbreviations legend and source textbooks at the bottom
This is a shared conversation. Sign in to Orris to start your own chat.