Operative steps of open left hemicolectomy
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Open Left Hemicolectomy - Operative Steps
Indication: Carcinoma of the descending colon, splenic flexure, and proximal sigmoid colon. The operation removes the left colon from the distal transverse colon to the proximal sigmoid, based on the vascular supply of the inferior mesenteric artery (IMA) and its left colic branch.
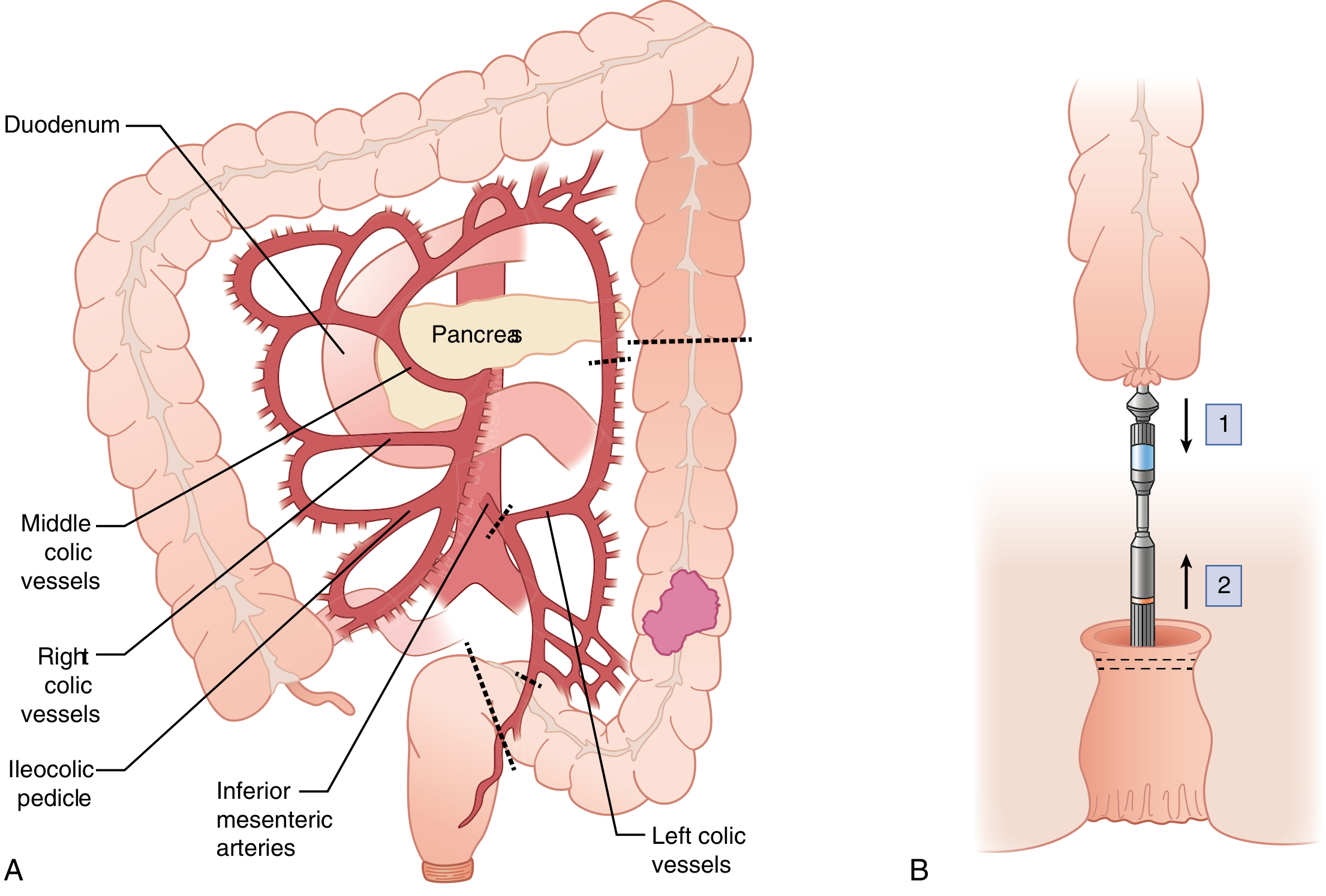
Left hemicolectomy: (A) IMA ligation, left colic vessels, and marginal artery division shown. (B) Double-stapled end-to-end anastomosis technique. - Sabiston Textbook of Surgery
Preoperative
- Mechanical bowel prep (surgeon-dependent) + antibiotic prophylaxis
- Thromboprophylaxis (LMWH + compression stockings)
- Ureteric stents considered for re-do or bulky tumors
- Position: supine or modified Lloyd-Davies (low lithotomy) to allow trans-anal access if needed; arms tucked, patient strapped to prevent slippage
Step 1 - Incision and Exploration
- Midline laparotomy from xiphisternum to pubis
- Systematic exploration for peritoneal disease, liver metastases, and lymphadenopathy to confirm resectability
- Visual inspection and palpation of the liver, omentum, and peritoneal surfaces
Step 2 - Medial-to-Lateral Mesocolic Dissection (Central Vascular Ligation)
- The small bowel is packed to the right and the omentum reflected superiorly
- The sigmoid mesocolon is lifted and the peritoneum of the mesentery is incised over the aorta at the base of the IMA
- The inferior mesenteric artery (IMA) is ligated close to its origin from the aorta ("high tie") - this includes the left colic artery and paracolic lymph nodes en bloc
- The inferior mesenteric vein (IMV) is separately ligated and divided at the inferior border of the pancreas (at the ligament of Treitz), providing full mobility
- Dissection proceeds in the avascular retroperitoneal plane (Toldt's fascia), anterior to Gerota's fascia, lifting the left mesocolon off the retroperitoneum
Critical: The left ureter and left gonadal vessels must be clearly identified in the retroperitoneum and swept posteriorly before any vascular ligation. They are most at risk during mobilization of the sigmoid mesentery.
Step 3 - Lateral Mobilization of the Left Colon
- The peritoneal "white line of Toldt" along the lateral attachment of the descending colon is incised with diathermy or scissors, from the sigmoid up to the splenic flexure
- The descending colon is mobilized medially off the left paracolic gutter in the avascular plane of the fascia of Toldt
- The ureter and gonadal vessels are again confirmed safe at this stage
Step 4 - Splenic Flexure Mobilization
This is one of the most technically demanding steps and is required to ensure a tension-free anastomosis.
- The splenocolic ligament is divided sharply - traction on the colon risks splenic capsular tears
- The lesser sac is entered by dividing the gastrocolic ligament / omental attachments from the transverse colon working toward the splenic flexure
- The omentum is dissected from the anterior surface of the transverse colon
- IMV attachments to the anterior surface of the pancreas are divided
- The medial and lateral planes of dissection meet, fully freeing the splenic flexure
- If greater reach is needed (extended left hemicolectomy), the right colon may also be mobilized
Step 5 - Bowel Division and Specimen Removal
- Proximal division: the distal transverse colon is divided at an appropriate point where vascularity (via middle colic artery) is confirmed; the left branch of the middle colic artery and marginal artery are ligated just distal to the transection line
- Distal division: at the proximal sigmoid (or at the upper rectum for an extended resection), with ligation of the superior rectal / sigmoid vessels
- A 5-7 cm clear margin proximal and distal to the tumor is standard
- The specimen is extracted, including a wedge of mesentery with all draining lymph nodes; a minimum of 12 lymph nodes must be harvested for accurate staging
- The greater omentum attached to the resected segment is removed en bloc
Step 6 - Anastomosis (Colorectal / Colocolonic)
- A tension-free, well-vascularized anastomosis is fashioned between the transverse colon and the upper rectum or proximal sigmoid
- Both stapled (double-stapled end-to-end or end-to-side circular) and handsewn (two-layer technique) methods are acceptable; no randomized data favor one over the other
- The mesenteric window is checked and closed to prevent internal hernia
- A temporary diverting loop ileostomy is recommended if the anastomosis is below the peritoneal reflection (increased leak risk)
Step 7 - Washout, Hemostasis, and Closure
- Peritoneal lavage with warm saline
- Confirm hemostasis at the vascular pedicles, retroperitoneum, and splenic flexure bed
- Drain placement is surgeon-dependent (not routinely recommended in uncomplicated cases)
- Layered mass closure of the abdominal wall (PDS loop or continuous PDS)
Key Anatomical Hazards Summary
| Structure | Risk |
|---|---|
| Left ureter | Ligation or diathermy injury during mesocolic dissection |
| Left gonadal vessels | Division during sigmoid mobilization |
| Spleen | Capsular tear during splenocolic ligament division |
| Duodenum | At risk during high IMV ligation near pancreatic border |
| Superior hypogastric plexus | Damage during high IMA ligation - causes bladder/sexual dysfunction |
Oncologic Principles
- Complete mesocolic excision (CME) along embryological planes with central vascular ligation improves lymph node harvest and may improve survival in node-positive disease (Bailey & Love)
- The extent of resection is dictated by the tumor's vascular territory: splenic flexure/descending colon tumors require the left branch of the middle colic + left colic artery; sigmoid tumors require the sigmoid branches from the IMA (Fischer's Mastery of Surgery)
- Splenic flexure cancers may alternatively be managed with an extended right hemicolectomy; oncologic outcomes are considered equivalent (Current Surgical Therapy 14e)
Sources: Bailey and Love's Short Practice of Surgery 28th Ed., Sabiston Textbook of Surgery, Fischer's Mastery of Surgery 8th Ed., Schwartz's Principles of Surgery 11th Ed., Current Surgical Therapy 14th Ed., Mulholland & Greenfield's Surgery 7th Ed.
Operative steps of open left hemicolectomy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive, textbook-sourced detail from Bailey & Love, Fischer's Mastery of Surgery, Sabiston, and Current Surgical Therapy. Here is the full structured answer:
Open Left Hemicolectomy - Operative Steps
Definition: Resection of the left colon (distal transverse colon, splenic flexure, descending colon, and proximal sigmoid) based on the vascular territory of the inferior mesenteric artery (IMA) and left colic artery (LCA). The operation of choice for carcinoma of the descending colon, splenic flexure, and proximal sigmoid.
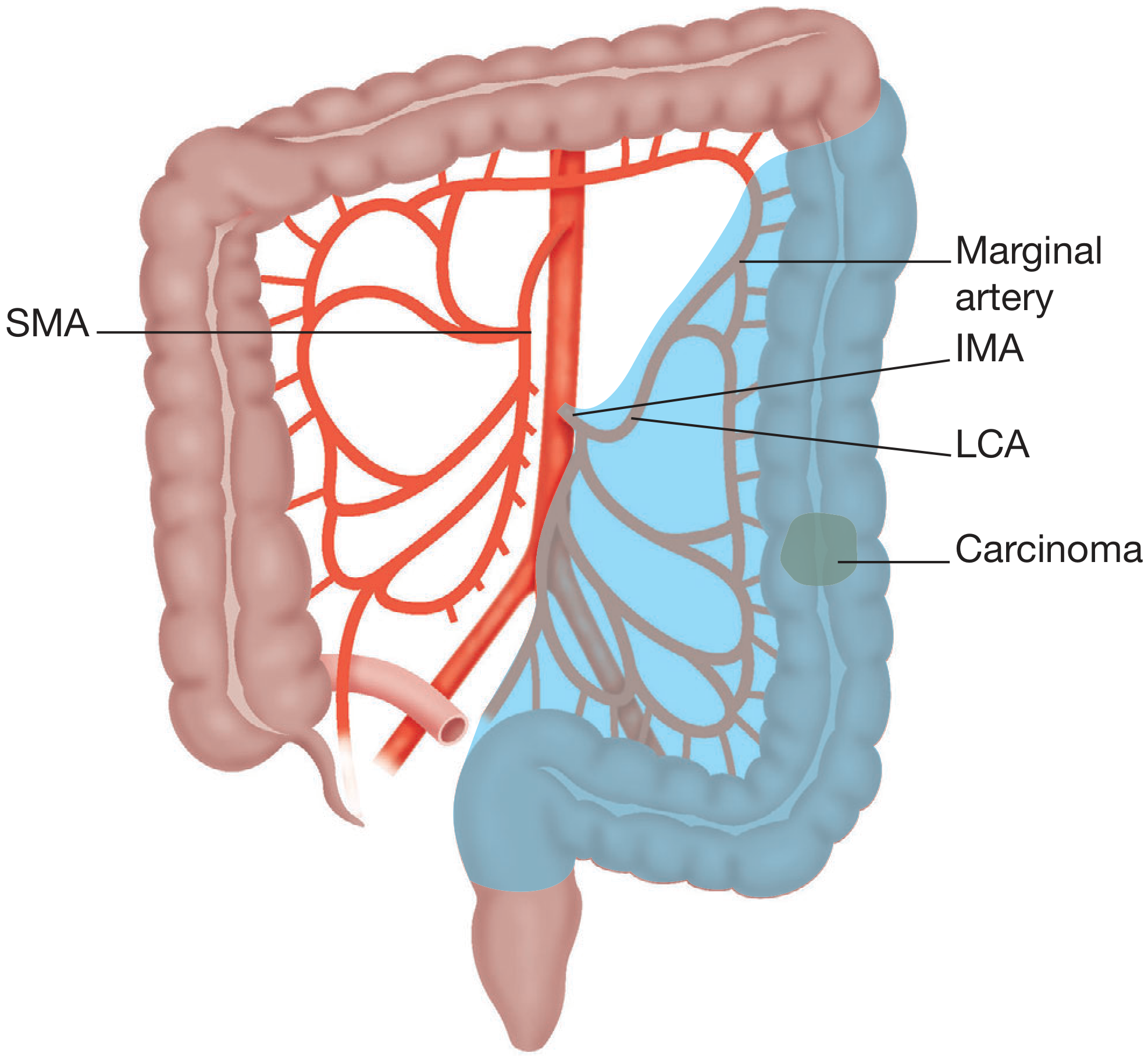
Figure: Extent of resection for left hemicolectomy (shaded blue). The IMA and LCA are ligated at their origins; the resected segment spans the splenic flexure to proximal sigmoid. - Bailey & Love's Short Practice of Surgery 28th Ed.
Preoperative Preparation
- Mechanical bowel prep (surgeon preference) + oral antibiotics
- IV antibiotic prophylaxis within 30 min of incision (e.g., cefoxitin + metronidazole)
- Rectal irrigation catheter placed (Foley 30 cc) to create a stool-free anastomotic field
- VTE prophylaxis: LMWH + pneumatic compression stockings
- Ureteric stents: consider for bulky, re-do, or locally advanced tumors
- Cross-match blood; IDC catheter
- Consent for stoma
Patient Positioning
- Supine or modified Lloyd-Davies (low lithotomy) - the latter allows trans-anal endoscopic access for anastomotic leak testing
- Arms tucked; patient secured with straps and non-slip pad to prevent slippage during table tilting
- Nasogastric tube at discretion
Step 1 - Incision
- Standard midline laparotomy from xiphisternum to pubis
- Self-retaining retractor placed (e.g., Bookwalter or Omni); wound protector inserted (reduces wound contamination and aids retraction)
- Small bowel packed to the right upper quadrant with warm moist packs
Step 2 - Abdominal Exploration
- Systematic inspection and palpation of the entire peritoneal cavity
- Liver (bimanual palpation for metastases), omentum, peritoneal surfaces, and pelvic organs
- Confirm resectability and identify the primary tumor
Step 3 - Lateral-to-Medial Mobilization of the Left Colon (preferred for open approach)
Note: Lateral-to-medial is the traditional approach for open surgery. Medial-to-lateral (starting at the IMV) is preferred for minimally invasive surgery but can also be used open to help develop the learning curve. - Fischer's Mastery of Surgery 8th Ed.
- The white line of Toldt (lateral peritoneal reflection of the descending colon mesentery) is incised with diathermy from the sigmoid colon upward to the splenic flexure
- The descending colon is elevated anteromedially off the left paracolic gutter, developing the avascular plane between the colonic mesentery (mesocolic fascia) and the retroperitoneum (Gerota's fascia anteriorly, fascia of Toldt)
- Left ureter is identified crossing the iliac vessels and swept posteriorly - must be confirmed safe before any vascular ligation
- Left gonadal vessels (ovarian/testicular) are similarly identified and protected medial to the ureter
- Mobilization continues cephalad as the sigmoid mesentery is freed
Step 4 - Splenic Flexure Mobilization (most technically demanding step)
- The splenocolic ligament is divided under direct vision - avoid traction on the colon to prevent splenic capsular tears
- The lesser sac is entered by dividing the gastrocolic ligament, separating the omentum from the anterior surface of the transverse colon and working toward the splenic flexure
- Attachments of the mesocolon to the anterior surface of the pancreas are divided; the IMV is identified here (lateral to the ligament of Treitz) and ligated at the inferior border of the pancreas - this is the single most important step for achieving full mobility of the left colon
- The lateral (omental) and medial (retroperitoneal) planes of dissection are joined, fully freeing the splenic flexure
- For an extended left hemicolectomy (e.g., mid-transverse colon lesions), full mobilization and counterclockwise rotation of the right colon may also be required to achieve a tension-free anastomosis
Step 5 - Central Vascular Ligation (CME Principle)
Complete mesocolic excision (CME) requires dissection along embryological fascial planes with high-tie vascular ligation:
For splenic flexure / proximal descending colon cancers:
- Ligate the left branch of the middle colic artery and the left colic artery at their branch points from the IMA
For mid/distal descending colon and upper sigmoid cancers:
- IMA ligated close to its aortic origin ("high tie") - this includes the left colic artery, sigmoid branches, and their draining lymph node chain
- The IMV is ligated separately at the inferior border of the pancreas for maximum mobility
Before ligation: confirm the left ureter lies lateral to the IMA by direct visualization. The superior hypogastric plexus runs just anterior to the aortic bifurcation and must not be divided to preserve bladder and sexual function.
Figure 96.9: Left hemicolectomy. (A) IMA ligated at origin; marginal artery divided at bowel transection lines. (B) Double-stapled end-to-end anastomosis. - Sabiston Textbook of Surgery
Step 6 - Mesenteric Division and Specimen Mobilization
- The mesocolon is divided in a wedge from the vascular ligation point toward the bowel wall at both transection lines
- The marginal artery is ligated just distal (and proximal) to the intended bowel transection sites, confirming viable cut ends
- Mesenteric division includes the lymphovascular pedicle en bloc with the specimen
Step 7 - Bowel Transection and Specimen Removal
- Proximal transection: through the distal transverse colon - ensure viable, tension-free end with good mesenteric arcades from the middle colic artery
- Distal transection: at the proximal sigmoid colon (or upper rectum for extended resection)
- Margins: minimum 5 cm proximal and distal clearance; distal margin ≥2 cm for upper rectal lesions
- The attached greater omentum is divided and removed en bloc with the specimen
- Minimum 12 lymph nodes must be harvested for adequate N-staging
- Specimen placed in wound protector bag for extraction; instruments changed after specimen removal; gloves changed before anastomosis to avoid contamination
Step 8 - Anastomosis (Colorectal or Colocolonic)
A tension-free, well-vascularized anastomosis is fashioned between the transverse colon and upper rectum/sigmoid.
Options (equivalent outcomes in RCTs):
| Technique | Method |
|---|---|
| Stapled end-to-end | Circular EEA stapler; double-stapled technique via trans-anal anvil placement |
| Stapled side-to-end | For low colorectal anastomoses |
| Handsewn | Two-layer interrupted/continuous; used when stapler not feasible |
- Mesenteric defect is closed to prevent internal herniation
- Anastomotic integrity test: pelvis filled with saline; proximal bowel clamped; flexible sigmoidoscopy performed - visualize the anastomosis for leak, bleeding, malperfusion (UCI grade I-III); Grade III requires revision
Defunctioning stoma:
- A loop ileostomy is recommended when the anastomosis is at or below the peritoneal reflection, in cases of technical difficulty, or when anastomotic tension/vascularity is uncertain - higher leak risk at this level
Step 9 - Washout, Hemostasis, and Closure
- Peritoneal lavage with warm saline (especially if bowel spillage occurred)
- Inspect vascular pedicle stumps, retroperitoneal dissection bed, and splenic bed for hemostasis
- Drain placement: not routinely recommended in uncomplicated cases; consider if anastomosis is low or tension on closure
- Abdominal closure: mass continuous PDS suture (loop or single-strand); subcutaneous irrigation; skin closure per surgeon preference
Key Anatomical Hazards
| Structure | Mechanism of Injury | Consequence |
|---|---|---|
| Left ureter | Ligation or diathermy in mesocolic dissection | Ureteric injury/obstruction |
| Left gonadal vessels | Division during sigmoid mesentery mobilization | Gonadal ischaemia |
| Spleen | Traction on splenocolic ligament | Capsular tear, splenectomy |
| Duodenum (4th part) | Dissection near ligament of Treitz during IMV ligation | Duodenotomy |
| Superior hypogastric plexus | High IMA ligation, aortic dissection | Bladder dysfunction, retrograde ejaculation |
| Left ureter (second risk point) | During distal sigmoid transection near pelvic brim | Pelvic ureteric injury |
Oncologic Principles Summary
- Complete mesocolic excision (CME): intact removal of mesocolic fascia along embryological planes with central vascular ligation; improves lymph node yield and may improve survival in node-positive disease
- Extent of vascular ligation is tumor-location dependent: splenic flexure tumors → left branch of middle colic + LCA; descending/sigmoid → IMA high tie
- Splenic flexure carcinomas may equivalently be treated by extended right hemicolectomy (oncologic outcomes comparable) - Current Surgical Therapy 14e
- Stapled and handsewn anastomoses have equivalent outcomes in randomized trials
Sources: Bailey & Love's Short Practice of Surgery 28th Ed. | Fischer's Mastery of Surgery 8th Ed. | Sabiston Textbook of Surgery | Schwartz's Principles of Surgery 11th Ed. | Current Surgical Therapy 14th Ed. | Mulholland & Greenfield's Surgery 7th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.