Enumerate injuries sustained due to FOOSH
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Now I have comprehensive textbook data to give a thorough, well-organized answer.
Injuries from FOOSH (Fall On OutStretched Hand)
FOOSH transmits a compressive axial load up the upper limb while the wrist is in dorsiflexion. The pattern of injury depends on age, bone density, wrist angle at impact, and the magnitude of force. Injuries occur at multiple levels simultaneously and should all be considered.
By Anatomical Level (Distal to Proximal)
1. Wrist / Distal Forearm
| Injury | Key Features |
|---|---|
| Colles' Fracture | Fracture of the distal radius metaphysis with dorsal displacement and volar angulation; most common wrist fracture in adults, especially older women; produces the classic "dinner fork" deformity; often accompanied by ulnar styloid fracture |
| Smith's Fracture | Reverse Colles' - distal radius fractures with volar displacement; occurs with wrist in palmar flexion at impact |
| Barton's Fracture | Intra-articular fracture of the dorsal rim of distal radius with radiocarpal subluxation |
| Volar (Reverse) Barton's | Intra-articular fracture of the volar rim; wrist is in volar flexion at impact; rarer |
| Chauffeur's Fracture | Isolated radial styloid fracture; caused by deviation and supination forces |
| Greenstick/Torus fracture | Buckle fracture of distal radius; typical in children due to pliable bone |
| Galeazzi Fracture-Dislocation | Fracture of the distal radial shaft with disruption of the distal radioulnar joint |
(ROSEN's Emergency Medicine; Tintinalli's Emergency Medicine)
2. Carpal Bones
| Injury | Key Features |
|---|---|
| Scaphoid Fracture | Most common carpal fracture (60-70% of all carpal fractures); waist fractures predominate (2/3 of cases); snuffbox tenderness; high risk of AVN with proximal pole fractures; X-rays may be negative initially |
| Lunate Fracture / Kienbock Disease | Axial load to lunate; can lead to avascular necrosis |
| Triquetrum Fracture | Second most common carpal fracture; usually a dorsal avulsion chip |
| Hamate Fracture | Hook fracture from direct palm strike or outstretched hand; associated with ulnar nerve/artery injury |
| Pisiform Fracture | Direct impact; base of hypothenar |
| Trapezium Fracture | Axial load along thumb metacarpal |
| Lunate/Perilunate Dislocation | High-energy FOOSH; perilunate dislocation precedes lunate dislocation on a spectrum of carpal instability |
| Carpal Instability (DISI/VISI) | Scapholunate or lunotriquetral ligament tears causing intercalated segment instability |
(Tintinalli's Emergency Medicine; ROSEN's Emergency Medicine)
3. Forearm Shafts
| Injury | Key Features |
|---|---|
| Radial Shaft Fracture | Isolated or combined; from direct violence or indirect FOOSH |
| Ulnar Shaft Fracture | Can occur with forearm in forced pronation |
| Both-Bone Forearm Fracture | Combined radius and ulna fractures; higher energy |
| Monteggia Fracture-Dislocation | Proximal ulna fracture + anterior dislocation of radial head; FOOSH with forced forearm pronation |
(Pye's Surgical Handicraft; Imaging Anatomy, Bones & Joints)
4. Elbow
| Injury | Key Features |
|---|---|
| Radial Head / Neck Fracture | Most common elbow fracture in adults (33-50% of elbow fractures); axial loading forces; classified by Mason system; associated with Essex-Lopresti injury (disruption of interosseous membrane + DRUJ) |
| Olecranon Fracture | Can occur with indirect FOOSH mechanism; more complex fracture-dislocation patterns |
| Coronoid Process Fracture | Often associated with elbow dislocation |
| Supracondylar Fracture of Humerus | Most common elbow fracture in children; FOOSH with elbow in full extension; extension type (95-98%); high risk of anterior interosseous nerve injury and Volkmann's ischemic contracture |
| Posterior Elbow Dislocation | Most common type (>90%); FOOSH causing hyperextension with valgus stress; associated with brachial artery injury (5-15%) and median nerve injury; frequently accompanied by radial head, coronoid, or distal humerus fractures ("terrible triad") |
| Capitellum Fracture | Shear force at capitellum; diagnosed on lateral X-ray |
| Medial Epicondyle Avulsion | Associated with elbow dislocation in children |
(ROSEN's Emergency Medicine; Tintinalli's Emergency Medicine; Rockwood & Green's Fractures in Adults 10th ed)
5. Humerus
| Injury | Key Features |
|---|---|
| Proximal Humeral Fracture | FOOSH with shoulder in flexion, abduction, and internal rotation; humeral head forced into valgus; common in osteoporotic elderly; Neer classification |
| Humeral Shaft Fracture | Less commonly from FOOSH; more often direct blow; risk of radial nerve injury |
(Rockwood & Green's Fractures in Adults 10th ed)
6. Shoulder Girdle
| Injury | Key Features |
|---|---|
| Clavicle Fracture | Force transmitted through outstretched arm to clavicle; middle third most common (80%); can also result from direct blow to shoulder |
| Acromioclavicular Joint Injury | Force transmitted from arm through acromion to clavicle |
| Glenohumeral Dislocation | Anterior dislocation most common; force applied along abducted, externally rotated arm |
| Glenoid Fracture | Impaction of humeral head on glenoid rim from FOOSH |
(Pye's Surgical Handicraft; Schwartz's Principles of Surgery; Rockwood & Green's)
Age-Based Patterns
| Age Group | Typical Injury |
|---|---|
| Children | Torus/greenstick distal radius, supracondylar fracture, lateral condyle fracture, medial epicondyle avulsion |
| Young Adults | Scaphoid fracture, carpal dislocations, radial head fracture |
| Older Adults (osteoporotic) | Colles' fracture, proximal humeral fracture, radial head fracture |
Associated Neurovascular Injuries to Exclude
- Anterior interosseous nerve - supracondylar fractures (inability to flex thumb IP and index DIP)
- Radial nerve - humeral shaft fractures (wrist drop)
- Median nerve - elbow dislocations
- Ulnar nerve/artery - hamate hook fractures
- Brachial artery - elbow dislocations (5-15%), supracondylar fractures
- Volkmann's ischemic contracture - compartment syndrome following supracondylar fracture
Sources: ROSEN's Emergency Medicine (Concepts and Clinical Practice); Tintinalli's Emergency Medicine (Comprehensive Study Guide); Rockwood and Green's Fractures in Adults 10th ed; Bailey and Love's Short Practice of Surgery 28th ed; Pye's Surgical Handicraft 22nd ed; Swanson's Family Medicine Review.
Mention injuries around wrist joint
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive, structured account of all injuries around the wrist joint, drawn directly from the textbooks.
Injuries Around the Wrist Joint
The wrist extends from the distal radius and ulna proximally to the carpometacarpal joints distally. It accounts for 2.5% of all ED visits annually and up to 25% of sports injuries. Injuries are grouped into four categories: distal radius/ulna fractures, carpal bone fractures, ligamentous/instability injuries, and soft tissue injuries.
Normal wrist PA X-ray anatomy for reference:
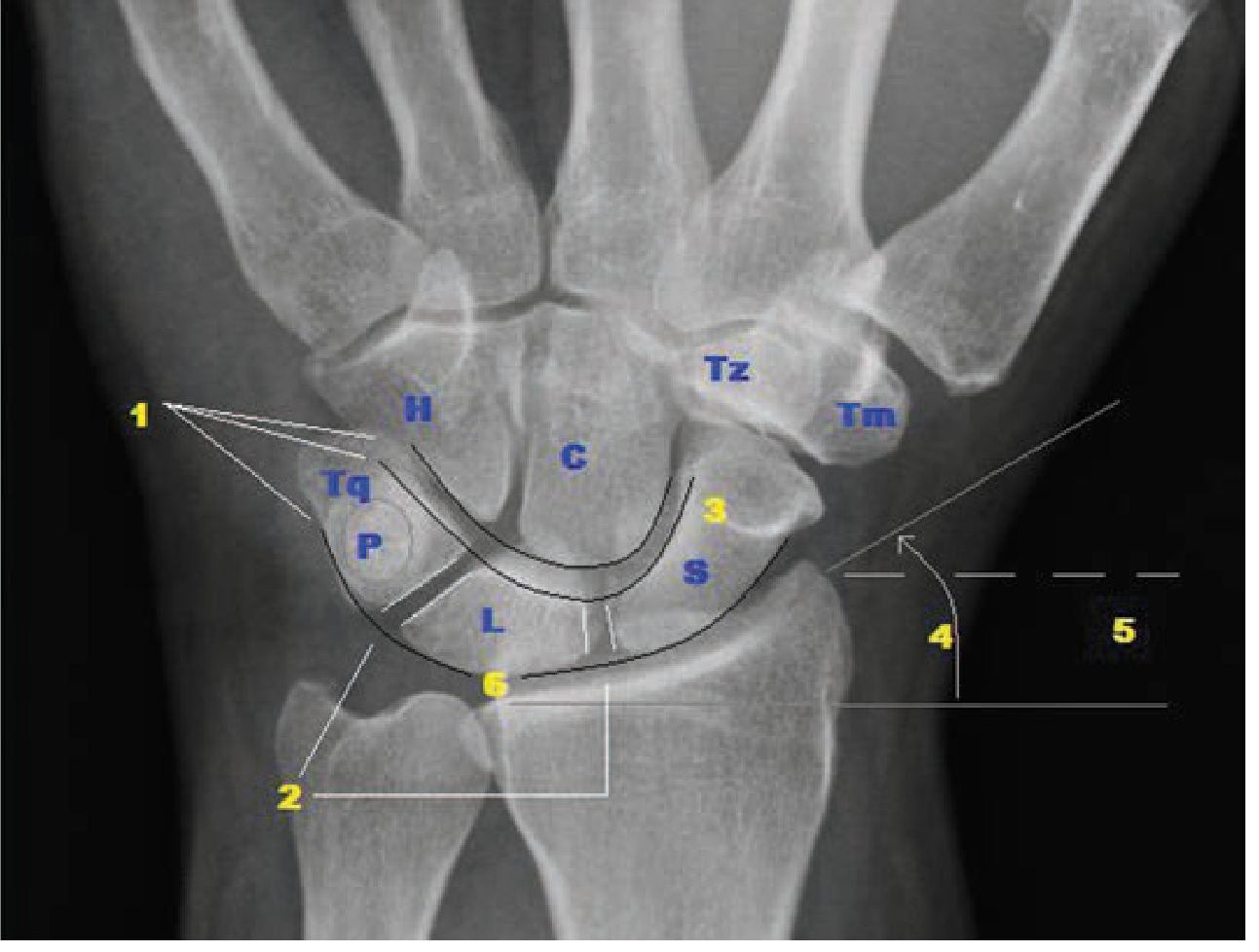
S = scaphoid; L = lunate; Tq = triquetrum; P = pisiform; C = capitate; H = hamate; Tm = trapezium; Tz = trapezoid. The three Gilula lines (arcs 1, 2, 3) should be smooth - disruption implies fracture, dislocation, or subluxation.
A. Distal Radius and Ulna Fractures
These are the most common wrist fractures and occur at the weakest point - the distal radial metaphysis.
1. Colles' Fracture
- Fracture of the distal radial metaphysis with dorsal displacement and volar angulation
- Classic mechanism: FOOSH with wrist in dorsiflexion
- "Dinner fork" deformity on lateral view; "bayonet" deformity on AP
- Most common in elderly osteoporotic women
- Often accompanied by an ulnar styloid fracture
- Requires closed reduction and cast immobilization; may need surgical fixation if intra-articular or unstable
2. Smith's Fracture ("Reverse Colles'")
- Distal radius fracture with volar displacement
- Mechanism: FOOSH with wrist in palmar flexion, or direct blow to dorsum of wrist
- "Garden spade" deformity
- Inherently unstable - often requires surgical fixation
3. Barton's Fracture
- Intra-articular fracture of the dorsal rim of the distal radius with radiocarpal subluxation
- Results from high-velocity impact across the wrist in dorsiflexion
- Unstable; usually requires ORIF
4. Volar (Reverse) Barton's Fracture
- Intra-articular fracture of the volar rim of the radius with volar radiocarpal dislocation
- Wrist is in palmar flexion at time of impact
- Rarer than dorsal Barton's
5. Chauffeur's Fracture (Radial Styloid Fracture)
- Isolated transverse or oblique fracture of the radial styloid, extending from the scaphoid fossa to the radial metaphysis
- Named for chauffeurs who suffered violent backfire of hand cranks
- Force directed along the radial side of the wrist; produced by ulnar deviation and supination
6. Greenstick / Torus (Buckle) Fracture
- Seen in children due to pliable immature bone
- Torus: cortical buckling on the compression side without complete fracture
- Greenstick: fracture through one cortex, bowing of the other
7. Galeazzi Fracture-Dislocation
- Fracture of the distal radial shaft combined with disruption of the distal radioulnar joint (DRUJ)
- Wrist pain + forearm deformity; ulna head prominent on dorsum
- Requires ORIF of radius + DRUJ stabilization
8. Distal Radioulnar Joint (DRUJ) Injury
- Piano key sign positive (ulnar head springs back when depressed)
- Pain with pronation/supination
- Often associated with TFCC tear
B. Carpal Bone Fractures
Carpal fractures are the most commonly missed wrist injuries. Impact on the thenar eminence tends to injure the scaphoid; impact on the hypothenar eminence tends to injure the triquetrum and pisiform.
1. Scaphoid Fracture (Most common carpal fracture - 60-70%)
- Mechanism: FOOSH on dorsiflexed hand, or axial load along thumb metacarpal
- Anatomic snuffbox tenderness (sensitivity 90%), scaphoid tubercle tenderness (sensitivity 87%)
- Waist = 2/3 of fractures; proximal pole = 16-28%; distal pole = 10%
- X-rays may be negative for up to 2 weeks - MRI is the gold standard if high clinical suspicion
- Complication: Avascular necrosis of the proximal fragment (risk up to 80% in proximal pole fractures) due to the retrograde blood supply entering distally
- Non-union and post-traumatic arthritis (SNAC wrist) if untreated
2. Triquetrum Fracture (Second most common)
- Usually a dorsal chip avulsion fracture (dorsal radiocarpal or intercarpal ligament avulsion)
- Best seen on lateral X-ray
- Often associated with lunotriquetral (LT) ligament injury
3. Lunate Fracture
- Rare as an isolated injury
- Associated with perilunate dislocation
- Avascular necrosis of the lunate = Kienbock's disease (osteonecrosis from repetitive microtrauma or acute fracture)
4. Capitate Fracture
- Often occurs in combination with scaphoid fracture (scaphocapitate syndrome)
- Proximal pole at risk for osteonecrosis due to retrograde blood supply
- May be part of perilunate injury spectrum
5. Hamate Fracture
- Hook of hamate fracture: fall on outstretched hand or direct palm strike; common in racquet sports, golf, baseball
- Best seen on carpal tunnel radiographic view or CT
- Associated with ulnar nerve/artery injury in Guyon's canal (ring/small finger weakness, pain)
- Chronic non-union can cause flexor tendon rupture (ring/small finger FDP)
6. Pisiform Fracture
- Direct impact to hypothenar region
- Treated with immobilization; excision if symptomatic non-union
7. Trapezium Fracture
- Axial load along the thumb metacarpal; radial styloid impaction
- Often associated with 1st CMC dislocation
8. Trapezoid Fracture
- Extremely rare due to protected position
C. Ligamentous Injuries and Carpal Instability
Ligamentous injuries are centered on the lunate, and form a spectrum of progressive severity based on force applied (Mayfield stages I-IV).
1. Scapholunate (SL) Ligament Tear - Most common wrist ligament injury
- FOOSH on thenar eminence
- Dorsal wrist pain, "clicking" with movement, tenderness distal to Lister's tubercle
- Radiographic findings:
- Terry Thomas sign (SL gap >3 mm on PA view; >8 mm on clenched fist view)
- Cortical ring sign (scaphoid foreshortening due to palmar rotation)
- DISI (Dorsal Intercalated Segment Instability) on lateral: SL angle >60°, lunate tilts dorsally
- Watson shift test: painful clunk with radial deviation while pressure applied over scaphoid tubercle
- Gold standard diagnosis: wrist arthroscopy (Geissler classification)
2. Lunotriquetral (LT) Ligament Tear
- FOOSH on hypothenar eminence
- Ulnar-sided wrist pain; LT ballottement test positive
- VISI (Volar Intercalated Segment Instability): lunate tilts volarly
- Less common and subtler than SL injury
3. Perilunate Dislocation (Mayfield Stage II-III)
- High-energy FOOSH; dorsal dislocation of all carpal bones relative to the lunate
- Lunate maintains its relationship with the radius
- Disruption through the space of Poirier (weak volar capsule between the two palmar arcades)
- On lateral X-ray: capitate lies dorsal to the lunate
4. Lunate Dislocation (Mayfield Stage IV - highest energy)
- Lunate dislocates volarly as remaining carpus relocates back under the radius
- PA view: "piece of pie" sign (triangular shape of dislocated lunate)
- Lateral view: "spilled teacup" sign (lunate tilted into palm)
- Median nerve compression (acute carpal tunnel syndrome) is a recognized complication - a surgical emergency
5. Triangular Fibrocartilage Complex (TFCC) Tear
- The TFCC is the main stabilizer of the DRUJ and ulnar wrist
- Mechanism: axial load with forearm rotation, or FOOSH
- Ulnar-sided wrist pain; positive ulnocarpal stress test (pain on compression in ulnar deviation)
- Classified as traumatic (Palmer Type 1) or degenerative (Type 2)
- MRI or arthroscopy for diagnosis
D. Other / Soft Tissue Injuries
| Injury | Notes |
|---|---|
| Wrist sprain | Partial or complete ligament tear without instability; diagnosis of exclusion - always image first |
| DRUJ instability | Isolated or combined with distal radius fractures |
| Extensor tendon injury | May accompany dorsal fractures |
| Flexor tendon injury | Can follow hook of hamate non-union (FDP ring/small finger) |
| Median nerve injury | Acute carpal tunnel syndrome with lunate dislocation or distal radius fracture |
Age-Based Pattern Summary
| Patient | Most Likely Injury |
|---|---|
| Child | Torus/greenstick distal radius (physeal injury spares cartilaginous carpals) |
| Young active adult | Scaphoid fracture, SL ligament tear, perilunate dislocation |
| Elderly / osteoporotic | Colles' fracture (often intra-articular); proximal humerus is a close second |
Sources: Tintinalli's Emergency Medicine, Comprehensive Study Guide - Wrist Injuries chapter; Miller's Review of Orthopaedics 9th ed; Pye's Surgical Handicraft 22nd ed; ROSEN's Emergency Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.