Excellent — I have both key figures. Now I have all the material needed for a comprehensive response. Let me compile the full pharmacology of anti-anginal drugs.
Anti-Anginal Drugs — Pharmacology
Overview
Angina pectoris results from an imbalance between myocardial oxygen supply and demand. Atherosclerotic coronary disease is the most common underlying cause, though coronary vasospasm (Prinzmetal angina) also reduces perfusion. Anti-anginal drugs restore this balance by either reducing O₂ demand, increasing supply (coronary dilation), or both.
Types of Angina
| Type | Mechanism | Key Features |
|---|
| Stable (Classic) | Fixed atherosclerotic obstruction | Effort-induced; relieved by rest or nitroglycerin |
| Unstable | Plaque rupture + partial thrombosis | Rest angina, crescendo pattern; ACS |
| Prinzmetal (Vasospastic) | Coronary artery spasm | Occurs at rest; responds to nitrates and CCBs |
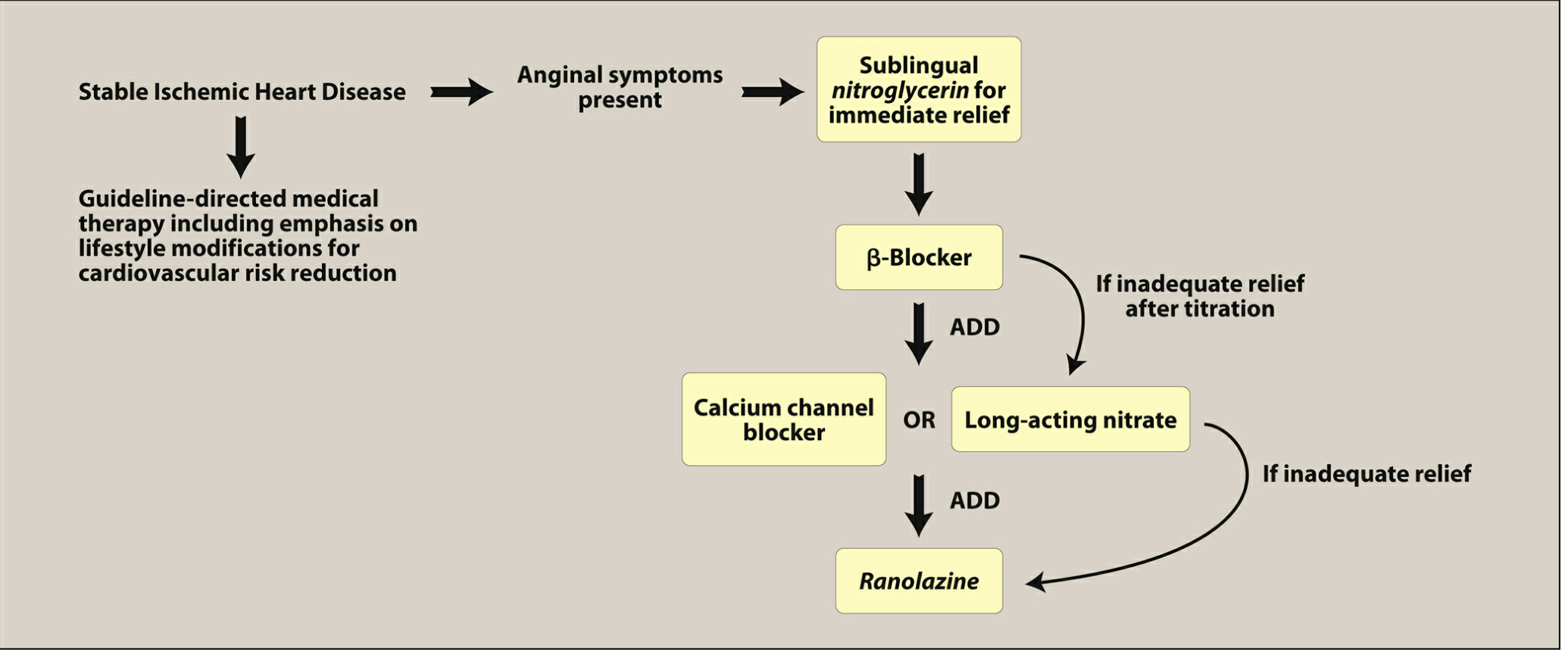
Treatment Algorithm
Fig. General treatment algorithm for stable angina — Lippincott Pharmacology, p. 416
Drug Classes
1. Organic Nitrates
Drugs: Nitroglycerin (NTG), Isosorbide dinitrate (ISDN), Isosorbide mononitrate (ISMN)
Mechanism of Action:
- Nitrates are converted to nitric oxide (NO) in vascular smooth muscle
- NO activates guanylyl cyclase → ↑ cGMP → activation of cGMP-dependent protein kinase → dephosphorylation of myosin light chain → smooth muscle relaxation
- Primary effect: venodilation (↓ venous return → ↓ preload → ↓ ventricular wall tension → ↓ O₂ demand)
- At higher doses: arteriolar dilation (↓ afterload)
- Also directly dilate coronary arteries, benefiting vasospastic angina and redistributing flow to ischemic subendocardium
Key point from Goodman & Gilman: When NTG is injected directly into the coronary artery, it does not abort angina induced by pacing — confirming that the dominant mechanism is preload reduction, not direct coronary dilation alone.
Preparations & Pharmacokinetics:
| Formulation | Route | Onset | Duration | Use |
|---|
| Nitroglycerin sublingual tablet/spray | SL | 1–3 min | 30 min | Acute attack |
| Nitroglycerin IV | IV | Immediate | During infusion | Unstable angina, ACS |
| Nitroglycerin transdermal patch | Transdermal | Hours | 24 h | Prophylaxis |
| Nitroglycerin buccal/sustained-release | Buccal/oral | — | Hours | Prophylaxis |
| Isosorbide dinitrate | Oral | 30 min | 4–6 h | Prophylaxis |
| Isosorbide mononitrate | Oral | Slow | 6–8 h | Prophylaxis |
- NTG and ISDN undergo extensive first-pass metabolism; ISMN does not (high oral bioavailability)
- NTG is highly lipophilic and readily absorbed through skin and mucous membranes
Nitrate Tolerance:
- Continuous nitrate exposure leads to tolerance (tachyphylaxis)
- Mechanism: depletion of sulfhydryl (-SH) groups required for NO bioactivation; upregulation of PDE
- Prevention: nitrate-free interval of 10–12 hours daily (e.g., remove patch at night)
Adverse Effects:
- Headache (vasodilation of meningeal vessels) — most common
- Orthostatic hypotension, reflex tachycardia
- Flushing
- Methemoglobinemia (high-dose IV NTG)
Contraindications:
- Concurrent use of PDE-5 inhibitors (sildenafil, tadalafil) — severe, potentially fatal hypotension
- Hypotension, hypovolemia
- Right ventricular infarction
- Hypertrophic obstructive cardiomyopathy (HOCM)
2. β-Adrenergic Blockers
Drugs:
- Non-selective: Propranolol, Nadolol, Sotalol
- Cardioselective (β₁): Atenolol, Bisoprolol, Metoprolol, Nebivolol
Mechanism of Action:
- Block β₁ receptors in the heart → ↓ heart rate (negative chronotropy) + ↓ contractility (negative inotropy) → ↓ myocardial O₂ demand
- Also reduce blood pressure, further lowering cardiac workload
- Reduce frequency and severity of angina attacks
- Increase exercise duration and tolerance in effort-induced angina
Clinical Use:
- First-line antianginal therapy for stable angina (unless contraindicated)
- Proven survival benefit after MI (reduce re-infarction and death)
- Improve mortality in heart failure with reduced ejection fraction (HFrEF)
- Cardioselective β₁-blockers are preferred to minimize side effects
- β-Blockers with intrinsic sympathomimetic activity (ISA) should be avoided in angina
Exception — Vasospastic angina: β-Blockers are ineffective and may worsen vasospastic/Prinzmetal angina (unopposed α-mediated vasoconstriction → increased spasm)
Adverse Effects:
- Bradycardia, AV block
- Bronchoconstriction (non-selective agents)
- Fatigue, depression
- Peripheral vasoconstriction
- Masked hypoglycemia in diabetics
- Impotence
Contraindications:
- Asthma/severe reactive airways disease (non-selective)
- Decompensated heart failure
- Significant bradycardia or AV block
- Vasospastic angina
3. Calcium Channel Blockers (CCBs)
Drugs:
- Dihydropyridines (DHP): Amlodipine, Nifedipine, Felodipine
- Non-dihydropyridines (non-DHP): Verapamil, Diltiazem
Mechanism of Action:
- Block voltage-gated L-type Ca²⁺ channels in vascular smooth muscle and cardiac muscle
- DHPs: Predominantly peripheral arterial vasodilation → ↓ afterload → ↓ O₂ demand; also dilate coronary arteries
- Non-DHPs (Verapamil, Diltiazem): Also suppress SA node automaticity and AV conduction (negative chronotropy and dromotropy) + negative inotropy
- Activity gradient (peripheral to myocardial): Amlodipine > Diltiazem > Verapamil
Clinical Use:
- All CCBs effective for stable and vasospastic angina
- First-line for Prinzmetal (vasospastic) angina — most effective
- DHPs used as add-on to β-blockers in stable angina
- Verapamil/diltiazem: alternative to β-blockers when β-blockers are contraindicated
Adverse Effects:
- DHPs: Reflex tachycardia (especially nifedipine), peripheral edema, flushing, headache
- Verapamil: Constipation, bradycardia, AV block, negative inotropy
- Diltiazem: Bradycardia, AV block (less than verapamil), less negative inotropy
Contraindications:
- Non-DHPs contraindicated in HFrEF (negative inotropy worsens function)
- Non-DHPs should not be combined with β-blockers (risk of severe bradycardia/AV block)
- Systolic blood pressure <90 mmHg
4. Ranolazine (Sodium Channel Blocker)
Drug: Ranolazine (RANEXA)
Mechanism of Action:
- Blocks late inward Na⁺ current (late I_Na) in ischemic myocardium
- Ischemia → ↑ late I_Na → intracellular Na⁺ overload → reversal of Na⁺/Ca²⁺ exchanger → intracellular Ca²⁺ overload → diastolic dysfunction and ischemic injury
- Blocking late I_Na → ↓ Ca²⁺ overload → improved diastolic relaxation → ↓ wall tension → ↓ O₂ demand
- Does not affect heart rate or blood pressure — hemodynamically neutral
- Also has mild anti-arrhythmic properties (decreases AF, SVT, ventricular arrhythmias)
Clinical Use:
- Used in patients with stable angina who have failed β-blockers, CCBs, or nitrates
- Can be used in combination with any of the above agents
- Provides additional antianginal benefit even on top of maximal conventional therapy
Adverse Effects:
- QT interval prolongation (risk of torsades de pointes)
- Dizziness, nausea, constipation
- Less effective in women
Drug Interactions:
- Strong CYP3A4 inhibitors (ketoconazole, clarithromycin) increase ranolazine levels
- P-glycoprotein inhibitors also increase levels
- Numerous interactions — check carefully before prescribing
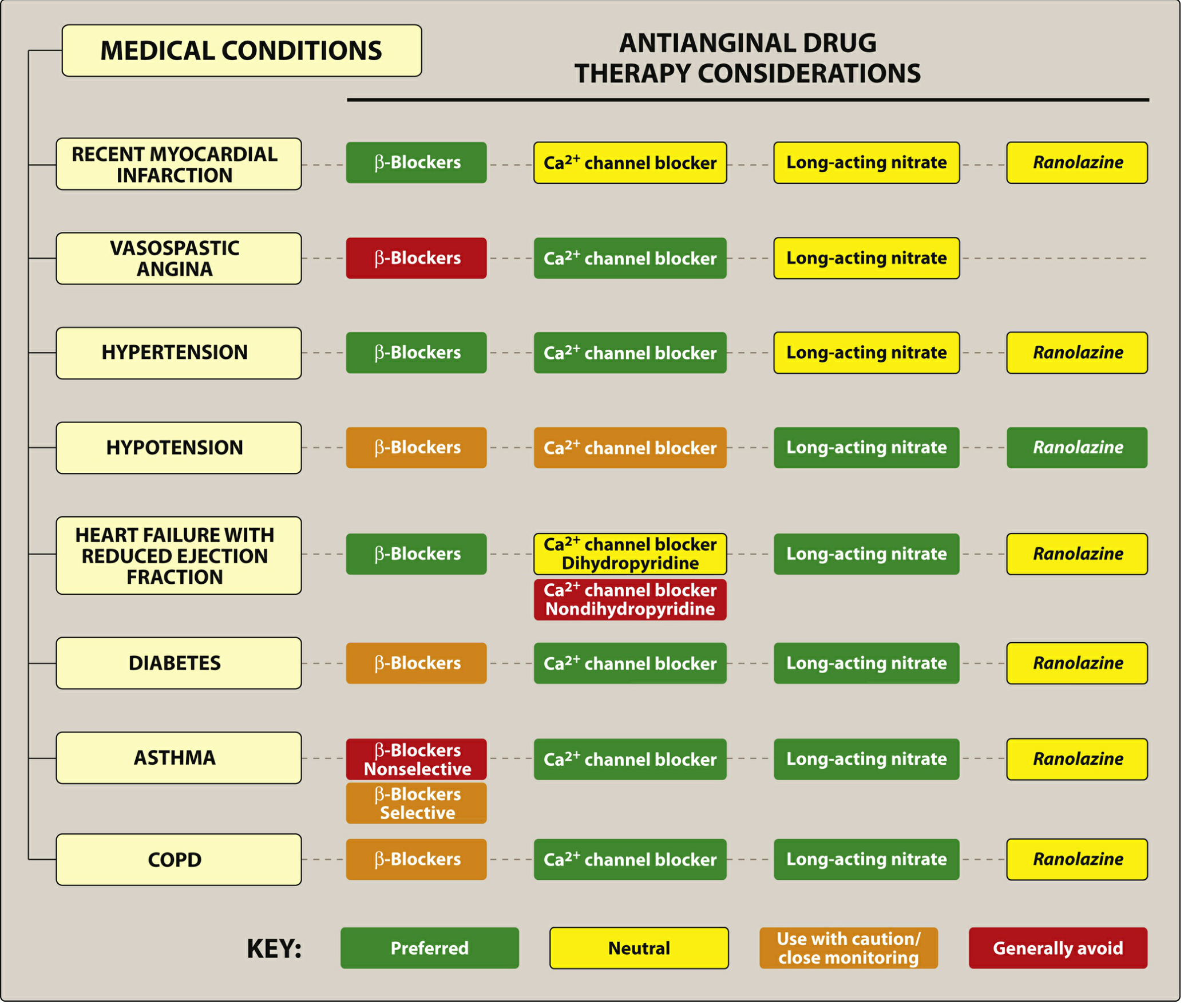
Antianginal Drug Therapy by Comorbidity
Fig. Antianginal therapy in patients with comorbidities — Lippincott Pharmacology, p. 417
Summary Comparison Table
| Drug Class | ↓ HR | ↓ Contractility | ↓ Preload | ↓ Afterload | Vasospastic Angina | 1st-Line for Stable Angina |
|---|
| Nitrates | ↑ (reflex) | — | +++ | + | ✓ | Acute relief only |
| β-Blockers | +++ | +++ | — | + | ✗ (contraindicated) | ✓ (first-line) |
| CCBs (DHP) | ↑ (reflex) | — | — | +++ | ✓✓ | Add-on |
| CCBs (non-DHP) | ++ | ++ | — | ++ | ✓✓ | Alternative |
| Ranolazine | — | — | — | — | — | Refractory cases |
Key Clinical Points
- Sublingual NTG (tablet or spray) must be prescribed to all angina patients for acute attack relief
- β-Blockers are first-line for stable angina (proven mortality benefit post-MI)
- CCBs (especially DHPs or diltiazem) are first-line for vasospastic angina; β-blockers are contraindicated in vasospasm
- Non-DHP CCBs (verapamil, diltiazem) are contraindicated in HFrEF due to negative inotropy
- Nitrate tolerance is prevented by a 10–12 hour nitrate-free interval daily
- Nitrates + PDE-5 inhibitors = dangerous — absolutely contraindicated combination
- Ranolazine is reserved for refractory angina; prolongs QT and has extensive drug interactions
- Combination therapy (β-blocker + CCB or nitrate) is used when monotherapy is inadequate
Sources: Lippincott Illustrated Reviews: Pharmacology, pp. 411–425 | Goodman & Gilman's The Pharmacological Basis of Therapeutics, pp. 626–690