Anti CCP antibody
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Searching PubMed
"anti-CCP" OR "anti-cyclic citrullinated peptide" rheumatoid arthritis
Reading File
Reading File
Loading Image
Here is a comprehensive overview of Anti-CCP (Anti-Cyclic Citrullinated Peptide) Antibody:
Anti-CCP Antibody (ACPA — Anticitrullinated Protein/Peptide Antibody)
What Is It?
Anti-CCP belongs to a broader class called anticitrullinated protein/peptide antibodies (ACPAs). These are autoantibodies directed against proteins or peptides in which the amino acid arginine has been post-translationally converted to citrulline by the enzyme peptidylarginine deiminase (PAD). The test is performed by ELISA; the reference value is < 20 U/mL.
Pathogenesis — Why Does Citrullination Matter?
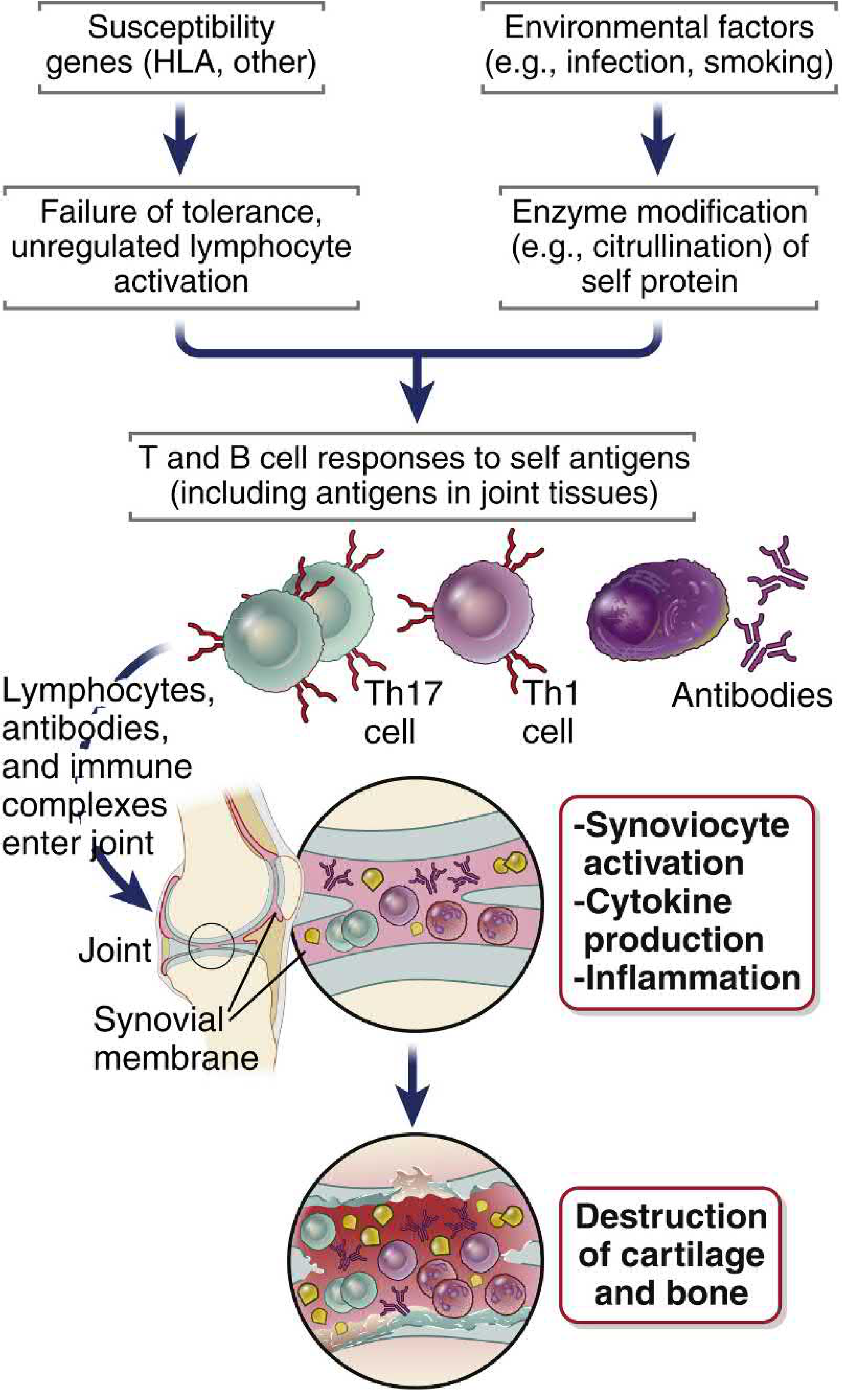
Environmental triggers (notably smoking and certain infections) induce citrullination of self-proteins in mucosal sites (especially the respiratory tract). Because citrullinated neoantigens are not normally present, central tolerance to them may be absent. In genetically susceptible individuals — those carrying HLA-DRB1 "shared epitope" alleles — these modified peptides bind with altered avidity to the HLA molecule, activating self-reactive T cells.
The resulting immune response involves:
- Th17 and Th1 cells secreting cytokines that recruit leukocytes into joints
- B cells producing ACPAs
- Synoviocyte activation → collagenase release → cartilage and bone destruction
- Formation of tertiary lymphoid organs in the synovium, perpetuating local inflammation
Importantly, this cascade begins up to 10 years before clinically detectable disease.
— Cellular and Molecular Immunology, p. 1281–1282; Goldman-Cecil Medicine, p. 2785
Diagnostic Performance
| Parameter | Value |
|---|---|
| Sensitivity | 60–80% |
| Specificity | 85–99% |
| Reference range | < 20 U/mL |
Anti-CCP is more specific than Rheumatoid Factor (RF) for RA. RF has sensitivity ~54–88% but specificity only 48–92%, whereas anti-CCP achieves specificity up to 99% by some assays.
Combining RF + anti-CCP has higher diagnostic yield than either alone.
— Textbook of Family Medicine 9e, p. 239; Robbins & Kumar Basic Pathology, p. 805
Clinical Utility
1. Diagnosis of RA
- Included in the 2010 ACR/EULAR classification criteria for RA (along with RF)
- Most useful when:
- Clinical diagnosis is uncertain
- RF is negative (seronegative RA): anti-CCP can be positive
- Early disease — ACPAs can precede clinical RA by several years
2. Prognosis
- Positive anti-CCP is associated with:
- More aggressive disease course
- Greater radiologic joint erosion and destruction
- Worse long-term functional outcomes
- Some studies show ACPA levels correlate with response to anti-TNF therapy
3. Predicting RA Development
- ACPAs have been detected in serum years before the onset of symptoms, making them a potential marker for pre-clinical RA
4. Pediatric Use
- In children, primarily associated with polyarticular RF-positive JIA (juvenile idiopathic arthritis)
- When positive in JIA, indicates more erosive disease
— Harriet Lane Handbook 23e, p. 924; Textbook of Family Medicine 9e, p. 879
Causes of False Positives
Anti-CCP is not entirely specific to RA. It can be positive in:
- Active tuberculosis
- Other autoimmune conditions
- Occasionally in healthy individuals
Comparison with Rheumatoid Factor
| Feature | Rheumatoid Factor | Anti-CCP |
|---|---|---|
| Target | Fc portion of IgG | Citrullinated peptides |
| Sensitivity for RA | ~70% (54–88%) | 60–80% |
| Specificity for RA | ~85% (48–92%) | 85–99% |
| Other diseases | Sjögren's, SLE, chronic infections | TB, rare autoimmune |
| Prognostic value | Yes (high titer = severe disease) | Yes (erosive disease) |
| Isotype measured | IgM (primarily) | IgG (primarily) |
| Pre-clinical detection | Limited | Yes — years before onset |
Key Takeaway
Anti-CCP is the most specific serologic marker currently available for RA and is superior to RF in discriminating RA from other inflammatory conditions. A positive result in a patient with early arthritis significantly increases the probability of RA and warrants prompt rheumatologic evaluation and initiation of DMARDs.
This is a shared conversation. Sign in to Orris to start your own chat.