Explain the surgical anatomy of the anus and rectum, the physiology of defecation and continence, anatomical landmarks, and relationships relevant to anorectal surgery. Discuss common anorectal conditions (e.g., hemorrhoids, fistulas, fissures) and skills in examining and diagnosing anorectal conditions.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full, detailed response.
Surgical Anatomy, Physiology, and Clinical Conditions of the Anus and Rectum
1. Surgical Anatomy of the Anorectum
The Rectum
The rectum begins at the rectosigmoid junction (approximately at the level of S3) and ends at the anorectal junction, a total length of roughly 12-15 cm. Unlike the colon, the rectum's longitudinal muscle layer is not organized into teniae coli - instead it forms a uniform, continuous outer coat that encircles the bowel and extends distally to insinuate between the internal and external anal sphincters all the way to the distal anal canal.
The rectum has three lateral curves that produce the transverse rectal folds (valves of Houston) visible internally. These folds, along with the rectal curvatures themselves, are anatomical landmarks used during proctoscopy and contribute passively to continence.
Perirectal spaces relevant to surgery:
- Ischiorectal (ischioanal) fossa - lateral to the external sphincter, filled with fat; site of ischiorectal abscesses
- Intersphincteric space - between IAS and EAS; the origin of most cryptoglandular abscesses
- Deep postanal space - posterior to the external sphincter, below the levator ani; connects the two ischiorectal fossae and is the origin of "horseshoe" abscesses
- Supraelevator space - above the levator ani; infection here may arise from upward extension of intersphincteric abscess or from intraabdominal pathology
The Anal Canal
The anal canal is 3-4 cm long and is kept closed at rest as an anteroposterior slit by tonic muscular contraction. Key landmarks from proximal to distal:
| Landmark | Position | Significance |
|---|---|---|
| Anorectal junction | Proximal end of the canal | Level of the puborectalis sling; palpable as the "anorectal ring" on digital exam |
| Dentate (pectinate) line | Mid-canal | Embryological junction of endoderm/ectoderm; superior = columnar mucosa (visceral pain), inferior = squamous anoderm (somatic pain) |
| Columns of Morgagni | Longitudinal mucosal folds above dentate line | Between them lie the anal crypts where anal glands open |
| Anal verge | Distal end | Junction of anal skin and perianal skin |
The dentate line is the single most important anatomical landmark in anorectal surgery. Above it: visceral innervation (insensate to sharp pain), lymphatics drain to mesenteric/internal iliac nodes, venous drainage to portal system (internal hemorrhoids originate here). Below it: somatic innervation via the pudendal nerve (exquisitely pain-sensitive), lymphatics drain to inguinal nodes, venous drainage to systemic circulation (external hemorrhoids originate here).
The Sphincter Complex
Internal Anal Sphincter (IAS):
- A thickened continuation of the circular smooth muscle of the rectum
- Under involuntary control; receives inhibitory innervation from enteric inhibitory motor neurons, plus extrinsic input from lumbar sympathetics and sacral parasympathetics via the pelvic plexus
- Responsible for approximately 70% of resting anal tone
- Produces the rectoanal inhibitory reflex (RAIR) - relaxes reflexively when the rectum is distended
External Anal Sphincter (EAS):
- Striated (voluntary) muscle; located distal to but partly overlapping the IAS
- Innervated by the pudendal nerve (S3-S4)
- Contributes high resting tone, but uniquely it can be voluntarily contracted to augment continence under threat of urgency
- Responsible for most voluntary squeeze pressure
Puborectalis:
- A U-shaped sling of striated muscle forming part of the levator ani complex
- Wraps around the anorectal junction, pulling the rectum anteriorly and maintaining the anorectal angle (approximately 90° at rest)
- Its tonic contraction creates a mechanical barrier preventing stool from entering the upper anal canal
- Innervated by direct branches of S3-S4 and the pudendal nerve
The Conjoined Longitudinal Muscle
The longitudinal muscle coat of the rectum joins with fibers of the puborectalis and levator ani at the anorectal junction, then travels distally as the conjoined longitudinal muscle between the IAS and EAS. Its terminal fibers spread out into the perianal skin as the corrugator cutis ani, creating the puckered appearance of the perianal skin.
Neurovascular Supply
Blood supply:
- Superior rectal artery (from the inferior mesenteric artery) - main supply to the upper rectum
- Middle rectal arteries (from internal iliac) - supply the mid-rectum
- Inferior rectal arteries (from the internal pudendal) - supply the anal canal and sphincters
Venous drainage:
- Internal hemorrhoidal plexus drains via the superior rectal vein to the portal system
- External hemorrhoidal plexus drains via the inferior rectal veins to the systemic circulation
- The two communicate at the anorectal junction, representing a portosystemic anastomosis
Nerve supply:
- Pudendal nerve (S2-S4): somatic motor (EAS, pelvic floor) and sensory (anoderm and perianal skin)
- Pelvic parasympathetics (S2-S4, nervi erigentes): motor to rectum; sensory (stretch receptors in rectal wall; these carry the urge to defecate)
- Lumbar sympathetics (L1-L3, hypogastric nerve): modulate motility and sphincter tone
- The presacral (superior hypogastric) plexus lies anterior to the sacrum - damage during rectal dissection causes ejaculatory dysfunction in men
2. Physiology of Defecation and Continence
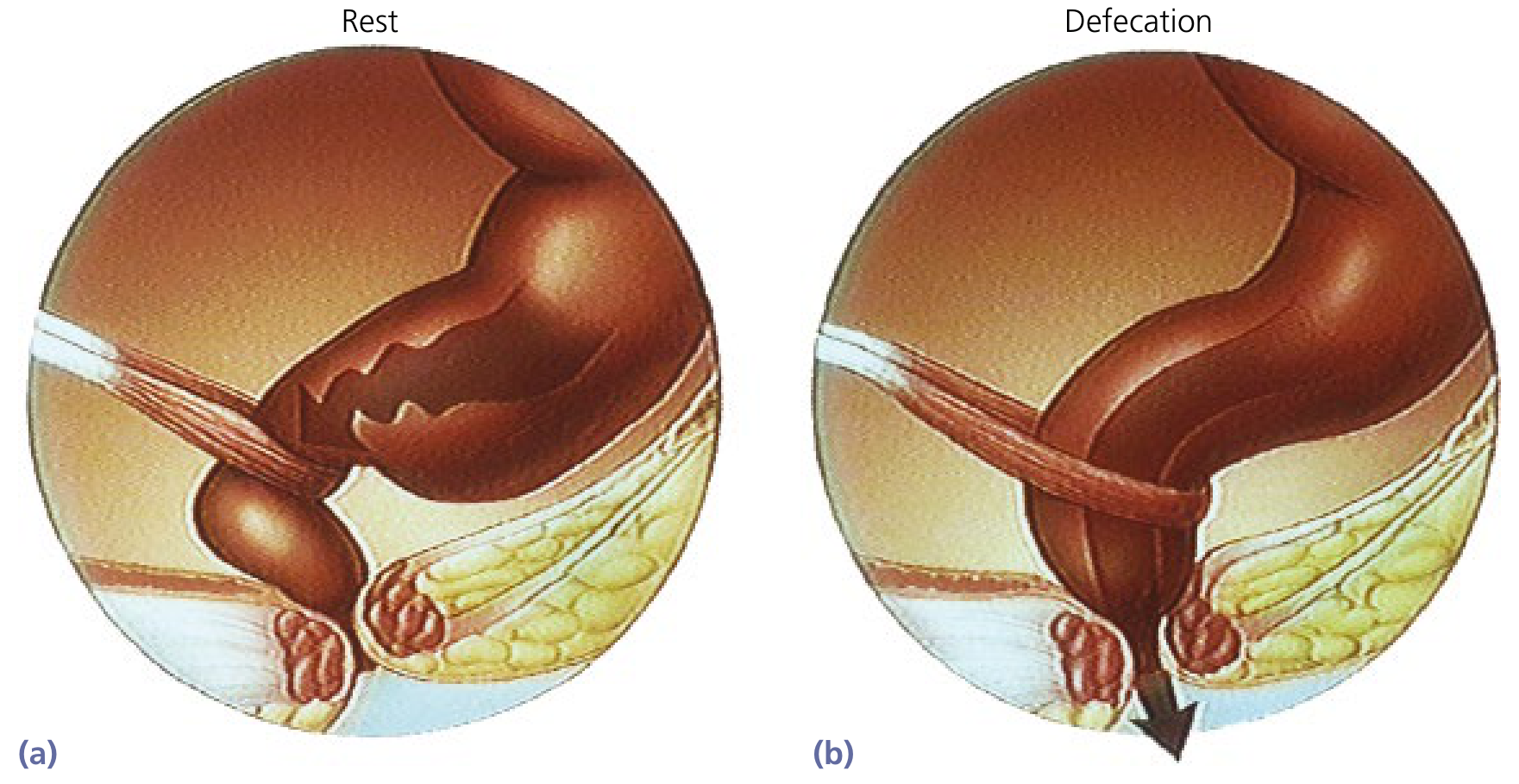
Anorectum at rest (a) and during defecation (b). The puborectalis and sphincters relax, opening the canal and permitting perineal descent (Yamada's Textbook of Gastroenterology, 7th ed.).
Defecation
Defecation is a coordinated, multi-step process:
- Mass movement - high-amplitude propagated contractions (HAPCs) of the colon, occurring 4-10 times per day (especially after meals/awakening), propel fecal material into the rectum
- Rectal distension - triggers the rectoanal inhibitory reflex (RAIR): the IAS reflexively relaxes, allowing luminal contents to make contact with the sensory epithelium of the upper anal canal (the "sampling reflex" - permits discrimination of solid, liquid, or gas)
- Accommodation - if defecation is inconvenient, the rectum relaxes (accommodates) and the urge dissipates
- Voluntary defecation - when socially appropriate: intra-abdominal pressure is raised by a Valsalva maneuver, the puborectalis muscle relaxes (straightening the anorectal angle), and both sphincters relax, directing expulsive force along the axis of the rectum and canal
Continence
Fecal continence requires the integrated function of multiple systems:
- Rectal compliance - adequate distensibility allows large volumes to be stored at low pressure; poor compliance (e.g., after radiation, IBD) leads to urgency and incontinence
- IAS tone - provides 70% of resting pressure; passive, involuntary barrier
- EAS and puborectalis tone - voluntary augmentation when urgency threatens; the puborectalis angle is tighter during squeeze, adding a mechanical flutter-valve effect
- Anal sensation - the anoderm and sampling zone above the dentate line allow discrimination of stool consistency and warn of impending leakage; neuropathy degrades this
- Vascular cushions (hemorrhoidal tissue) - the spongy vascular pads at the 3, 7, and 11 o'clock positions contribute to fine-tuning anal closure by filling the canal; they account for approximately 15-20% of resting tone
- Stool consistency - formed stool is more easily retained; loose stool challenges all continence mechanisms
Impaired continence results from: poor rectal compliance, sphincter injury (IAS or EAS), pudendal neuropathy (obstetric, chronic straining), or cognitive/mobility deficits.
3. Common Anorectal Conditions
3.1 Hemorrhoids
Anatomy and pathophysiology: Hemorrhoids are normal vascular cushions present in all adults, located at the left lateral (3 o'clock), right posterior (7 o'clock), and right anterior (11 o'clock) positions. They are dilated vascular channels between the anal mucosa and the underlying IAS. Symptoms arise when these cushions lose their connective tissue support (increased circulating matrix metalloproteinases), prolapse, and become susceptible to trauma. Risk factors include constipation, loose stools, prolonged straining, and pregnancy.
Classification:
- Internal hemorrhoids - above the dentate line; covered by columnar/transitional mucosa; painless unless thrombosed or strangulated
- External hemorrhoids - below the dentate line; covered by squamous anoderm; painful when thrombosed (somatic innervation)
Grading of internal hemorrhoids:
| Grade | Description |
|---|---|
| I | Bleed; may be enlarged; no prolapse |
| II | Prolapse with straining; reduce spontaneously |
| III | Prolapse; require manual reduction |
| IV | Irreducibly prolapsed; cannot be reduced |
Symptoms: Painless bright red rectal bleeding (on tissue, dripping into toilet), prolapse, mucus discharge, perianal moisture, pruritus. Pain is uncommon unless thrombosis occurs.
Diagnosis: History and physical examination including gentle anal eversion; anoscopy (beveled or slotted anoscope) is the definitive diagnostic tool; hemorrhoids may also be seen on flexible sigmoidoscopy in retrograde view.
Treatment:
- Grades I-III: dietary fiber (20-30 g/day), increased fluid intake, sitz baths, avoidance of prolonged straining. Phlebotonics (e.g., diosmin, flavonoids) improve venous tone and reduce bleeding
- Grades II-III resistant to medical therapy: rubber band ligation (RBL) is the most common office procedure; creates scarring that fixes mucosa to underlying tissue
- Alternative office procedures: sclerotherapy, infrared photocoagulation, suture ligation
- Grade IV / refractory grade III / strangulation: hemorrhoidectomy (excisional; Ferguson or Milligan-Morgan technique); Doppler-guided hemorrhoidal artery ligation (DGHAL)
- Thrombosed external hemorrhoid: sitz baths, topical analgesia; excision (not just incision) within 72 hours if acutely painful
3.2 Anal Fissure
Pathophysiology: A longitudinal tear (with ulceration) of the anoderm just inside the anal margin. The underlying mechanism is hypertonia of the IAS, reducing anodermal blood flow - especially at the posterior midline, where cadaveric studies show the least arterial perfusion. This creates an ischemic wound that cannot heal.
Location: >90% occur in the posterior midline; approximately 10% anterior (more common in women, often obstetric). An "off-midline" fissure must raise suspicion for Crohn disease, TB, syphilis, HIV, leukemia, or squamous cell carcinoma, and warrants examination under anaesthesia, culture, and biopsy.
Clinical features:
- Severe pain during and after defecation ("passing razor blades" or "cut glass")
- Pain may persist for hours after the bowel movement
- Small amount of bright red blood (streaking tissue or stool)
- Chronic fissure (>6-8 weeks): associated with a sentinel skin tag (distal) and a hypertrophied anal papilla (proximal at the dentate line); fibrotic, rolled margins; visible IAS fibers at the base

Anal fissure with inflammatory changes at the anal margin (Goldman-Cecil Medicine).
Diagnosis: Usually made clinically by gently applying opposing traction to the buttocks - the fissure is visible without instrumentation. Digital exam and anoscopy are deferred until healing to avoid severe pain. Examination under anaesthesia (EUA) is needed for atypical fissures.
Treatment:
| Acuity | First Line | Second Line | Definitive |
|---|---|---|---|
| Acute | High-fiber diet, fluids, sitz baths | -- | -- |
| Chronic | As above + topical 0.2-0.4% glyceryl trinitrate (GTN) or topical calcium channel blocker (0.3% nifedipine or 2% diltiazem) | Botulinum toxin A injection into the IAS | Lateral internal sphincterotomy (LIS) - >90% long-term healing; risk of incontinence |
Note: GTN causes headache in up to 20%; calcium channel blockers have fewer side effects. Botulinum toxin is effective but expensive and results are less durable. LIS, while the most effective surgical option, carries a small but real risk of incontinence (especially gas and liquid stool), which is important to discuss with patients.
3.3 Anorectal Abscess and Fistula
These represent the acute and chronic manifestations of the same suppurative process.
Pathogenesis (cryptoglandular theory): Anal glands arise from the anal canal at the level of the crypts of Morgagni, penetrate through the IAS, and empty into the intersphincteric space. Fecal plugging or trauma to these ducts causes suppuration, forming an abscess in the intersphincteric space that then tracks along anatomical planes.
Classification of abscesses by space:
- Perianal - most common; subcutaneous at the anal verge; often points externally
- Intersphincteric - between IAS and EAS; exquisitely tender on rectal exam; may not have obvious external signs (diagnosis often requires EUA)
- Ischiorectal - lateral; large volume of pus; fluctuant buttock swelling; fever and leukocytosis common
- Supraelevator - above levator ani; pelvic source or upward extension; palpable on rectal or vaginal exam
- Horseshoe abscess - originates in the posterior intersphincteric space, extends into the deep postanal space and both ischiorectal fossae bilaterally
Classification of fistulas (Parks classification):
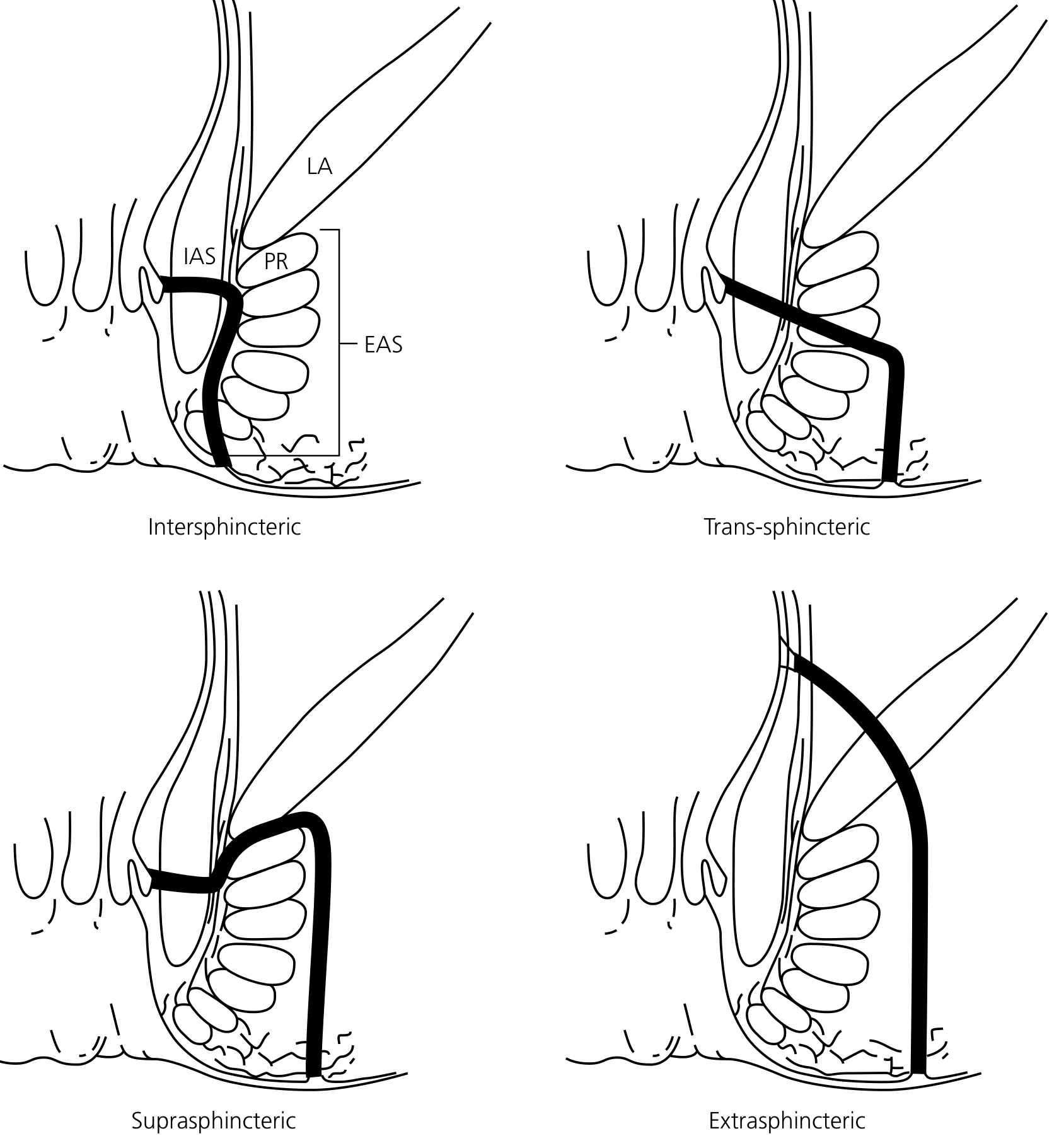
Parks classification of anorectal fistulas (Yamada's Textbook of Gastroenterology, 7th ed.)
| Type | Course | Continence risk |
|---|---|---|
| Intersphincteric (most common ~70%) | Tracks between IAS and EAS to perianal skin | Low - fistulotomy safe |
| Transsphincteric (~25%) | Passes through EAS into ischiorectal fossa | Moderate - partial sphincter division |
| Suprasphincteric (~5%) | Up through intersphincteric plane, over puborectalis, down to ischiorectal fossa | High - complete sphincter division |
| Extrasphincteric (<1%) | From rectum through levator ani; bypasses sphincters entirely | Very high - total continence loss if divided |
Goodsall's rule predicts fistula anatomy: external openings posterior to the transverse anal line have curved tracts leading to a single internal opening in the posterior midline; anterior openings follow a straight radial path to the nearest crypt.
Clinical features of abscess: Gradual onset of perianal pain, pressure, and fullness, worsened by sitting or defecation; fever; malaise. The pattern of external signs depends on the anatomical space involved.
Clinical features of fistula: Intermittent or persistent purulent or blood-stained discharge from an external opening; recurring abscess episodes; mild perianal discomfort.
Treatment:
- Abscess: Prompt surgical incision and drainage (I&D); incision placed as close to the anal verge as possible. Antibiotics alone are inadequate; they are indicated post-drainage only in immunocompromised patients, diabetics, or those with cellulitis
- Simple low fistula (intersphincteric, low transsphincteric): Fistulotomy - laying open the tract; curative in >90% when <30% of sphincter is involved
- Complex / high fistula: Seton placement (draining or cutting) to allow progressive sphincter division with fibrosis; endorectal advancement flap; LIFT (ligation of intersphincteric fistula tract); fibrin glue (low success rate); fistula plug
- Crohn-related fistulas: Anti-TNF biologic therapy (infliximab) heals fistulas in up to 60%; seton drainage as a bridge; surgical options reserved for failure of medical therapy
4. Examination Skills and Diagnosis of Anorectal Conditions
History Taking
Key elements of an anorectal history:
- Bleeding: bright red vs. dark; amount; relationship to defecation (on tissue only, dripping, mixed with stool); associated pain
- Pain: onset, character, relation to defecation, duration after stooling
- Prolapse or protrusion: onset; reducible spontaneously vs. manually vs. irreducible
- Discharge: purulent, mucoid, bloody
- Continence: ability to control gas, liquid, solid stool; urgency
- Stool habits: constipation, diarrhea, straining, stool consistency
- Obstetric/surgical history: vaginal deliveries, prior anorectal operations
- Family history: IBD, colorectal cancer
- Medications: constipating agents, anticoagulants, immunosuppressants
Positioning
The patient is placed in the left lateral (Sims) position or prone jackknife position on the examination table. The prone jackknife position offers better visualization and is preferred in the operating room. A lithotomy position is used when simultaneous vaginal examination is needed.
Inspection
Gently apply opposing traction to the buttocks with both hands. Inspect for:
- Skin tags, external hemorrhoids, fistula openings
- Fissures (posterior midline primarily)
- Prolapsing tissue (ask the patient to strain or bear down)
- Perianal soiling, excoriation
- Asymmetry, swelling, erythema, induration (abscess)
- Condylomata, tumors
Digital Rectal Examination (DRE)
A well-lubricated, gloved index finger is gently inserted into the anal canal. Assess:
- Resting tone (IAS function) and squeeze pressure (EAS and puborectalis)
- The anorectal ring (puborectalis sling) - an important landmark felt posteriorly at the anorectal junction; inadvertent division = complete incontinence
- Rectal wall for masses, tenderness, induration
- Prostate (in men) and cervix/posterior uterus (in women)
- Contents of the rectal vault (stool, blood)
- Ask the patient to bear down to assess descent and prolapse dynamics
- Check the finger for blood, mucus, or stool on withdrawal
If severe perianal pain prevents examination (e.g., acute fissure, intersphincteric abscess), do not force it - examination under anaesthesia is appropriate.
Anoscopy
The workhorse of anorectal office examination:
- Insert lubricated anoscope with obturator in place; remove obturator once seated
- Rotate 90° and repeat to visualize all four quadrants
- Internal hemorrhoids appear as purplish-red cushions above the dentate line; ask patient to strain to assess degree of prolapse
- Dentate line, anal crypts, and papillae are assessed
- Fissures are visible but examination is usually deferred if the patient is in severe pain
- Enables rubber band ligation and sclerotherapy of hemorrhoids in the office setting
Rigid Proctoscopy
- Standard instrument is 25 cm long; diameters of 15 or 19 mm for routine use (11 mm "pediatric" for strictures)
- Allows inspection of the rectum and distal sigmoid
- Must be used with suction for adequate visualization
- Useful for biopsy, polyp removal, evaluation of radiation proctitis or rectal tumors
- Transanal endoscopic microsurgery (TEM) and TAMIS (transanal minimally invasive surgery) use wider-diameter platforms for resection of larger lesions
Flexible Sigmoidoscopy and Colonoscopy
- Flexible sigmoidoscope (60 cm): left-sided colonic and rectal evaluation; no sedation typically needed; 1-2 enema preparations
- Colonoscope (100-160 cm): full colonic and terminal ileal evaluation; requires complete bowel preparation and conscious sedation
- Both allow biopsy, polypectomy, and therapeutic intervention
- Internal hemorrhoids may be seen on retrograde view
- Mandatory when rectal bleeding is atypical, in patients >50, or when proximal pathology is suspected
Ancillary Investigations
| Test | Indication |
|---|---|
| Anorectal manometry | Assess IAS and EAS pressures, RAIR, rectal sensation, and compliance (incontinence, constipation, pre-operative sphincter function) |
| Endoanal ultrasound | Identify sphincter defects (obstetric injury), fistula anatomy |
| MRI pelvis | Best for mapping complex fistulas, Crohn perianal disease, rectal tumors |
| Defecography/MRI defecography | Assess pelvic floor dynamics, rectocoele, intussusception |
| Pudendal nerve terminal motor latency (PNTML) | Detect pudendal neuropathy contributing to incontinence |
Summary Table: Key Differential Features
| Condition | Pain | Bleeding | External sign | Key investigation |
|---|---|---|---|---|
| Internal hemorrhoid | None (unless thrombosed) | Bright red, painless | Prolapse on strain | Anoscopy |
| External hemorrhoid (thrombosed) | Severe, acute | Minor | Tender blue-black lump at verge | Clinical |
| Anal fissure | Severe, post-defecation | Streak, bright red | Sentinel tag, visible tear | Clinical inspection |
| Perianal abscess | Constant, throbbing | None | Tender fluctuant swelling | Clinical; CT/MRI if deep |
| Fistula-in-ano | Mild-moderate | Purulent discharge | External opening, skin scarring | EUA, MRI |
| Rectal prolapse | Discomfort | Mucus, blood | Full-thickness extrusion on straining | Clinical, defecography |
Sources:
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Chapter: Anorectal Anatomy and Innervation / Hemorrhoids / Anal Fissure
- Schwartz's Principles of Surgery, 11th ed., Chapter: Motility, Defecation, and Continence / Clinical Evaluation
- Yamada's Textbook of Gastroenterology, 7th ed., Chapter: Physiology of Continence and Defecation / Anorectal Abscess and Fistula / Hemorrhoids
- Goldman-Cecil Medicine, Chapter: Anal Fissure
- Mulholland and Greenfield's Surgery, 7th ed., Chapter: Anorectal Abscess/Fistula
This is a shared conversation. Sign in to Orris to start your own chat.