Discuss management of spontaneous CSF Rhinorrhea in a middle aged female. Ms ent University exam pattern for 20 marks. With diagrams wherever necessary.
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Searching PubMed
"spontaneous CSF rhinorrhea" AND "endoscopic repair" AND "intracranial hypertension"
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I now have all the material needed for a thorough, exam-quality answer. Let me compose the full 20-mark response:
Management of Spontaneous CSF Rhinorrhea in a Middle-Aged Female
[MS ENT University Examination - 20 Marks]
Introduction and Clinical Relevance
Spontaneous CSF rhinorrhea refers to leakage of cerebrospinal fluid through the anterior skull base into the nasal cavity in the absence of accidental trauma or recent surgery. This entity has special clinical significance in the context of a middle-aged female because such patients have a strong overlap with Benign Intracranial Hypertension (BIH) / Idiopathic Intracranial Hypertension (IIH) - a condition predominantly affecting obese middle-aged women. Studies show that 72-82% of patients with apparent spontaneous CSF rhinorrhea fulfill diagnostic criteria for BIH, and up to 82% have an elevated BMI. Understanding this association is the cornerstone of proper management.
Classification of CSF Rhinorrhea
Box: Classification of CSF Rhinorrhea (Ommaya's Classification)
I. TRAUMATIC
A. Accidental
1. Immediate
2. Delayed
B. Surgical
1. Neurosurgical (transsphenoidal, craniotomy)
2. Rhinologic (sinus surgery, septoplasty)
II. NONTRAUMATIC
A. Elevated Intracranial Pressure
1. Intracranial neoplasm
2. Hydrocephalus
3. Benign Intracranial Hypertension (BIH/IIH) ← KEY in middle-aged women
B. Normal Intracranial Pressure
1. Congenital anomaly
2. Skull base neoplasm
3. Erosive processes (osteomyelitis, granulomatosis)
4. Idiopathic (true spontaneous)
Spontaneous CSF rhinorrhea is best reserved for cases where investigation reveals no specific etiology, though most have occult elevated ICP.
Pathophysiology (Special Emphasis for Middle-Aged Females)
CSF is produced by the choroid plexus at 20 mL/hour (480 mL/day), with a total volume of ~140 mL (20 mL ventricles + 50 mL intracranial subarachnoid space + 70 mL paraspinal space). Normal ICP is up to 14 cm H₂O in adults.
For a CSF fistula to form, two conditions must coexist:
- A defect in the dura, arachnoid, intervening bone, and sinus mucosa
- A pressure gradient to drive CSF outward
In the middle-aged obese female:
- IIH/BIH causes chronically elevated ICP
- Pulsatile CSF pressure remodels the skull base - typically the cribriform plate, lateral lamella of the cribriform plate, or lateral recess of the sphenoid sinus (via arachnoid granulations)
- An empty sella (seen in 100% of spontaneous vs. 11% of nonspontaneous CSF leaks) reflects arachnoid/CSF herniation into the sella from elevated ICP - a radiologic marker
- Common sites: cribriform plate (most common), ethmoid roof, sphenoid sinus lateral recess
Key fact for exam: When the patient is actively leaking, the opening pressure at lumbar puncture may appear normal (the leak acts as a "safety valve" decompressing ICP). After surgical repair, the true elevated ICP becomes unmasked.
Clinical Features
History:
- Unilateral, watery, clear nasal discharge - typically worse on leaning forward (positional)
- Intermittent - "on and off" until the defect is surgically repaired
- Salty or sweet taste (CSF has low glucose but patient may perceive sweetness)
- Headache (may relate to underlying IIH)
- Risk of ascending meningitis (presents as fever, neck stiffness, photophobia)
- History of obesity, headaches, pulsatile tinnitus, or visual disturbance (IIH features)
Signs:
- "Reservoir sign" or "Halo sign" (ring test) - CSF forms a clear ring around blood on filter paper
- Papilledema (suggests elevated ICP/IIH)
- Middle-aged, obese female body habitus
Investigations / Diagnosis
Diagnosis proceeds in two steps: confirmation of CSF, then localization of the defect.
Step 1: Confirm the Fluid is CSF
| Test | Details | Sensitivity |
|---|---|---|
| β-2 Transferrin | Gold standard - electrophoretic identification of this CSF-specific isoform | Highly specific (~99%), preferred test |
| β-Trace protein (β-TP) | Prostaglandin-D-synthase; rapidly rising as a confirmatory test | High specificity |
| Glucose (>30 mg/dL) | Simple, but poor sensitivity/specificity (lacrimal fluid also positive) | Low |
| Halo/ring test | Double ring on filter paper | Unreliable (not specific) |
β-2 Transferrin is the investigation of choice - it is specific to CSF, perilymph, and vitreous humor.
Step 2: Localize the Defect
(a) High-Resolution CT of the Paranasal Sinuses (HR-CTPNS):
- First-line imaging
- Identifies bony defects, opacified sinuses, encephaloceles
- Best for bony detail; may miss soft tissue/dural defects
- Non-contrast CT is often the only investigation needed to identify the site
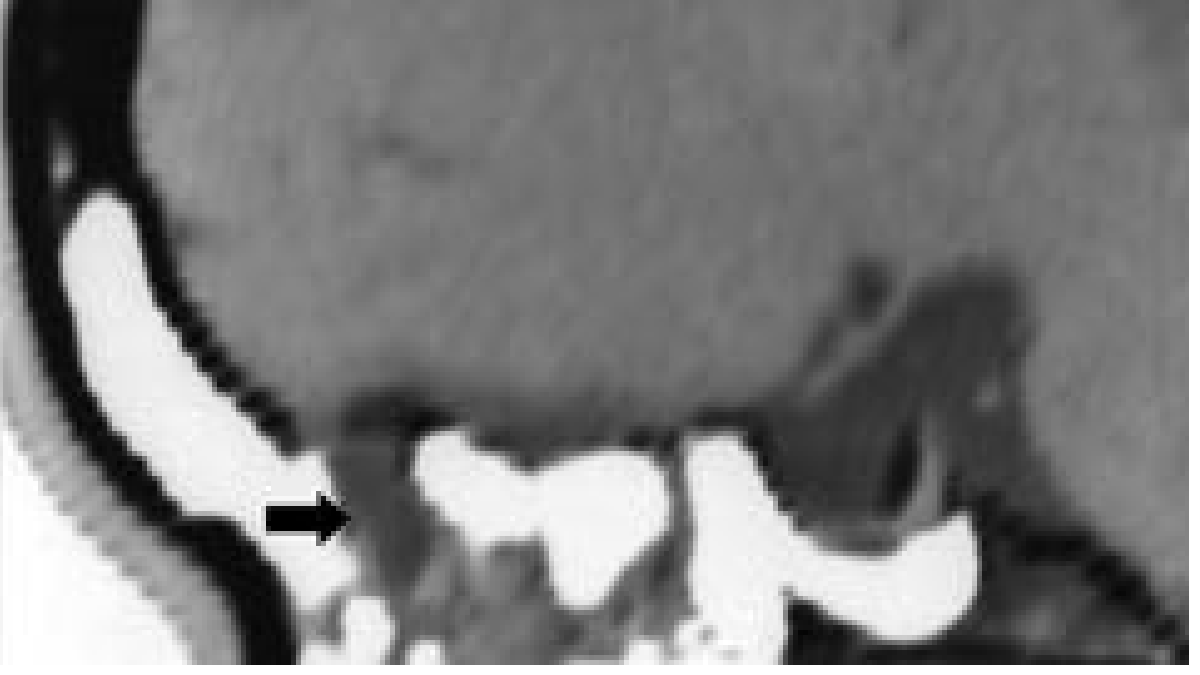
Fig. 1: CT Cisternography - contrast material within the ethmoid sinuses (arrow) confirming CSF fistula. Sagittal reconstruction shows direct continuity of contrast from the subarachnoid space to the sinuses. (Cummings Otolaryngology)
(b) MR Cisternography (MRC):
- Non-invasive, no radiation, no intrathecal contrast needed
- Heavily T2-weighted with fat suppression and video reversal
- Identifies soft tissue defects, meningoencephaloceles, empty sella, and opacification
- Can detect intermittent leaks and distinguishes CSF from mucus
(c) CT Cisternography (CTC):
- Intrathecal metrizamide + CT
- ~80% sensitivity for active leaks
- Defines precise site of communication
- Requires active leak at time of imaging
(d) Intrathecal Fluorescein:
- 0.1 mL of 10% IV fluorescein diluted in 10 cc patient's own CSF, infused slowly over 30 minutes intrathecally
- Nasal endoscopy under blue light identifies the exact site of leak intraoperatively
- Not FDA-approved - patient consent required; complications are dose-related (seizures at high doses)
(e) Radionuclide Cisternography (RISA / In-111 DTPA):
- Intranasal pledgets assayed for radionuclide tracer
- Poor spatial resolution; high false-positive rate
- Rarely used as the sole test
(f) Nasal Endoscopy:
- Direct visualization of the leak site
- More valuable with intrathecal fluorescein enhancement
Additional investigations for middle-aged female:
- Formal ophthalmology - assess for papilledema (marker of ICP)
- MRI brain - empty sella, Meckel's cave, meningoencephalocele
- Lumbar puncture (after repair) - opening pressure to confirm/quantify ICP elevation
- Endocrine evaluation - if empty sella found (pituitary function)
Management
Management strategy depends on etiology, duration, and whether the leak is active. The overall approach is illustrated below:
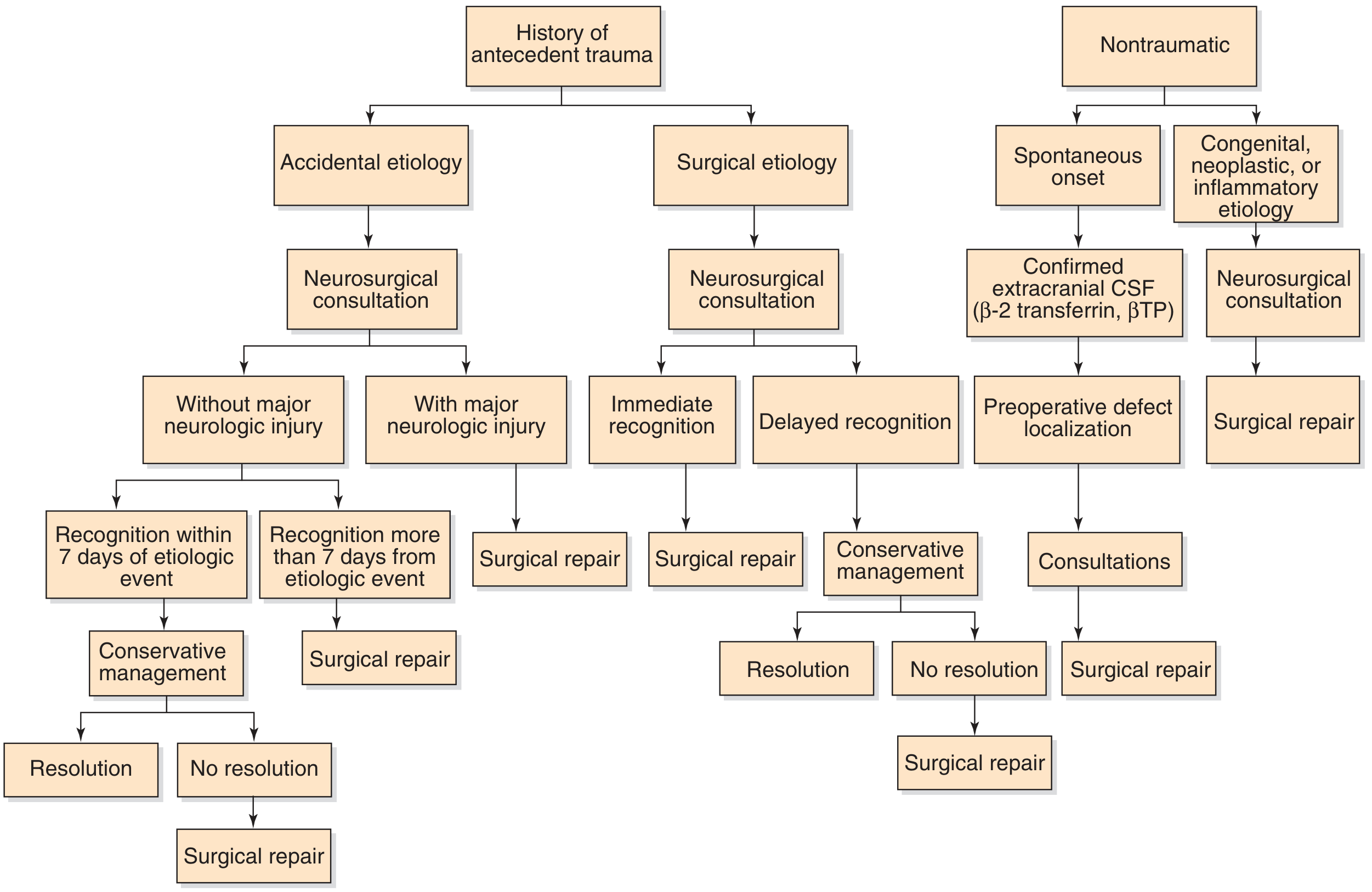
Fig. 2: Management strategy for CSF rhinorrhea repair. For the spontaneous onset (nontraumatic) pathway: confirm CSF (β-2 transferrin/βTP) → preoperative defect localization → consultations → surgical repair. (Cummings Otolaryngology, Fig. 48.10)
A. Conservative Management
Applicable for acute leaks (<7 days) or as a temporizing measure before definitive surgery.
Components:
BOX: Conservative Treatment of CSF Rhinorrhea
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
1. Strict bed rest with head elevation (30-45°)
2. Subarachnoid drainage via lumbar catheter
- Rate: 10 mL/hour (bag at shoulder level)
- CSF monitoring: cell count, protein, glucose, culture daily
3. Stool softeners (avoid Valsalva)
4. Avoid: coughing, sneezing, nose blowing, straining
5. Prophylactic antibiotics (controversial - more data for traumatic leaks)
6. Immunization: S. pneumoniae, H. influenzae, Meningococcus
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Lumbar Drain Management:
- Rate: 10 cc/hour is desirable
- Complications: meningitis, low ICP headache, pneumocephalus (air drawn through defect if ICP too low), subdural hematoma from over-drainage
- Contraindication: markedly elevated ICP (risk of cerebral herniation)
- Duration: 5-7 days
Limitations in spontaneous leaks: Unlike traumatic leaks (which resolve spontaneously in 70-85% within 1 week), spontaneous CSF leaks rarely resolve with conservative management alone because the underlying skull base defect and elevated ICP persist. Surgical repair is usually required.
B. Surgical Management
Indications for Surgery:
- Spontaneous CSF rhinorrhea (primary indication for surgical repair)
- Failed conservative management (leak persists >7-10 days)
- Recurrent CSF leak
- Large defect, meningoencephalocele
- Previous meningitis
- High-flow leak
Approaches available:
1. Endoscopic Endonasal Repair (Preferred - Gold Standard)
Since the 1980s, endoscopic endonasal repair has become the primary technique for surgical management of skull base CSF fistulae.
Steps of Endoscopic Repair:
STEP 1: Preoperative
├── Review HR-CT + MRI to identify defect location
├── Intrathecal fluorescein injection (intraoperatively, optional)
└── Patient consent for fluorescein (off-label use)
STEP 2: Endoscopic Dissection
├── Standard anterior and posterior ethmoidectomy as needed
├── Visualize the defect site (enhanced by fluorescein under blue light)
└── Identify any associated meningoencephalocele
STEP 3: Defect Preparation
├── Remove mucosa within 5 mm of defect margins (denuded bone needed for graft adherence)
├── Bipolar cautery / Coblation for meningoencephalocele reduction
│ (NEVER push a meningoencephalocele intracranially - fulgurate it)
└── Ensure flat surface for graft placement
STEP 4: Graft Selection and Placement
├── Autogenous grafts (preferred): fascia lata, temporalis fascia, fat, cartilage, septal bone
├── Allografts: acellular dermal allograft (ADM)
├── Xenografts: collagen dural substitutes (Durepair, Dura-Gen), porcine subintestinal submucosa
├── Pedicled: middle turbinate mucosal flap (higher failure rate)
└── Technique: UNDERLAY (intracranial side, held by ICP) preferred for small defects
BATH-PLUG (Wormald technique): fat plug intracranially, ICP holds it
STEP 5: Securing the Repair
├── Overlay graft of nasal mucosal free graft
├── Layers of absorbable collagen packing (e.g., Gelfoam, Surgicel)
├── Final non-absorbable nasal pack to hold everything in place
└── Lumbar drain (optional, individualized - high-flow or tenuous repairs)
Graft technique diagram:
Subarachnoid space (ICP pushes graft in)
↑
┌─────────────────────────────────────────────────────┐
│ ← Dura mater │
│ ← Underlay graft (fascia/ADM - on intracranial side) │
│ ← Skull base bone (defect) │
│ ← Overlay graft (nasal mucosal graft) │
│ ← Absorbable packing │
│ ← Nasal cavity │
└─────────────────────────────────────────────────────┘
Bath-plug technique:
Intracranial fat plug → fills defect → held by ICP from above
Results of Endoscopic Repair:
- Primary repair success rate: ~90%
- Secondary repair (revision) success rate: ~97%
- (From a large systematic review - Cummings)
Postoperative Care:
- Bed rest for several days
- Anti-staphylococcal antibiotics (prophylaxis for nasal packing)
- ICU/step-down monitoring for 24 hours (intracranial complications)
- Nasal packing removed at 3-5 days
- Avoid strenuous activity, sneezing, coughing for 6 weeks
- Serial nasal endoscopy in outpatient clinic to monitor healing
- Lumbar drain continued 1-5 days postoperatively if placed
2. Extracranial Non-Endoscopic Approaches (Historical)
External transsinus approaches (via external ethmoidectomy or transnasal without endoscope) - now largely replaced by endoscopic techniques. Mentioned for completeness and exam purposes.
3. Intracranial (Transcranial) Repair
- Via frontal craniotomy, done by neurosurgery
- Indicated for:
- Very large defects (especially posterior frontal sinus table, far lateral defects)
- Failed endoscopic repair
- Complex skull base pathology requiring simultaneous cranial base reconstruction
- Defects requiring osteoplastic flap or trephination (posterior frontal table)
- Repair using temporalis fascia, pericranium, or fat placed extradurally
- Higher morbidity than endoscopic approach
C. Management of the Underlying IIH/BIH (CRITICAL in Middle-Aged Female)
This step is uniquely important in the middle-aged obese female and is a high-yield exam point:
If surgical repair is done without addressing ICP → HIGH RECURRENCE RATE
LONG-TERM ICP MANAGEMENT (Post-repair)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
1. Weight reduction (primary modifiable risk factor)
2. Pharmacological:
- Acetazolamide (carbonic anhydrase inhibitor)
- Reduces CSF production
- Dose: 500 mg - 2 g/day in divided doses
- First-line medical therapy for IIH
- Furosemide (second-line diuretic, used with acetazolamide)
- Topiramate (weight loss benefit + mild carbonic anhydrase inhibition)
3. CSF Diversion Procedures (if medical therapy fails):
- Ventriculoperitoneal (VP) shunt
- Lumboperitoneal (LP) shunt
- Optic nerve sheath decompression (primarily for visual symptoms)
4. Repeat ophthalmology: monitor for papilledema resolution
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Key Exam Concept: In spontaneous CSF rhinorrhea in middle-aged women, the ICP paradox: the leak acts as a pressure-release valve. After repair, the true elevated ICP re-emerges. Failure to treat the elevated ICP leads to recurrence through the same or a new defect.
Complications of CSF Rhinorrhea
| Complication | Notes |
|---|---|
| Meningitis | Most feared - ascending infection via the fistula (pneumococcal most common) |
| Pneumocephalus | Air entering subarachnoid space |
| Brain abscess | Rare |
| Intracranial hypotension | From over-drainage |
| Recurrent leak | Especially if underlying ICP not treated |
Meningitis prevention:
- Vaccinate against Streptococcus pneumoniae, Haemophilus influenzae, Neisseria meningitidis
- Prophylactic antibiotics: controversial - best data support use for traumatic leaks, not conclusively proven for spontaneous
Summary Flow Diagram: Management of Spontaneous CSF Rhinorrhea in Middle-Aged Female
MIDDLE-AGED FEMALE with watery nasal discharge
↓
Confirm CSF: β-2 Transferrin (Gold Standard)
↓
Localize Defect:
HR-CT PNS + MRI Brain
± CT or MR Cisternography
± Intrathecal fluorescein (intraoperative)
↓
Multidisciplinary Assessment:
ENT + Neurosurgery + Ophthalmology + Endocrinology
↓
Is IIH present? (Obese? Empty sella? Papilledema?)
↓
YES ─────────────────── NO (true idiopathic)
↓ ↓
Treat IIH: Conservative trial
Acetazolamide (bed rest, lumbar drain
Weight loss 5-7 days)
↓ ↓
SURGICAL REPAIR (Primary): Resolved? → Observe
Endoscopic Endonasal Repair Not resolved? → Surgery
(Underlay/Bath-plug technique)
↓
Postoperative ICP management
(Acetazolamide ± VP/LP shunt if needed)
↓
Monitor with serial nasal endoscopy
Key Points for Exam
- Spontaneous CSF rhinorrhea in middle-aged obese women is strongly linked to IIH - treat the underlying ICP or risk recurrence.
- β-2 Transferrin is the gold-standard confirmatory test.
- Endoscopic endonasal repair is the current gold standard surgical approach (90% primary success, 97% revision success).
- Underlay technique is preferred for graft placement - ICP holds the graft in place.
- Fluorescein helps identify the exact leak site intraoperatively but is off-label.
- Empty sella on MRI = marker of elevated ICP.
- Meningitis prophylaxis: vaccinate, antibiotics are controversial.
- Unlike traumatic leaks, spontaneous leaks rarely resolve with conservative management alone.
- Long-term: acetazolamide reduces CSF production; VP/LP shunt for refractory IIH.
- The CSF acts as a pressure-release valve - after repair, ICP must be monitored and treated.
References: Cummings Otolaryngology Head and Neck Surgery (6th ed.), Chapter 48 - CSF Rhinorrhea; Shambaugh Surgery of the Ear; K.J. Lee's Essential Otolaryngology.
This is a shared conversation. Sign in to Orris to start your own chat.