What is the definition of rapidly progressive renal failure as per KDIGO guidelines
Reading File
Finding Sources
Searching the Web
KDIGO definition rapidly progressive renal failure glomerulonephritis
Finding Sources
Reading Web Page
rapidly progressive renal failure definition KDIGO
I now have solid, direct information from the KDIGO 2021 Glomerular Diseases Guideline and supporting textbooks. Here is the complete answer:
KDIGO Definition of Rapidly Progressive Renal Failure
The KDIGO (Kidney Disease: Improving Global Outcomes) 2021 Clinical Practice Guideline for Glomerular Diseases provides the most specific quantitative definition:
Rapidly progressive renal failure (in the context of RPGN) is defined as a ≥50% decline in eGFR over ≤3 months, after excluding other causes of RPGN (e.g., ANCA-associated vasculitis, anti-GBM disease) and reversible causes (e.g., drug toxicity, common pre- and post-renal causes).
This definition appears explicitly under Practice Point 2.4.3 (IgAN with RPGN) in the KDIGO 2021 Glomerular Diseases Guideline, and the same quantitative threshold is applied consistently across other glomerular disease contexts in the guideline.
Key Components of the KDIGO Definition
| Parameter | Criterion |
|---|---|
| Magnitude of GFR decline | ≥50% reduction in eGFR |
| Time frame | ≤3 months |
| Exclusions required | Other RPGN causes (AAV, anti-GBM disease) and reversible causes (drug toxicity, pre-/post-renal factors) must be excluded |
| Biopsy correlation | Crescents in a high proportion of glomeruli (typically >50%), with mesangial/endocapillary hypercellularity and focal necrosis |
Important Caveats per KDIGO
- The presence of crescents on biopsy alone, without a corresponding decline in serum creatinine, does not constitute rapidly progressive renal failure. Both the clinical and pathological criteria must be present.
- Patients with biopsy-proven crescents but stable GFR require close follow-up for prompt detection of any GFR decline; a second biopsy may be considered if deterioration occurs.
Broader Context: General RPGN Definition
More broadly, RPGN (Rapidly Progressive Glomerulonephritis) is defined clinically as a rapid decrease in GFR of at least 50% over a period of days to 3 months, as also described in Medscape/Emedicine and Robbins Pathology, which characterizes it as "acute renal failure, features of the nephritic syndrome, and often severe oliguria" with crescent formation on biopsy.
In summary: Per KDIGO, rapidly progressive renal failure = ≥50% decline in eGFR within ≤3 months, with biopsy evidence of crescentic glomerulonephritis and after exclusion of other reversible or secondary causes.
What is the definition of RPRF
Based on the previous answer I just provided, RPRF stands for Rapidly Progressive Renal Failure - and the definition is exactly what was covered above.
To summarize directly:
Definition of RPRF (Rapidly Progressive Renal Failure)
Per KDIGO 2021 Glomerular Diseases Guideline:
A ≥50% decline in eGFR over ≤3 months, after excluding other causes of RPGN (ANCA-associated vasculitis, anti-GBM disease) and reversible causes (drug toxicity, pre- and post-renal factors).
Quick Reference
| Component | Definition |
|---|---|
| GFR decline | ≥50% reduction in eGFR |
| Time frame | ≤3 months |
| Histology | Crescents in >50% of glomeruli (crescentic GN) |
| Clinical | Nephritic syndrome features + severe oliguria |
| Exclusions | Reversible causes must be ruled out first |
RPRF is the clinical syndrome; crescentic glomerulonephritis is its pathological correlate. The two terms (RPRF and RPGN - Rapidly Progressive Glomerulonephritis) are often used interchangeably in clinical practice.
What are the main causes of RPGN/RPRF?
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a thorough, textbook-grounded answer:
Causes of RPGN / RPRF
RPGN is classified into three immunopathological types based on the mechanism of glomerular injury. This classification is essential because it directly guides treatment.
Classification Overview
| Type | Mechanism | IF Pattern | Key Diseases |
|---|---|---|---|
| Type I | Anti-GBM antibody | Linear IgG + C3 | Goodpasture disease/syndrome |
| Type II | Immune complex deposition | Granular IgG/IgA/C3 | SLE, IgAN, post-infectious GN, HSP/IgA vasculitis, MPGN |
| Type III | Pauci-immune (ANCA-associated) | Negative / no deposits | AAV: GPA, MPA, EGPA; idiopathic |
TYPE I - Anti-GBM Antibody-Mediated (10-20%)
Caused by circulating IgG antibodies directed against the NC1 domain of the α3 chain of type IV collagen in the GBM.
- Goodpasture disease (isolated renal) - anti-GBM nephritis without lung involvement
- Goodpasture syndrome - anti-GBM nephritis + pulmonary hemorrhage (hemoptysis)
- Two age peaks: young men (2nd-3rd decade) and older women (>60 years)
- Almost all patients progress to kidney failure if untreated
- Immunofluorescence: linear staining of IgG and C3 along the GBM
TYPE II - Immune Complex-Mediated (20-30%)
Granular immune complex deposition in the GBM and/or mesangium triggers complement activation and inflammation.
Primary (idiopathic):
- Immune complex GN of unknown cause
Secondary:
- IgA nephropathy (IgAN) - crescentic/rapidly progressive IgAN (KDIGO Practice Point 2.4.3)
- IgA vasculitis / Henoch-Schonlein purpura (HSP)
- Post-infectious GN - classically post-streptococcal (also staphylococcal, especially IgA-dominant infection-related GN in diabetics)
- Systemic Lupus Erythematosus (SLE) - class III/IV lupus nephritis
- Membranoproliferative GN (MPGN)
- Cryoglobulinemia
Immunofluorescence: granular ("lumpy-bumpy") pattern of IgG, IgA, IgM, and/or C3.
TYPE III - Pauci-Immune / ANCA-Associated (50-60% - most common type)
No detectable immune deposits on IF or EM. Most cases are ANCA-positive and represent small-vessel vasculitis.
- Granulomatosis with Polyangiitis (GPA) - formerly Wegener's - PR3-ANCA (c-ANCA)
- Microscopic Polyangiitis (MPA) - MPO-ANCA (p-ANCA)
- Eosinophilic Granulomatosis with Polyangiitis (EGPA) - formerly Churg-Strauss - MPO-ANCA
- Idiopathic pauci-immune crescentic GN - ANCA-negative cases (~20%)
Immunofluorescence: negative (pauci-immune = "few immune deposits").
Histological Hallmark (All Types)
The unifying pathological finding across all three types is crescent formation - proliferation of parietal epithelial cells and infiltrating monocytes/macrophages filling Bowman's space, compressing the glomerular tuft.
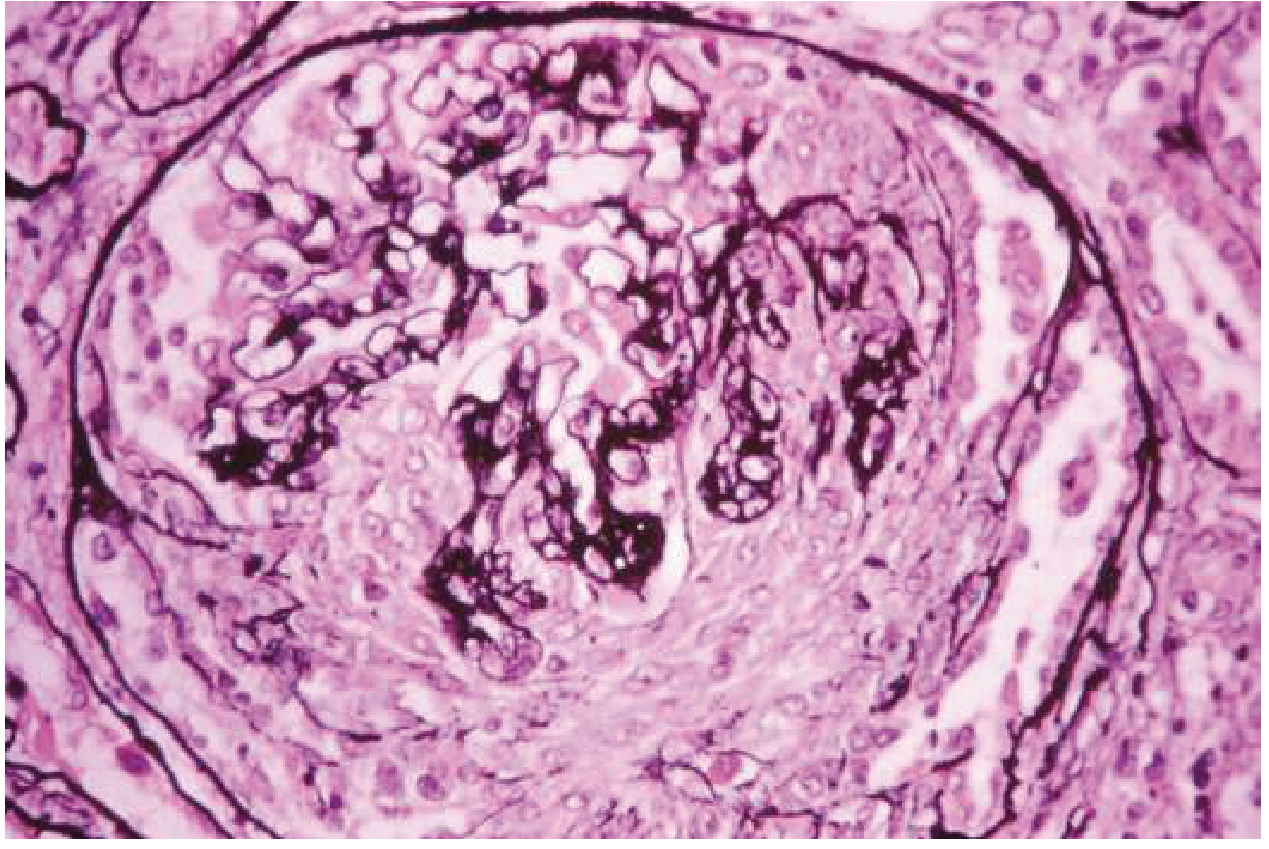
Crescentic glomerulonephritis: cellular proliferation filling Bowman's space and compressing the glomerular tuft.
- Crescents defined as affecting >50% of glomeruli in most classification schemes
- Segmental capillary necrosis and GBM ruptures are additional features
- Fibrin deposition in Bowman's space is characteristic
Key Clinical Point
Any cause of RPGN can also present with pulmonary-renal syndrome (simultaneous lung and kidney involvement), most notably:
- Anti-GBM disease (Goodpasture syndrome)
- ANCA-associated vasculitis (GPA, MPA)
Sources: Robbins & Kumar Basic Pathology; Goldman-Cecil Medicine International Edition; NKF Primer on Kidney Diseases 8e
This is a shared conversation. Sign in to Orris to start your own chat.