Right iliac fossa pain radioloy
Reading File
Finding Sources
Finding Sources
Searching PubMed
"right iliac fossa" AND radiology imaging
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive radiology content with images. Let me compile the full answer.
Radiology of Right Iliac Fossa (RIF) Pain
RIF pain is the commonest acute surgical presentation in the developed world. The main cause is acute appendicitis, but there is a long differential that imaging must help resolve. Plain AXR is largely unhelpful; the key modalities are ultrasound (US), CT, and MRI.
Differential Diagnosis at a Glance
Imaging must distinguish between these conditions:
| Surgical | Gynaecological | Other |
|---|---|---|
| Acute appendicitis | Acute salpingitis / PID | Mesenteric adenitis |
| Meckel's diverticulitis | Ovarian torsion | Terminal ileitis (Crohn's / Yersinia) |
| Caecal/right-sided diverticulitis | Ruptured follicular cyst | Ureteric colic |
| Intussusception | Ectopic pregnancy | Pyelonephritis |
| Malignancy | - | Rectus sheath haematoma |
| Omental infarction | - | Psoas abscess |
"Clinical diagnosis alone results in a normal appendix being found at appendicectomy in 10%-15%, and in young women the negative appendicectomy rate is higher still." - Grainger & Allison's Diagnostic Radiology
1. Plain Radiograph (AXR)
Plain abdominal X-rays are not indicated for suspected appendicitis. There are no specific plain film signs. However:
- Appendicolith - radio-opaque density projected over the RIF; high positive correlation with acute appendicitis when present
- Secondary ileus, matted small bowel loops, or proximal obstruction may be visible
- Erect CXR is useful if perforated peptic ulcer is suspected (gas under diaphragm in ~70%)
Fig. 18.24A - Supine AXR: radio-opaque appendicolith (white arrow) in the RIF of a 24-year-old presenting with acute abdominal pain:
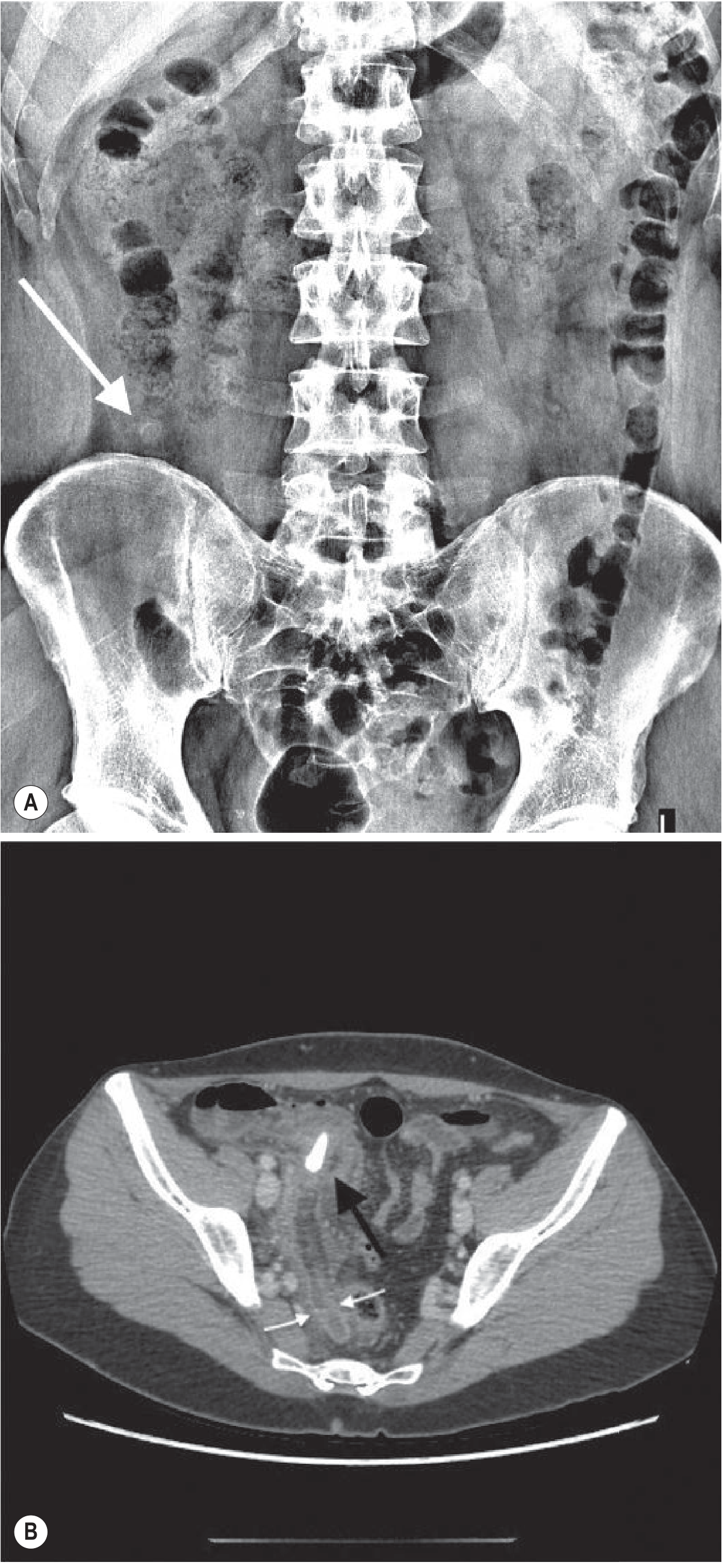
(A) AXR - radio-opaque appendicolith in RIF. (B) CT axial - appendicolith (black arrow) within the base of the inflamed oedematous appendix (white arrows)
2. Ultrasound (US)
Graded compression US is the preferred first-line test in:
- Children (favourable body habitus, radiation avoidance)
- Young women (higher incidence of tubal / ovarian pathology)
- Pregnant patients
Technique: The probe is applied with gradually increasing pressure over the RIF to displace bowel loops and expose the appendix.
US Signs of Acute Appendicitis (Table 18.6)
| Feature | Finding |
|---|---|
| Structure | Blind-ending, non-compressible tubular structure |
| Diameter | ≥7 mm |
| Peristalsis | Absent |
| Appendicolith | Hyperechoic focus with posterior acoustic shadow |
| Surrounding fat | Hyperechoic (periappendiceal inflammation) |
| Fluid | Peri-appendiceal fluid or abscess |
| Caecum | Oedema at caecal pole |
| Tenderness | Maximal tenderness directly over the appendix |
Sensitivity: 78%-98% / Specificity: 85%-98%
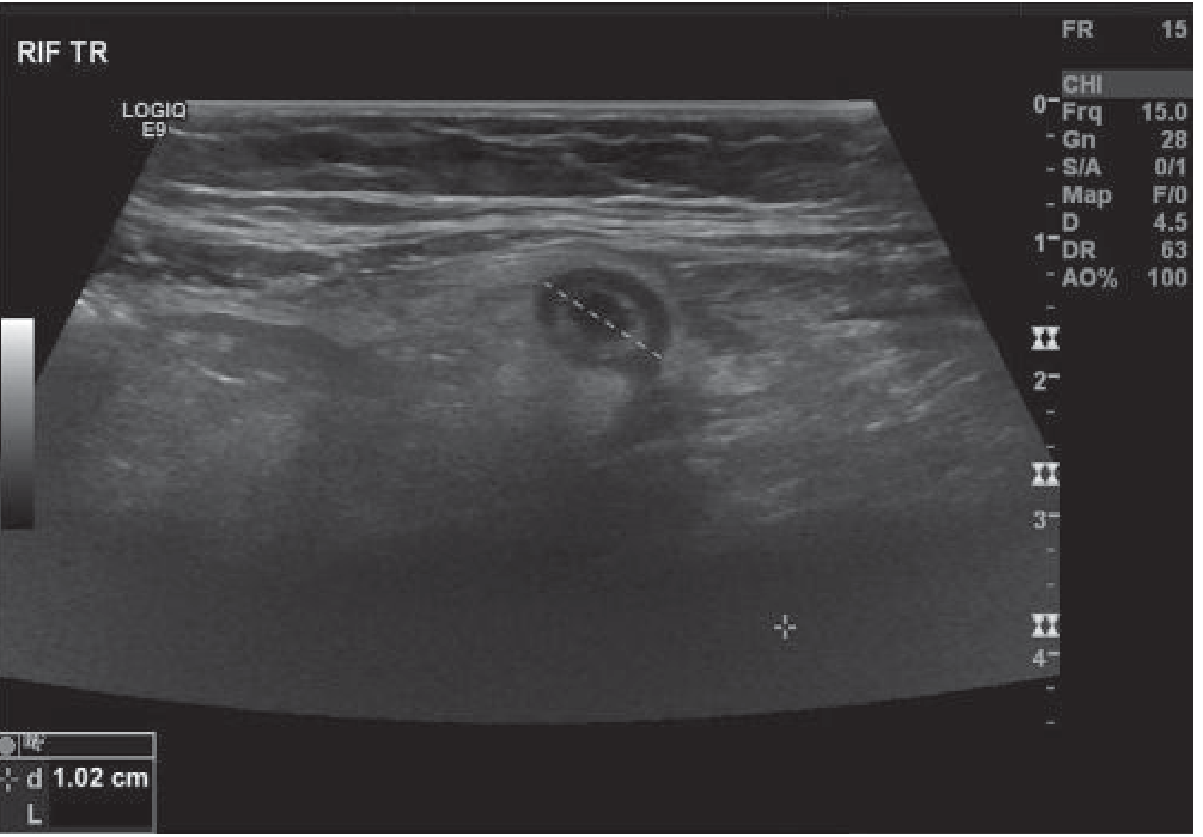
Fig. 18.25 - RIF transverse US: thickened hypoechoic tubular blind-ended structure measuring 1.02 cm (>7 mm), surrounded by hyperechoic fat:
US Pitfalls
False negatives:
- Focal tip appendicitis
- Retrocaecal appendicitis
- Gangrenous or perforated appendicitis (may become compressible - reported in 38% paediatric perforations, 55% adult perforations)
- Gas-filled appendix
- Very enlarged appendix
False positives:
- Dilated fallopian tube
- Peri-appendicitis
- Inflammatory bowel disease
- Inspissated stool mimicking appendicolith
A negative US where the appendix is not visualised is of little clinical value - it does not exclude appendicitis.
3. Computed Tomography (CT)
CT is the most sensitive and specific investigation for RIF pain.
Performance: Sensitivity and specificity approaching 100%/95% in expert centres; overall accuracy 93%-98%.
CT Signs of Acute Appendicitis:
| Sign | Detail |
|---|---|
| Appendix diameter | >6 mm |
| Wall enhancement | After IV contrast |
| Appendicolith | Hyperdense focus within appendix |
| Fat stranding | Increased fat attenuation peri-appendiceal |
| Fluid | Peri-appendiceal |
| Phlegmon / abscess | Soft-tissue mass ± gas |
| Caecal thickening | Oedema at appendiceal origin = "caecal bar" |
| Extraluminal gas | Indicates perforation |
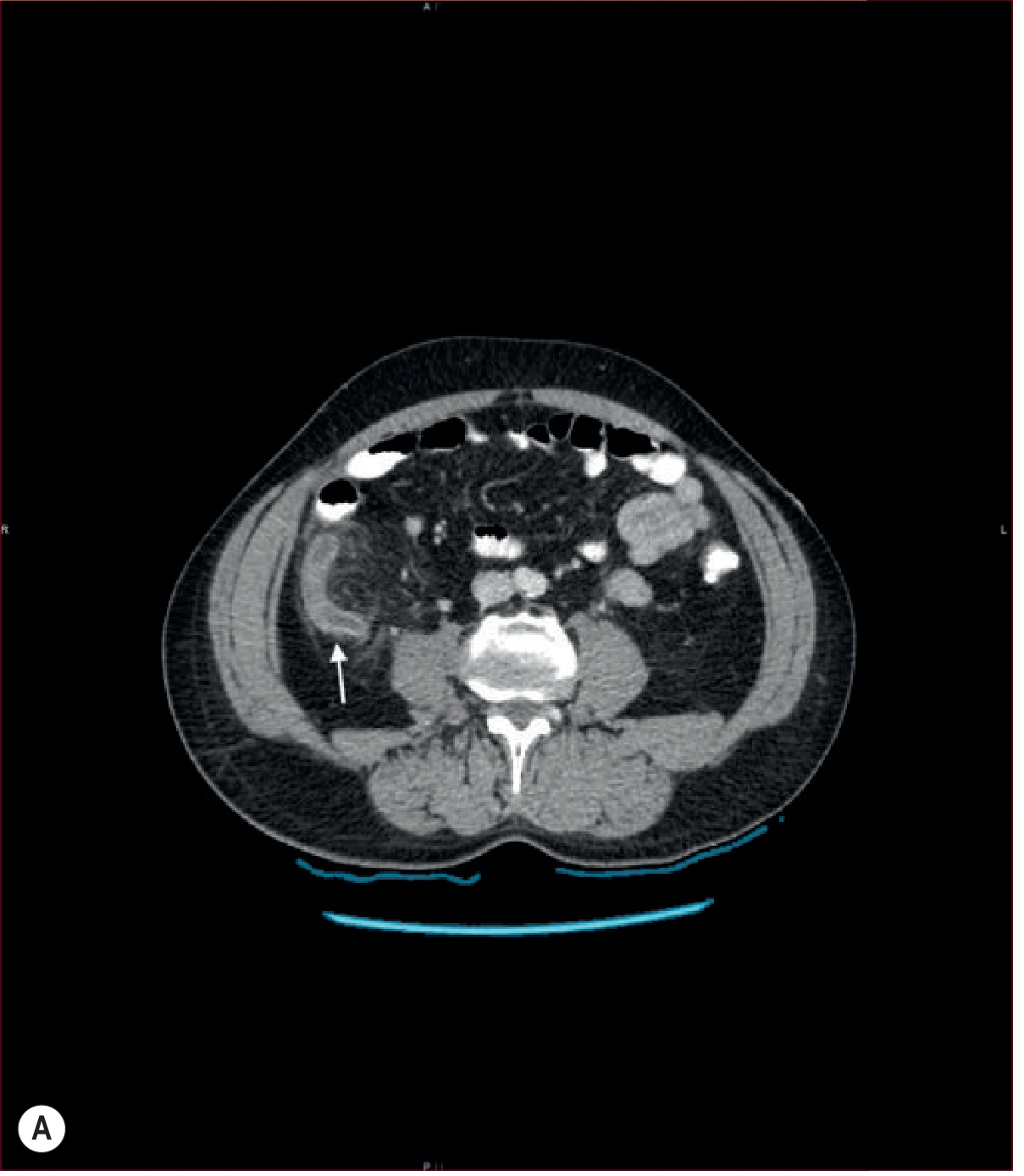
Axial CT - inflamed appendix (white arrow) with enhancing wall and surrounding peri-appendiceal fat inflammatory changes:
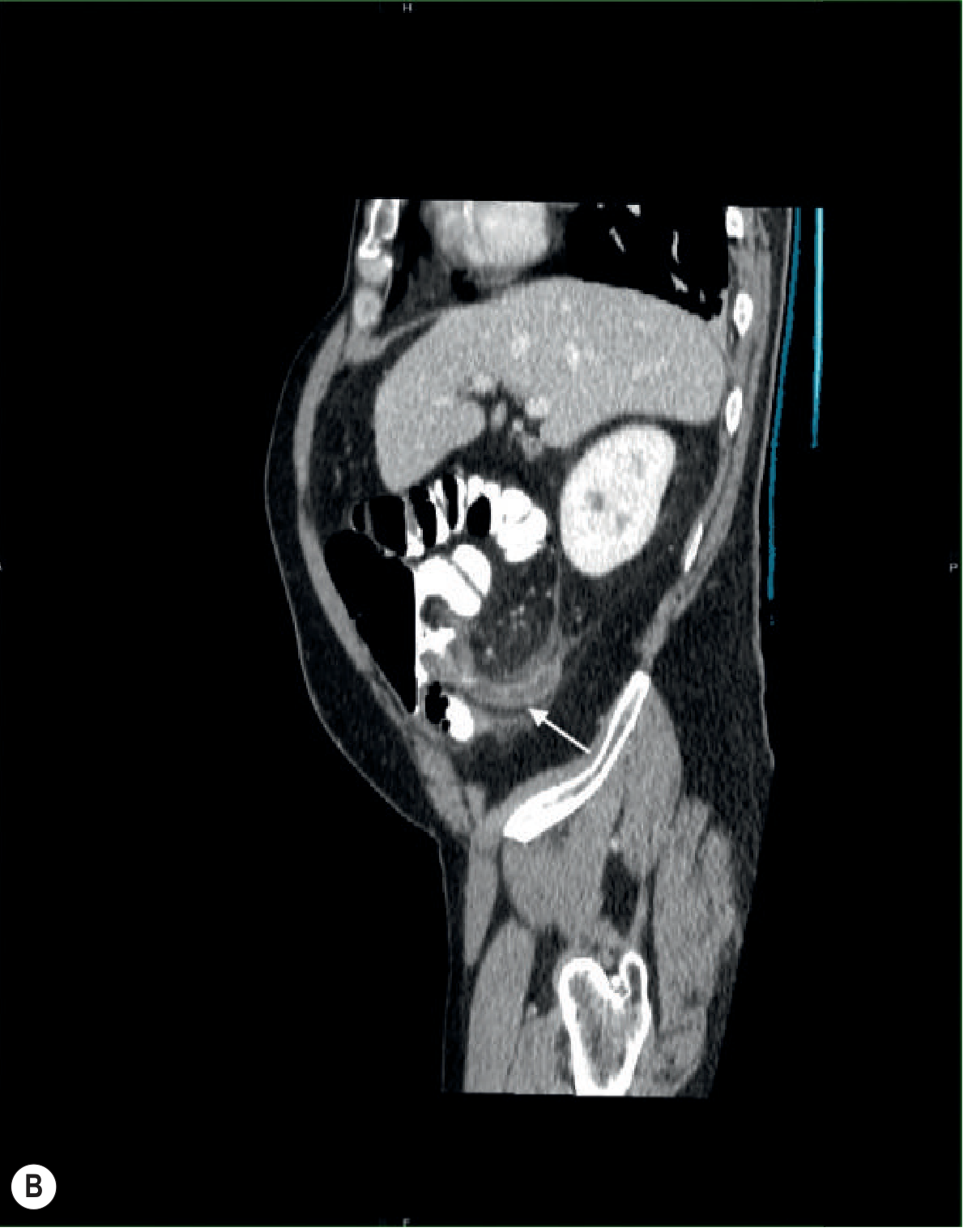
Sagittal CT - same patient showing the inflamed appendix:
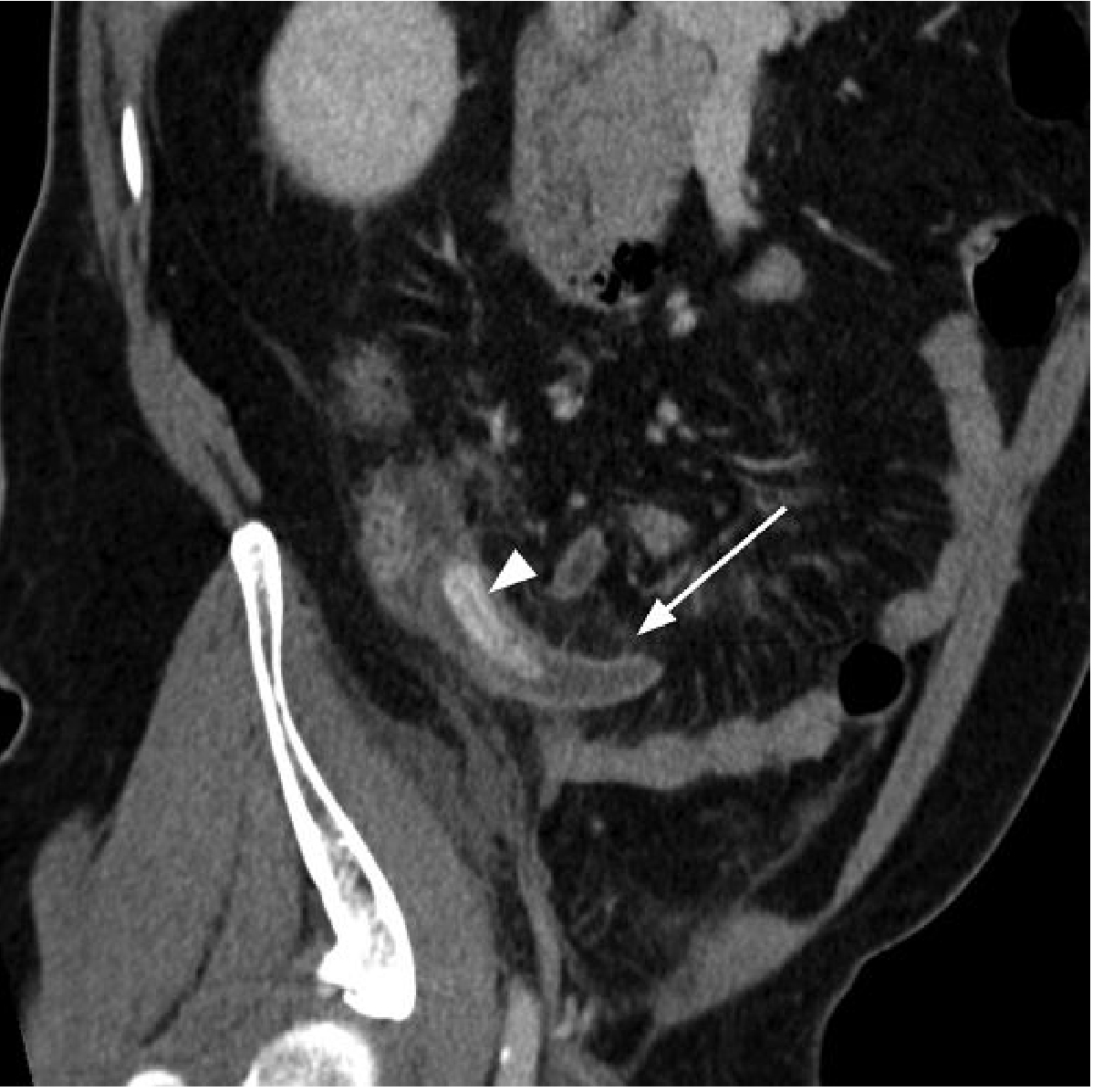
Coronal oblique CT - dilated blind-ending appendix with surrounding fat stranding (arrow) and appendicolith at the orifice (arrowhead):
CT Advantages
- Establishes an alternative diagnosis in up to 89% of non-appendicitis cases
- Key alternative diagnoses CT can identify: mesenteric adenitis, terminal ileitis, Meckel's diverticulitis, typhlitis, epiploic appendagitis, omental infarction
- Reduces negative appendicectomy rate from >20% to <9%
CT Disadvantages
- Radiation dose - particularly concerning in young patients and those with chronic disease requiring repeated imaging
- Performance depends heavily on radiologist experience
- Can cause treatment delay if not readily available
4. MRI
MRI is a radiation-free alternative showing substantial promise, particularly for:
- Pregnant patients (US first, MRI if equivocal)
- Paediatric presentations
- DWI (diffusion-weighted imaging) sequences enhance detection
The strategy of US first with CT only if equivocal has good positive and negative predictive value and significantly reduces radiation exposure in this typically young group.
Recommended Imaging Strategy
RIF Pain
↓
Children / Pregnant / Young Women
→ US first (graded compression)
→ If equivocal → MRI (preferred) or CT
Adult males / Equivocal clinical picture
→ US or CT (based on local expertise)
→ CT if US negative/non-diagnostic
Clinically obvious appendicitis
→ Imaging may not be needed before surgery
→ Image if: diagnostic doubt, atypical features, high suspicion of perforation/abscess
Selected Alternative Diagnoses and Their Radiology
| Condition | Key Imaging Finding |
|---|---|
| Ureteric colic | US/urogram: hydronephrosis, ureteric calculus; urinalysis: haematuria |
| Mesenteric adenitis | CT: enlarged mesenteric lymph nodes, normal appendix |
| Terminal ileitis (Crohn's) | CT/MRI: thickened terminal ileum, wall enhancement, skip lesions |
| Ovarian torsion | US: enlarged ovary, absent Doppler flow, free fluid |
| Ectopic pregnancy | US pelvis: adnexal mass, free fluid in pouch of Douglas; serum βhCG positive |
| Pyelonephritis | US: renal parenchymal oedema; CT: nephromegaly, striated nephrogram |
| PID / Salpingitis | US/MRI: thickened fallopian tube, free pelvic fluid, pyosalpinx |
| Epiploic appendagitis | CT: oval fat-density lesion with hyperechoic rim and central dot sign |
| Omental infarction | CT: fat-density mass with surrounding inflammation, no bowel involvement |
Sources:
- Grainger & Allison's Diagnostic Radiology, Chapter 18 (Imaging of the Acute Abdomen)
- Bailey and Love's Short Practice of Surgery 28th Edition, Chapter 76
- 22nd Edition Pye's Surgical Handicraft
This is a shared conversation. Sign in to Orris to start your own chat.