IBS management
Reading File
Finding Sources
Searching PubMed
"irritable bowel syndrome"[MeSH Terms] AND management
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the material needed for a comprehensive answer. Here is the full IBS management overview:
Irritable Bowel Syndrome (IBS) - Management
Diagnosis First: Rome IV Criteria
IBS is diagnosed clinically. Rome IV requires recurrent abdominal pain, on average at least 1 day/week in the last 3 months, associated with two or more of:
- Related to defecation
- Associated with a change in stool frequency
- Associated with a change in stool consistency
Subtypes are based on predominant stool form:
| Subtype | Description |
|---|---|
| IBS-C | Constipation-predominant (~25%) |
| IBS-D | Diarrhea-predominant (~35-40%) |
| IBS-M | Mixed bowel habits (~35-40%) |
| IBS-U | Unclassified (<5%) |
Alarm features (warrant colonoscopy and further workup): onset after age 40, rectal bleeding, significant weight loss, nocturnal diarrhea, steatorrhea, progressive course.
Minimum workup for typical IBS without alarm features: CBC, fecal calprotectin or lactoferrin, CRP. Check celiac serology in IBS-D if celiac prevalence >1%.
Step 1: General Measures (All Subtypes)
Patient Education & Reassurance
- Explain the gut-brain axis model; validate symptoms as real
- Reassure about the benign (non-progressive, non-malignant) nature
- Set realistic expectations - management aims to control symptoms, not cure
Dietary Modification
Low-FODMAP Diet (Fermentable Oligosaccharides, Disaccharides, Monosaccharides, and Polyols)
- Reduces IBS symptoms in 50-80% of patients
- A network meta-analysis of 13 RCTs found low-FODMAP diet superior to all other dietary interventions
- NNT = 5 (95% CI 3-11)
- Recommended by the ACG
Common high-FODMAP foods to avoid:
| Category | High-FODMAP Examples |
|---|---|
| Fruits | Apples, cherries, mangoes, pears, watermelon |
| Vegetables | Garlic, onion, artichokes, Brussels sprouts, fennel |
| Grains | Wheat, rye, barley |
| Dairy | Lactose-containing milk, soft cheeses |
| Legumes | Chickpeas, lentils, beans |
| Polyols | Cauliflower, mushrooms, stone fruits |
Other dietary advice:
- Eat slowly; avoid chewing gum and carbonated beverages (reduce gas/bloating)
- Consider lactose exclusion if dairy worsens symptoms
- Regular meals; avoid skipping meals
Lifestyle
- Regular aerobic exercise reduces global IBS symptoms
- Stress reduction strategies
Step 2: Pharmacotherapy (Subtype-Specific)
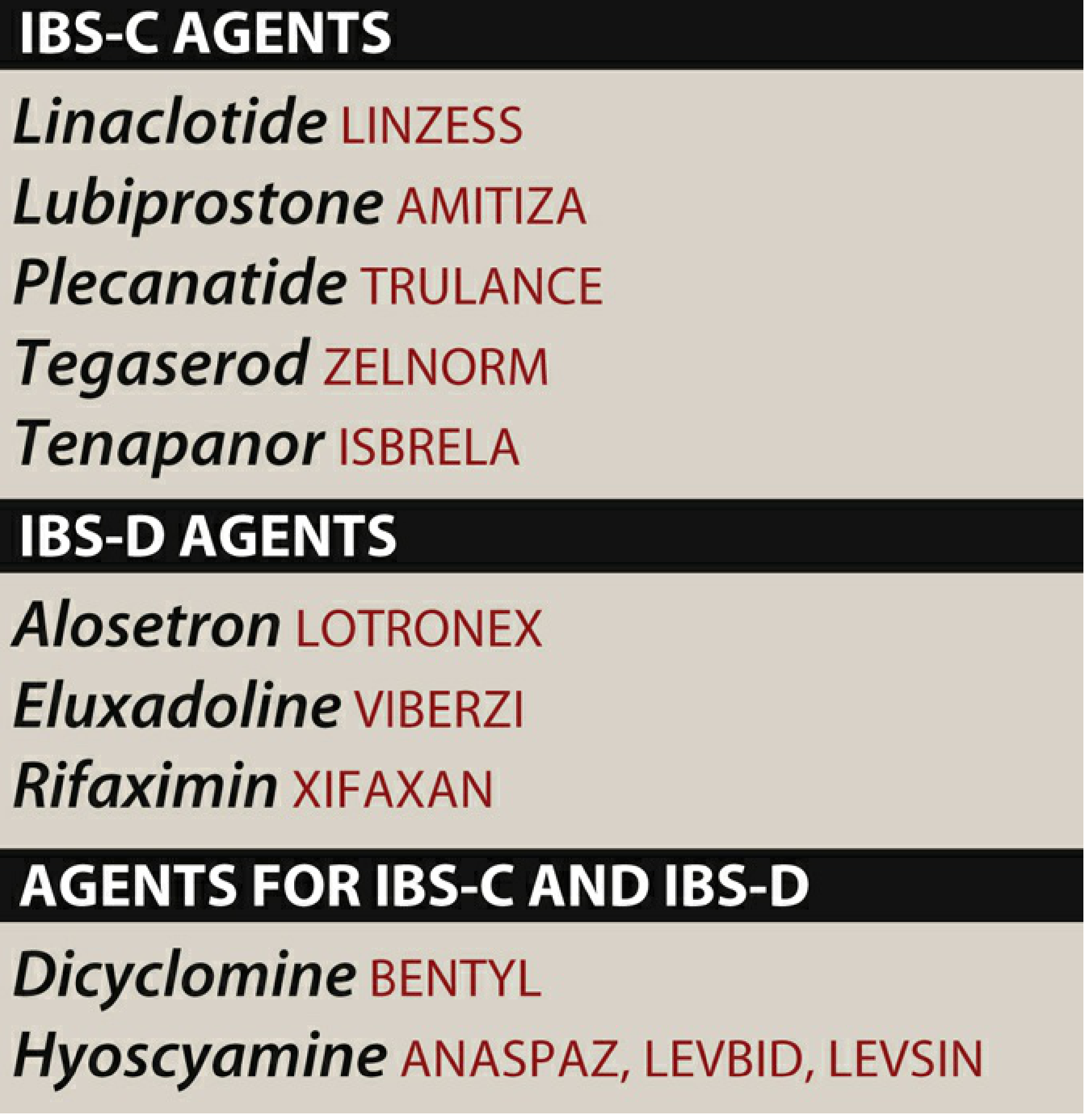
IBS-C (Constipation-Predominant)
| Drug | Mechanism | Notes |
|---|---|---|
| Linaclotide (Linzess) | Guanylate cyclase-C agonist | Increases intestinal fluid secretion + accelerates transit; also reduces visceral pain. First-line |
| Plecanatide (Trulance) | Guanylate cyclase-C agonist | Similar to linaclotide; pH-sensitive activation |
| Lubiprostone (Amitiza) | Chloride channel (ClC-2) activator | Approved in women with IBS-C; SE: nausea |
| Tenapanor (Isbrela) | NHE3 inhibitor | Reduces intestinal sodium absorption, increases luminal water |
| Tegaserod (Zelnorm) | 5-HT₄ partial agonist (prokinetic) | Restricted to women <65 without cardiovascular risk factors or ischemic CV disease history |
| Osmotic laxatives (PEG, lactulose) | Increase stool water content | Used empirically; less evidence specifically in IBS-C |
| Fiber supplements (psyllium) | Bulking agent | Psyllium preferred over insoluble fiber (wheat bran may worsen symptoms) |
IBS-D (Diarrhea-Predominant)
| Drug | Mechanism | Notes |
|---|---|---|
| Alosetron (Lotronex) | 5-HT₃ antagonist | Women only, severe IBS-D; risk of ischemic colitis and severe constipation - restricted prescribing program |
| Eluxadoline (Viberzi) | µ-opioid agonist / κ-opioid agonist / δ-opioid antagonist | Reduces motility and visceral pain; avoid in pancreatitis or alcoholism (risk of sphincter of Oddi spasm) |
| Rifaximin (Xifaxan) | Non-absorbable antibiotic; reduces bacterial load | Short-term use; can be retreated; NNT ~8 |
| Loperamide | Opioid receptor agonist (gut-selective) | Reduces stool frequency; does not help pain; OTC; useful for urgency |
| Ondansetron | 5-HT₃ antagonist | Off-label; improves stool consistency and urgency |
| Cholestyramine | Bile acid sequestrant | Useful if bile acid malabsorption contributing (~25% of IBS-D) |
Both IBS-C and IBS-D (Antispasmodics)
| Drug | Mechanism | Notes |
|---|---|---|
| Dicyclomine (Bentyl) | Antimuscarinic | Reduces GI spasms; SE: dry mouth, drowsiness, urinary retention |
| Hyoscyamine (Levsin) | Antimuscarinic | Same class; taken before meals for postprandial pain |
| Peppermint oil | Calcium channel blocker (smooth muscle relaxant) | Good evidence; NNT ~4; often taken as enteric-coated capsule |
Step 3: Neuromodulators / Antidepressants
Beneficial independent of their effect on mood - act on gut-brain axis, reduce visceral hypersensitivity.
- Tricyclic antidepressants (TCAs) - e.g., amitriptyline, imipramine, nortriptyline: effective across all IBS subtypes. Slow GI transit (beneficial in IBS-D). Lower doses than for depression (10-50 mg at night). Evidence is strongest.
- SSRIs - may be more useful in IBS-C (accelerate transit); evidence more mixed than TCAs
- SNRIs (duloxetine) are an emerging option
Step 4: Psychological / Brain-Gut Behavioral Therapies
A 2025 Lancet Gastroenterology network meta-analysis (PMID: 41077057) found behavioral therapies significantly superior to control for IBS symptom reduction.
- Cognitive Behavioral Therapy (CBT) - best evidence; improves both pain and quality of life
- Gut-directed hypnotherapy - consistently effective for pain
- Mindfulness-based therapies
- Psychodynamic therapy
These are recommended when symptoms are refractory, when psychological comorbidity exists, or when the patient prefers non-pharmacological approaches. A multidisciplinary approach (medical + psychological) is optimal.
Step 5: Modulation of the Gut Microbiota
- Probiotics: A 2024 network meta-analysis (PMID: 38999862) supports modest benefit; multi-strain preparations appear superior to single strains. Lactobacillus and Bifidobacterium combinations most studied.
- Prebiotics: Less evidence; can worsen bloating in some patients
- Synbiotics: Emerging data, generally favorable
- Fecal Microbiota Transplantation (FMT): Still investigational for IBS; results from RCTs have been inconsistent
Summary Algorithm
All IBS → Education + dietary modification (low-FODMAP) + lifestyle
↓
IBS-C: Fiber + osmotic laxatives → linaclotide/plecanatide → lubiprostone/tenapanor/tegaserod*
IBS-D: Loperamide (urgency) → rifaximin → eluxadoline or alosetron*
All: Antispasmodics (peppermint oil, dicyclomine) for pain
TCAs for pain across subtypes
CBT/gut-directed hypnotherapy for refractory cases
*restricted populations
Recent Evidence (2024-2025)
- Dietary interventions meta-analysis (Lancet GH 2025, PMID 40258374): Low-FODMAP diet ranked highest among dietary interventions in a network meta-analysis of IBS patients.
- Brain-gut behavioral therapies meta-analysis (Lancet GH 2025, PMID 41077057): CBT and gut-directed hypnotherapy showed the greatest effect on abdominal pain and global IBS symptoms.
- Probiotics/FMT meta-analysis (Nutrients 2024, PMID 38999862): Probiotics and synbiotics effective; FMT evidence remains inconsistent.
Sources: Harrison's Principles of Internal Medicine 22E (2025); Goldman-Cecil Medicine; Lippincott Illustrated Reviews: Pharmacology.
This is a shared conversation. Sign in to Orris to start your own chat.