Normal wave form of pulse
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Loading Image
Excellent! I now have everything needed for a thorough, well-illustrated answer.
Normal Waveform of the Arterial Pulse
Mechanism of Pulse Formation
Blood ejected into the aorta during systole generates a pressure wave that travels along the arterial wall at approximately 4 m/s in the aorta, 8 m/s in large arteries, and 16 m/s in small arteries. This wave expands the arterial wall as it passes, and that expansion is what we palpate as the pulse. The pressure wave velocity is far higher than actual blood flow velocity. As a result, the radial pulse at the wrist is felt about 0.1 seconds after the peak of systolic ejection into the aorta.
- Ganong's Review of Medical Physiology, 26th Ed., p. 542
The Normal Arterial Pressure Waveform
The diagram below (from Miller's Anesthesia) shows the normal waveform alongside the ECG. Each numbered component is labeled:
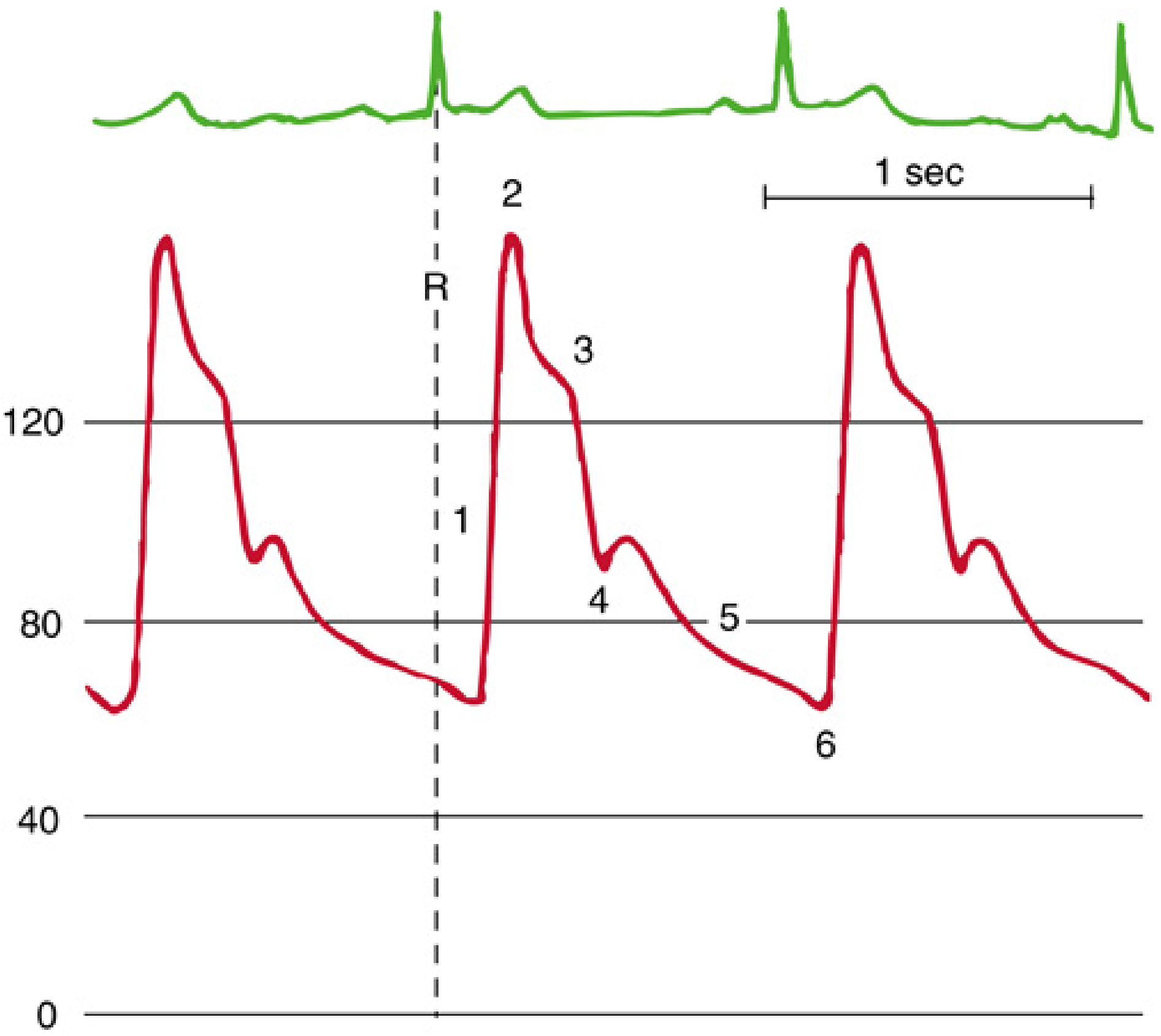
FIG. 32.25 - Miller's Anesthesia, 10e. Normal arterial blood pressure waveform and its relation to the ECG R wave.
Components of the Normal Pulse Waveform
| # | Component | Description |
|---|---|---|
| 1 | Systolic upstroke (Anacrotic limb) | Rapid rise in pressure as the left ventricle ejects blood into the aorta. The ascending limb is steep in normal individuals. |
| 2 | Systolic peak | The highest point of the waveform, corresponding to peak systolic pressure (~120 mmHg normally). |
| 3 | Systolic decline (Catacrotic limb) | Pressure falls as ejection slows and ventricular outflow decreases. |
| 4 | Dicrotic notch | A small notch/oscillation on the descending limb caused by vibrations when the aortic valve snaps shut (end of systole). It is visible on pressure recordings but not palpable at the wrist. |
| 5 | Diastolic runoff | Gradual decline in pressure as blood continues to flow into the peripheral circulation during diastole. |
| 6 | End-diastolic pressure | The lowest point of the waveform, corresponding to diastolic pressure (~70-80 mmHg normally). |
- Miller's Anesthesia, 10e, p. 4774
Key Features of the Normal Pulse on Palpation
A normal arterial pulse (shown leftmost in the chart below, compared with pathological patterns) has:
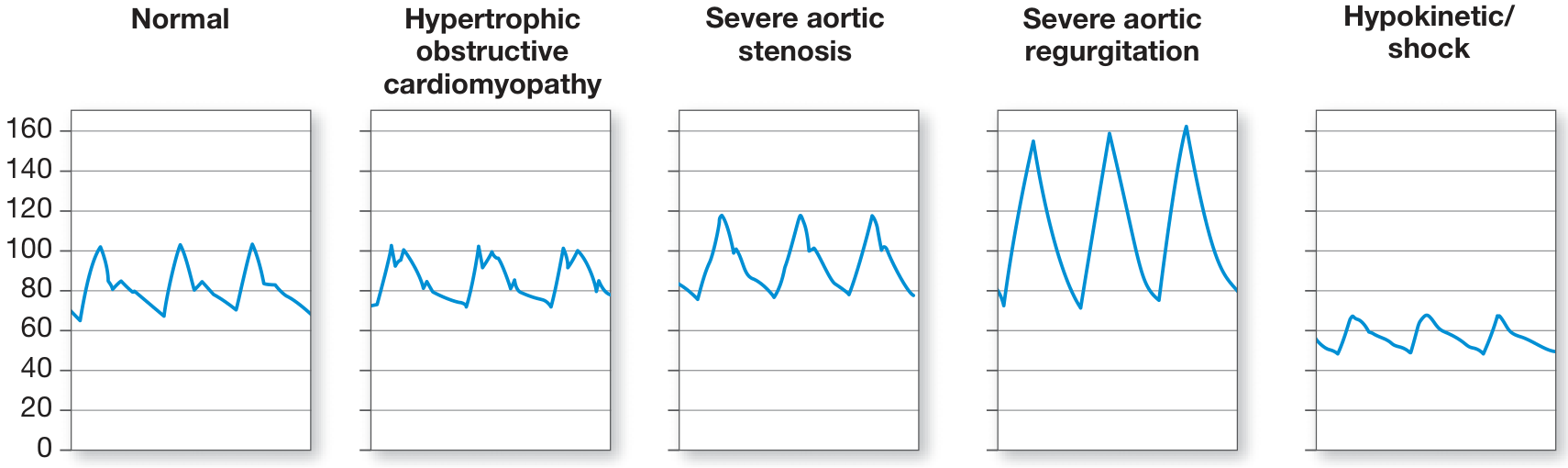
Fuster and Hurst's The Heart, 15th Ed. - Arterial pulse waveform patterns.
- Sharp systolic upstroke - brisk, rapid rise
- Narrow, rounded peak - single well-defined systolic peak (~100 mmHg)
- Prominent dicrotic notch on the downstroke
- Rapid downstroke back toward baseline
- Sabiston Textbook of Surgery, 20e
Pulse Pressure and Wave Strength
The strength of the pulse depends on the pulse pressure (systolic - diastolic), not mean arterial pressure:
- Weak/thready pulse: low stroke volume, as in shock
- Strong/bounding pulse: high stroke volume (exercise, aortic regurgitation, histamine administration)
- Corrigan/water-hammer pulse: seen in aortic regurgitation - very strong upstroke with rapid collapse
Distal Pulse Amplification
As the pressure wave travels from the aorta to peripheral arteries, the waveform changes:
- Wider pulse pressure
- Delayed systolic upstroke
- Slurred, delayed dicrotic notch
- More prominent diastolic wave
This is because retrograde reflected waves at the arteriolar level add to the antegrade wave, amplifying the peripheral waveform.
- Miller's Anesthesia, 10e, p. 4775
Summary
| Parameter | Normal Value |
|---|---|
| Systolic pressure | ~120 mmHg |
| Diastolic pressure | ~80 mmHg |
| Pulse pressure | ~40 mmHg |
| Pulse wave velocity (aorta) | ~4 m/s |
| Radial pulse delay from aorta | ~0.1 sec |
| Dicrotic notch | Present (visible on recording, not palpable) |
The normal pulse has a brisk upstroke, single systolic peak, and dicrotic notch - any deviation from this pattern points toward specific cardiac or vascular pathology.
This is a shared conversation. Sign in to Orris to start your own chat.