Treatment of scabies
Reading File
Finding Sources
Searching PubMed
scabies treatment
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Searching the Web
scabies treatment guidelines 2024 2025 permethrin ivermectin CDC WHO
I now have comprehensive data from Fitzpatrick's (the gold-standard dermatology text), Rosen's Emergency Medicine, Textbook of Family Medicine, Goldman-Cecil, plus web search results and recent PubMed systematic reviews. I have enough to write a thorough answer.
Treatment of Scabies
Scabies is caused by Sarcoptes scabiei var. hominis, an obligate human parasite mite that burrows into the stratum corneum. Treatment requires a scabicide, environmental decontamination, and simultaneous treatment of all contacts.
First-Line Treatment
1. Permethrin 5% Cream (Drug of Choice)
- Application: Apply from the neck down to the entire skin surface, paying close attention to finger/toe web spaces, the cleft of the buttocks, umbilicus, under fingernails and toenails, and around the genitals
- Infants and young children: Also treat the scalp and face
- Duration: Leave on for 8-14 hours (overnight), then wash off
- Repeat: A second application at 7-14 days is standard to kill any nymphs that hatched after the first treatment (eggs have some protection from scabicides)
- For crusted (Norwegian) scabies: Apply daily for 7 days, then twice weekly until cured
- Safety: Pregnancy Category B; approved by FDA for patients ≥2 months old
- Note: Permethrin resistance is increasingly reported in some regions
2. Oral Ivermectin
- Dose: 200 mcg/kg as a single oral dose, repeated at 14 days (second dose is essential - ivermectin has limited ovicidal activity)
- Indications: Crusted scabies, treatment failures, immunocompromised patients, mass treatment campaigns, patients who cannot adequately apply topical therapy
- For crusted scabies: Multiple doses recommended - days 1, 2, and 8 (some protocols extend further); combine with a topical agent
- Efficacy vs permethrin: A 2026 systematic review and meta-analysis (Innocent et al., BMC Infect Dis 2026, PMID 42098632) and a 2025 review (Abu-Zaid et al., Front Med 2025, PMID 41282002) confirm comparable efficacy between oral ivermectin and permethrin for classic scabies; cure rates with permethrin tend to be marginally higher in some trials
- Limitations: Not FDA-approved for scabies (off-label use); not recommended in children <15 kg or pregnant women; limited ovicidal activity
Treatment Drug Summary Table
| Drug | Dose/Application | Comments |
|---|---|---|
| Permethrin 5% cream | Neck down, 8-14 hrs, repeat at 7 days | First-line; Pregnancy Cat B; resistance emerging |
| Oral ivermectin | 200 mcg/kg x2 (day 1 and 14) | First-line alternative; off-label; not in pregnancy/<15 kg |
| Benzyl benzoate 10-25% | Apply x2-3 days, repeat at 7 days | Effective, cheap; widely used in developing countries |
| Crotamiton 10% cream | Apply days 1, 2, 3, and 8 | Antipruritic; marginal efficacy |
| Precipitated sulfur 5-10% | Apply 8 hrs on days 1, 2, 3 | Safe in neonates and pregnancy; limited data |
| Lindane 1% lotion | Apply 8 hrs, repeat at 7 days | Avoid - FDA black box warning for neurotoxicity; banned in California; contraindicated <10 years, pregnancy, seizure disorders |
| Malathion 0.5% lotion | Topical | Alternative in some European guidelines (Grade C) |
| Ivermectin 1% lotion | Topical | As effective as permethrin 5% cream in some studies |
Crusted (Norwegian) Scabies
This is a hyperinfestation variant with millions of mites, occurring in immunocompromised, elderly, or neurologically impaired patients. It is highly contagious and requires aggressive combined therapy:
- Oral ivermectin 200 mcg/kg on days 1, 2, 8 (and sometimes days 9, 15 for severe cases) PLUS
- Topical permethrin 5% applied daily for 7 days, then twice weekly until cured
- Strict isolation and thorough environmental decontamination are mandatory
- All healthcare workers and close contacts must be treated simultaneously
Environmental Decontamination (Fomite Control)
This is an integral part of treatment - failure here causes recurrence:
- Machine wash all clothing, bedding, and towels in hot water (>50°C/122°F)
- Items that cannot be washed (stuffed animals, etc.) can be:
- Dry cleaned
- Tumble dried on high heat for ≥15 minutes
- Sealed in plastic bags for at least 1 month (mites cannot survive >3-7 days off host)
- Vacuum furniture and carpets
Simultaneous Contact Treatment
All household members and close physical/sexual contacts must be treated at the same time, regardless of symptoms. Asymptomatic carriers are common (incubation period is 4-6 weeks for a new infestation), and failure to treat contacts universally causes rapid re-infestation.
Symptomatic Relief
Even after successful treatment, pruritus and rash can persist for up to 4 weeks (the so-called "postscabetic itch") due to the continued antigenic stimulation from dead mites and eggs:
- Antihistamines (oral): For pruritus relief
- Topical mid-potency corticosteroids: Help reduce inflammation and itch
- Do not mistake persistent posttreatment itch for treatment failure unless new burrows or new family member cases appear
Special Populations
| Population | Preferred Agent | Notes |
|---|---|---|
| Pregnant women | Permethrin 5% cream | Pregnancy Cat B; sulfur 5-10% is the safest alternative |
| Neonates (<2 months) | Sulfur 5-10% in petrolatum | Permethrin relatively contraindicated |
| Infants (2 months-2 yrs) | Permethrin 5% (include face/scalp) | Avoid lindane |
| HIV/immunocompromised | Ivermectin + permethrin combined | High risk of crusted scabies |
| Children <10 years | Permethrin 5% | Lindane absolutely contraindicated |
When to Suspect Treatment Failure vs. Postscabetic Itch
- Postscabetic itch: No new burrows, no new contacts developing symptoms, improves gradually over weeks
- True treatment failure or reinfestation: Appearance of new burrows, new household members developing itch, or symptoms worsening after 4 weeks
Sources: Fitzpatrick's Dermatology, 8e | Rosen's Emergency Medicine, 10e | Textbook of Family Medicine, 9e | Goldman-Cecil Medicine | IUSTI European Guideline for Scabies | CDC STI Treatment Guidelines 2021
Images of scabies rash
Finding Sources
Finding Sources
Finding Sources
Loading Image
Loading Image
Loading Image
Finding Sources
Loading Image
Loading Image
Loading Image
I have an excellent set of clinical and microscopic images from Fitzpatrick's Dermatology and Rosen's Emergency Medicine. Here is the full visual guide:
Scabies Rash - Image Gallery
All images sourced from Fitzpatrick's Dermatology (8e) and Rosen's Emergency Medicine (10e).
1. Crusted (Norwegian) Scabies - Face and Scalp Involvement

Fig. 178-1 - Crusted scabies showing hyperkeratotic plaques with diffuse scaling around the ear and hairline. This variant is populated with thousands to millions of mites. It occurs in immunocompromised, elderly, or neurologically impaired patients. Note the head and scalp involvement - a site typically spared in healthy adults but affected in crusted disease.
2. Classic Scabies Burrows - Interdigital Web Spaces and Knuckles

Fig. 178-2 - Several thread-like, serpentine burrows visible in the web spaces of the fingers and across the knuckles. This is one of the most common and characteristic locations for scabies. The burrow is the pathognomonic lesion - a 1-10 mm linear or J-shaped tunnel excavated by the female mite in the stratum corneum.
3. Scabies - Papules and Excoriations on Buttocks

Fig. 107.30 (Rosen's EM) - Scattered erythematous papules with excoriations over the buttocks and upper thighs, a classic distribution site. Pruritus is typically intense and worst at night.
4. Dermoscopy - The "Delta-Wing Jet" Sign

Fig. 178-4 - Dermoscopy of a scabies burrow showing the classic "delta-wing jet" sign:
- Dark brown structure (left): Dense mite head parts
- Translucent body extending to the right
- Red arrows: Scabies eggs along the burrow track
- Black arrow: Relatively translucent mite body
- S-shaped curving track: The burrow itself
Dermoscopy is a useful non-invasive technique to visualize the mite in vivo before scraping.
5. Microscopy - Gravid Female Mite, Eggs, and Fecal Pellets (Scybala)

Fig. 178-3 - Mineral oil preparation from a scraped burrow under low-power microscopy. Left: the gravid female mite (Sarcoptes scabiei). Right: oval gray eggs (the mite lays 0-4 eggs/day, up to 50 over her 30-day lifespan) and small dark fecal pellets (scybala). Confirming any of these elements on scraping gives a definitive diagnosis.
6. Skin Biopsy - Mite in the Stratum Corneum (Histology)
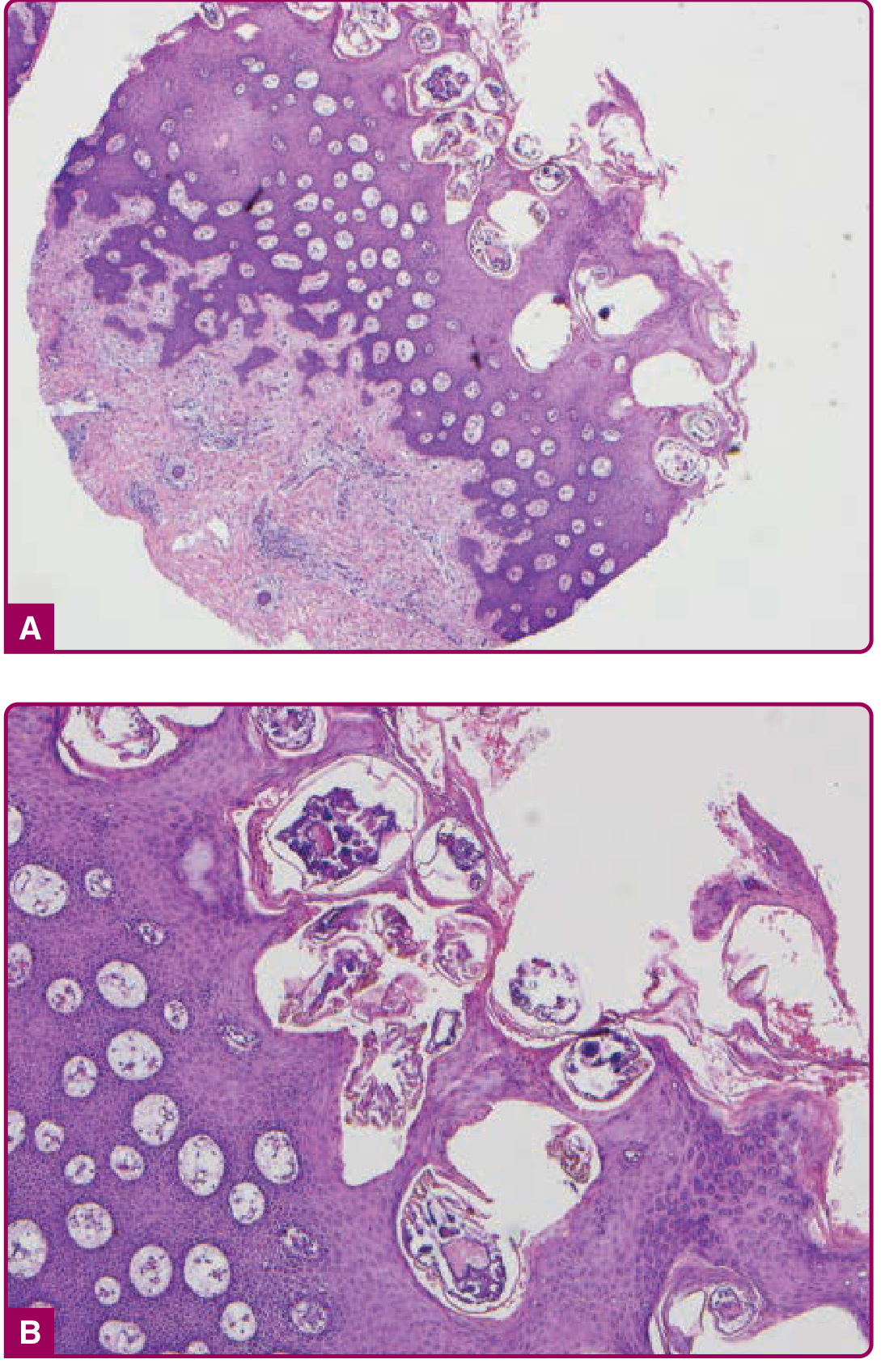
Fig. 178-5 - H&E skin biopsy sections at (A) ×4 and (B) ×10 magnification. The mite is seen transected within the stratum corneum - the diagnostic finding on histopathology. Note the massive burden of eggs and mite cross-sections in this crusted scabies case, explaining why hyperkeratotic lesions harbor millions of organisms.
Clinical Summary: Key Morphologies to Recognize
| Lesion | Significance |
|---|---|
| Burrow (linear/J-shaped, 1-10 mm) | Pathognomonic; best seen in web spaces, wrists |
| Papules/pustules (<5 mm) | Most common lesion; intense nocturnal itch |
| Excoriations | Due to scratching; can obscure primary lesions |
| Nodules (indurated, crusted) | Common in infants, intertriginous areas |
| Hyperkeratotic plaques | Crusted scabies; palms, soles, nails |
Source: Fitzpatrick's Dermatology 8e, Rosen's Emergency Medicine 10e
This is a shared conversation. Sign in to Orris to start your own chat.