brainstem physiology functions etc according to guyton book
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the core content. Let me compile the comprehensive answer from Guyton and Hall.
Brainstem Physiology — Guyton and Hall Textbook of Medical Physiology
Overview: What Is the Brain Stem?
The brain stem consists of the medulla, pons, and mesencephalon (midbrain). Guyton describes it in two complementary ways:
- As an extension of the spinal cord — it contains motor and sensory nuclei that serve the face and head regions just as the spinal cord serves the rest of the body.
- As its own master — it has unique, indispensable integrative functions that neither the cortex nor the spinal cord can substitute for.
Core Functions of the Brain Stem (Guyton's List)
| Function | Structure Primarily Involved |
|---|---|
| Control of respiration | Medullary respiratory centers |
| Control of the cardiovascular system | Medullary vasomotor centers |
| Partial control of gastrointestinal function | Dorsal motor nucleus of vagus |
| Control of stereotyped body movements | Reticular nuclei + vestibular nuclei |
| Control of equilibrium | Vestibular nuclei |
| Control of eye movements | CN III, IV, VI nuclei; MLF |
| Way station for command signals from higher centers | Reticular formation throughout |
1. Motor Control via the Brain Stem
Cortical and Brain Stem Control of Motor Function
Most voluntary movements initiated by the cerebral cortex are achieved by activating patterns of function stored in lower brain areas — the spinal cord, brain stem, basal ganglia, and cerebellum. These lower centers then send specific control signals to muscles.
A few movements (e.g., fine dexterous finger/hand movements) do have a near-direct cortical-to-motor neuron pathway, but most motor control flows through or via the brain stem.
2. Reticular and Vestibular Nuclei — Support Against Gravity
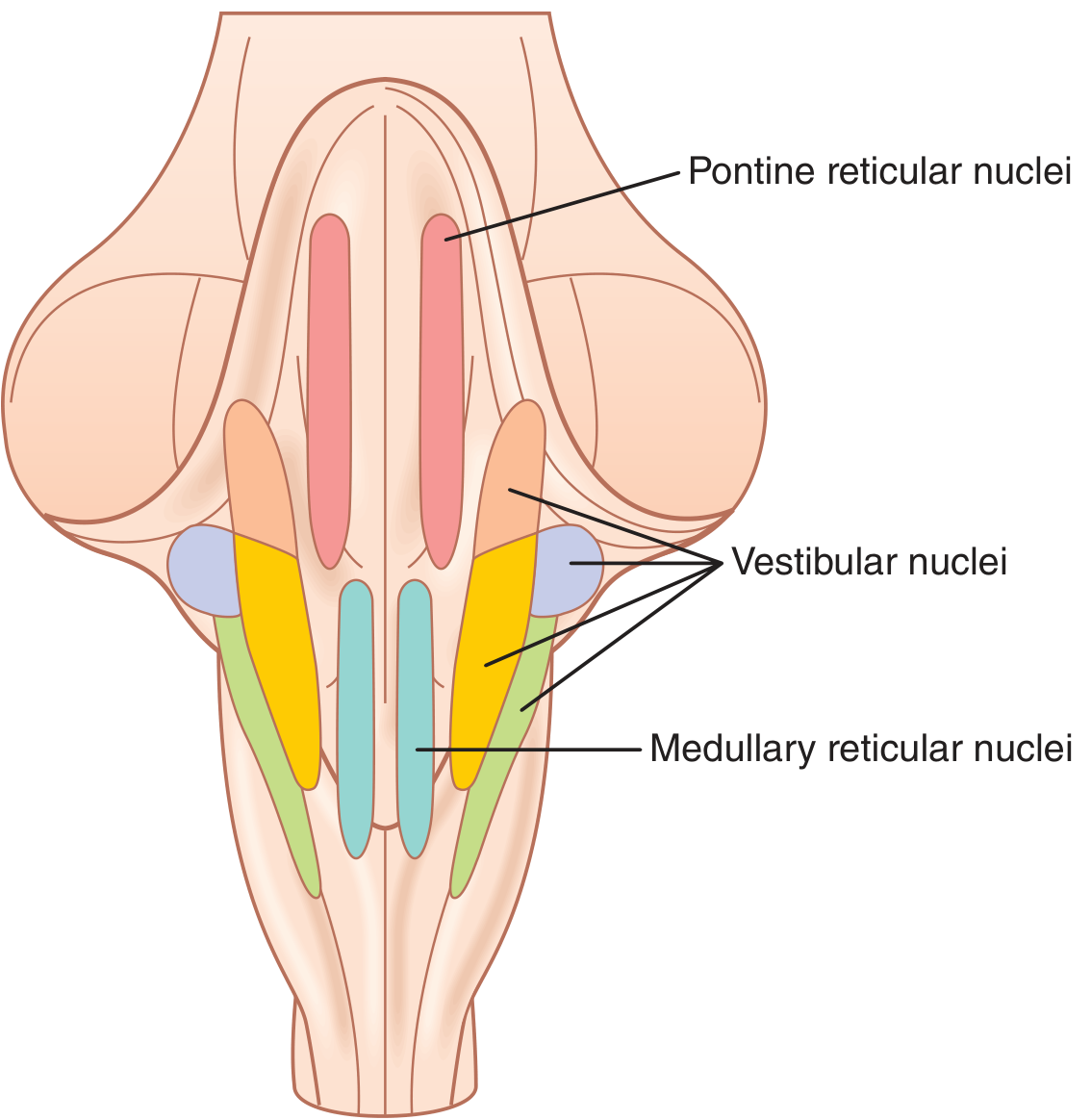
Figure 56.7 — Locations of the reticular and vestibular nuclei in the brain stem
Excitatory–Inhibitory Antagonism Between Pontine and Medullary Reticular Nuclei
Two major groups of reticular nuclei work antagonistically:
Pontine reticular nuclei (posterolateral pons + mesencephalon)
- Transmit excitatory signals downward via the pontine reticulospinal tract (anterior spinal cord column)
- Terminate on medial anterior motor neurons → excite axial/antigravity muscles (vertebral column extensors, limb extensors)
- Have a high natural excitability; receive strong input from vestibular nuclei and deep cerebellar nuclei
Medullary reticular nuclei (ventral, midline throughout medulla)
- Transmit inhibitory signals downward via the medullary reticulospinal tract (lateral cord column)
- These inhibitory signals can be overcome when the pontine system is strongly activated
- Receive inhibitory input from the basal ganglia and from cortical areas anterior to the motor cortex
Role of the Vestibular Nuclei
The vestibular nuclei cooperate with the pontine reticular system to excite antigravity muscles. They send signals via the lateral vestibulospinal tract to the same anterior motor neurons. The decerebrate animal (brain stem transected above the vestibular nuclei) shows intense antigravity rigidity because:
- The pontine and vestibular excitatory systems are released from cortical inhibitory override
- The medullary inhibitory area loses its corticospinal-driven input
3. Vestibular Apparatus and Equilibrium
The Vestibular Apparatus
Located in the inner ear, the vestibular apparatus contains:
- Utricle and saccule — detect static head orientation (gravity) and linear acceleration via maculae and otoliths (statoconia)
- Three semicircular ducts (anterior, posterior, lateral) — detect rotational acceleration via cristae ampullares and cupula
Hair cells are the sensory transducers. Bending stereocilia toward the kinocilium → depolarization (increases firing from ~100/sec baseline to several hundred/sec). Bending away → hyperpolarization.
Neuronal Connections of the Vestibular Apparatus
Signals pass via the vestibular nerve (CN VIII) → vestibular nuclei in the brain stem. From there, signals project:
- Downward via vestibulospinal tracts → anterior motor neurons of the spinal cord (equilibrium control)
- Upward via the medial longitudinal fasciculus (MLF) → CN III, IV, VI nuclei → corrective eye movements (vestibulo-ocular reflex)
- To the cerebellum (vestibulocerebellum / flocculonodular lobe)
- To the cerebral cortex (parietal lobe, deep in the sylvian fissure) → conscious awareness of body position
4. Reticular Formation and Brain Arousal (ARAS)
Reticular Excitatory Area — The "Driver" of Brain Activity
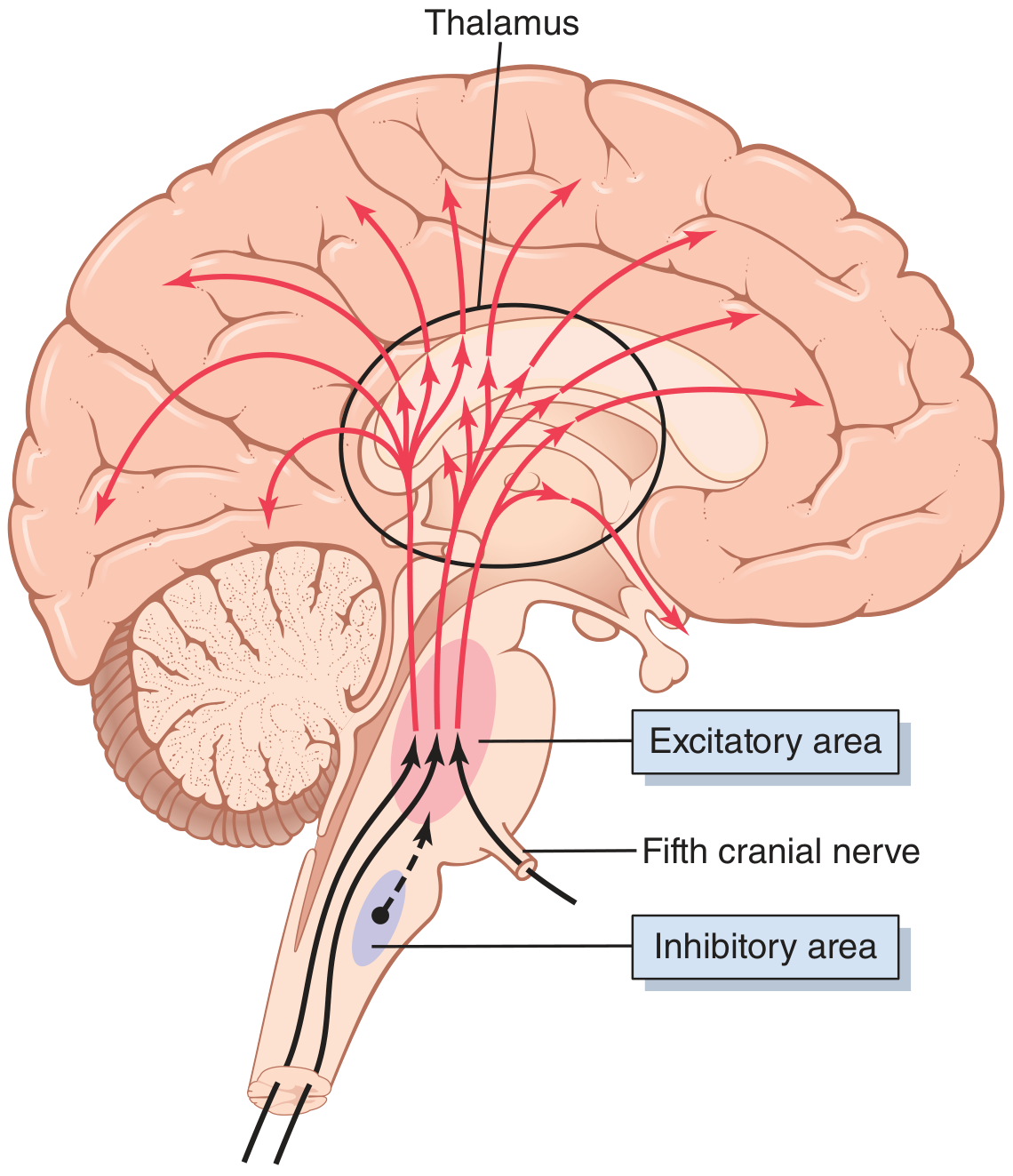
Figure 59.1 — The excitatory-activating system; excitatory area in pons/mesencephalon, inhibitory area in medulla
The bulboreticular facilitatory area (pons + mesencephalon) is the ARAS (Ascending Reticular Activating System). It drives wakefulness and alertness by:
- Sending signals upward → thalamus → all regions of cerebral cortex + subcortical areas
- Sending signals downward → spinal cord (antigravity tone, reflex amplification)
Two types of excitatory signals reach the thalamus:
- Rapid action potentials from large neurons — release acetylcholine (lasts milliseconds, destroyed by acetylcholinesterase)
- Slowly conducted signals from small neurons → intralaminar thalamic nuclei → gradually build cortical excitation over seconds to minutes (controls long-term background excitability)
What activates the excitatory area?
- Peripheral sensory signals — especially pain, which is the strongest activator
- Feedback from the cerebral cortex — once activated, the cortex sends back excitatory signals, creating a positive feedback loop that sustains wakefulness
- Cutting the brain stem above the entry of CN V (trigeminal) → loss of all major somatosensory input → rapid progression to coma
Reticular Inhibitory Area
Located medially and ventrally in the medulla, this area:
- Inhibits the reticular facilitatory area → decreases overall brain activity
- Acts partly by activating serotonergic neurons, which secrete serotonin at key brain sites (inhibitory neurohormone)
5. Neurohormonal Control of Brain Activity from the Brain Stem
The brain stem contains the cell bodies of four major neurohormonal/neurotransmitter systems that modulate global brain activity:
| System | Location | Transmitter | Effect |
|---|---|---|---|
| Norepinephrine | Locus ceruleus (pons-mesencephalon junction) | Norepinephrine | Generally excitatory; important in REM sleep/dreaming |
| Dopamine | Substantia nigra (anterior mesencephalon) | Dopamine | Excitatory in some areas, inhibitory in others; projects to caudate/putamen |
| Serotonin | Raphe nuclei (midline pons/medulla) | Serotonin | Generally inhibitory; projects to spinal cord (pain suppression) + widespread brain areas |
| Acetylcholine | Pons/mesencephalon reticular area | Acetylcholine | Excitatory; critical for wakefulness and REM sleep |
6. Stereotyped Movements — Brain Stem Integration
An anencephalic baby (no brain structures above the mesencephalon) can still perform:
- Suckling and food extrusion
- Hand-to-mouth movements
- Yawning and stretching
- Crying and visual tracking (eyes + head movements)
- Postural adjustments when pressure is applied to the legs
This demonstrates that many stereotyped motor functions are integrated at the brain stem level, independent of the cerebral cortex.
7. Dual Pain Pathways Through the Brain Stem
Two ascending pain pathways pass through the brain stem:
- Neospinothalamic tract — fast pain, sharp quality; travels with minimal synapses to the thalamus
- Paleospinothalamic tract — slow, burning/aching pain; synapses extensively in the reticular formation of the brain stem → this is why deep visceral/burning pain is so arousing and autonomically activating
Summary Table
| Brain Stem Region | Key Function |
|---|---|
| Medulla | Respiratory rhythmogenesis, cardiovascular (vasomotor) center, vomiting center, reticular inhibitory area, nuclei of CN IX–XII |
| Pons | Pneumotaxic and apneustic respiratory centers, pontine reticular excitatory system (antigravity), locus ceruleus, nuclei of CN V–VIII |
| Mesencephalon | Superior/inferior colliculi (visual/auditory reflexes), substantia nigra (dopamine), red nucleus, nuclei of CN III–IV, periaqueductal gray (pain modulation) |
| Throughout (Reticular Formation) | ARAS (arousal/wakefulness), neurohormonal modulation, coordination of autonomic reflexes |
Source: Guyton and Hall Textbook of Medical Physiology (Chapters 56 & 59), p. 692–698, 729–732
DCML and ALS Pathway physiology
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
All three key diagrams retrieved. I have all the content needed for a comprehensive answer.
DCML and ALS Pathways — Guyton and Hall Textbook of Medical Physiology
All sensory information from the somatic body enters the spinal cord through the dorsal roots of the spinal nerves, then ascends to the brain through one of two alternative pathways that partially reconverge at the thalamus.
Side-by-Side Comparison (Overview)
| Feature | DCML | ALS |
|---|---|---|
| Full name | Dorsal Column–Medial Lemniscal System | Anterolateral System |
| Fiber size | Large myelinated (Aβ) | Smaller myelinated (Aδ) + unmyelinated (C) |
| Conduction velocity | 30–110 m/sec | few m/sec to 40 m/sec |
| Where it crosses | Medulla (at dorsal column nuclei) | Spinal cord (at each entry level) |
| Spatial localization | High — up to 100 gradations | Poor — only 10–20 gradations |
| Temporal fidelity | High — rapidly changing signals | Low |
| Thalamic relay | Ventrobasal complex | Ventrobasal complex (tactile) + Intralaminar nuclei (pain) |
| Cortical destination | Postcentral gyrus (S-I) | Postcentral gyrus + reticular areas |
1. Dorsal Column–Medial Lemniscal System (DCML)
Sensations Carried
- Touch requiring precise localization
- Touch with fine gradations of intensity
- Vibratory sensations (phasic)
- Movement sensation against the skin
- Joint position sense (proprioception)
- Fine pressure judgment
Anatomy — 3-Neuron Arc
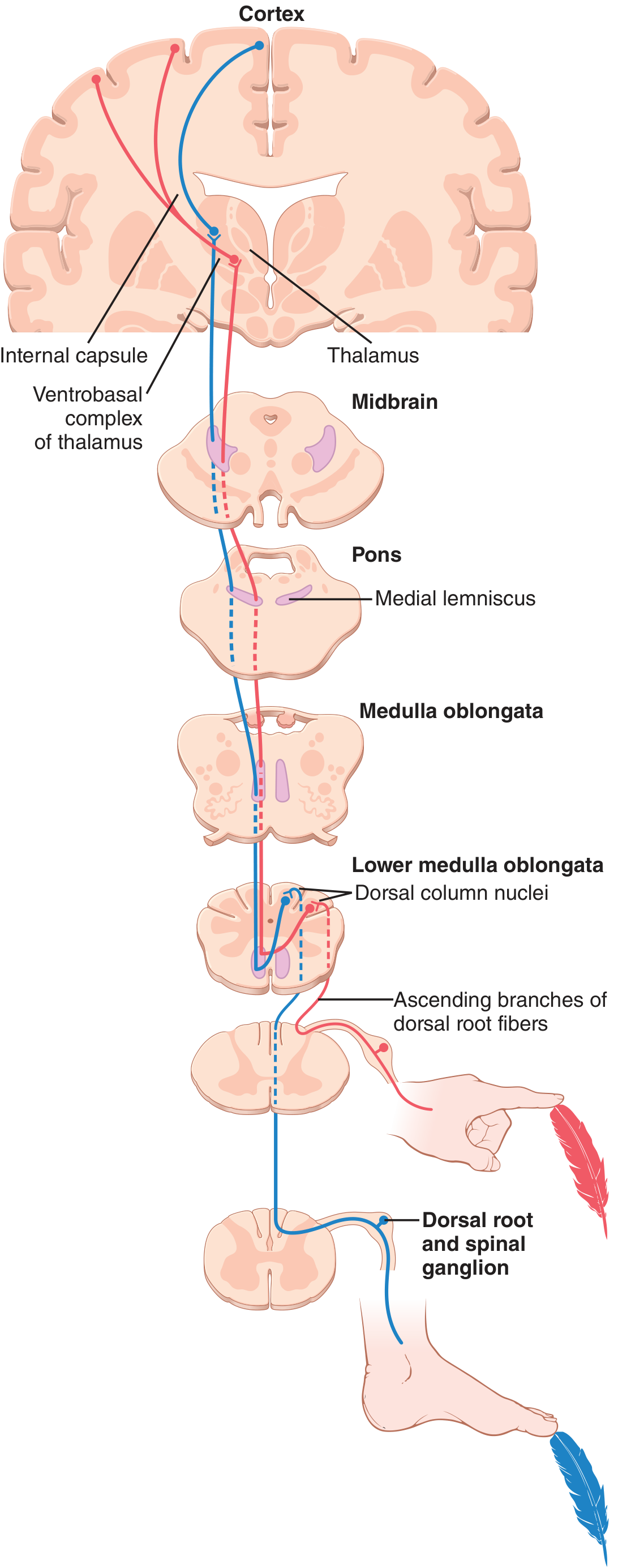
Figure 48.3 — Dorsal column–medial lemniscal pathway
Neuron 1 (Primary afferent):
- Large myelinated fibers from specialized mechanoreceptors (Meissner's corpuscles, Pacinian corpuscles, Merkel's discs, Ruffini endings, muscle spindles, joint receptors)
- Enter via the dorsal root → divide into a medial branch (ascends ipsilaterally in dorsal column without synapsing) and a lateral branch (enters dorsal horn gray for spinal reflexes and spinocerebellar tracts)
- Cell body in dorsal root ganglion (DRG)
Neuron 2 (Second-order):
- Medial branch ascends ipsilaterally in the dorsal column all the way to the dorsal medulla
- Lumbar/sacral fibers → fasciculus gracilis → synapse in nucleus gracilis
- Thoracic/cervical fibers → fasciculus cuneatus → synapse in nucleus cuneatus
- At the dorsal column nuclei, fibers decussate (cross) in the sensory decussation of the medulla
- Then ascend as the medial lemniscus through the contralateral brain stem (pons, midbrain)
- Also joined by trigeminal sensory fibers (face sensation) in the brain stem
Neuron 3 (Third-order):
- Medial lemniscus terminates in the ventrobasal complex (VPL/VPM) of the thalamus
- Projects via the internal capsule (posterior limb) to the postcentral gyrus = Somatosensory Area I (S-I)
- Also projects to Somatosensory Area II (smaller, lateral parietal cortex)
Spatial Orientation (Somatotopy)
A key distinguishing feature: strict somatotopic organization is maintained throughout.
- In the dorsal columns: lower body fibers lie medially, upper body fibers laterally
- In the medial lemniscus (after crossing): lower body is lateral, upper body medial
- In the thalamus and cortex: precise body map preserved
2. Anterolateral System (ALS)
Sensations Carried
- Pain (fast and slow)
- Thermal sensations (warm and cold)
- Crude touch and pressure (only rough localization)
- Tickle and itch
- Sexual sensations
Anatomy — 3-Neuron Arc
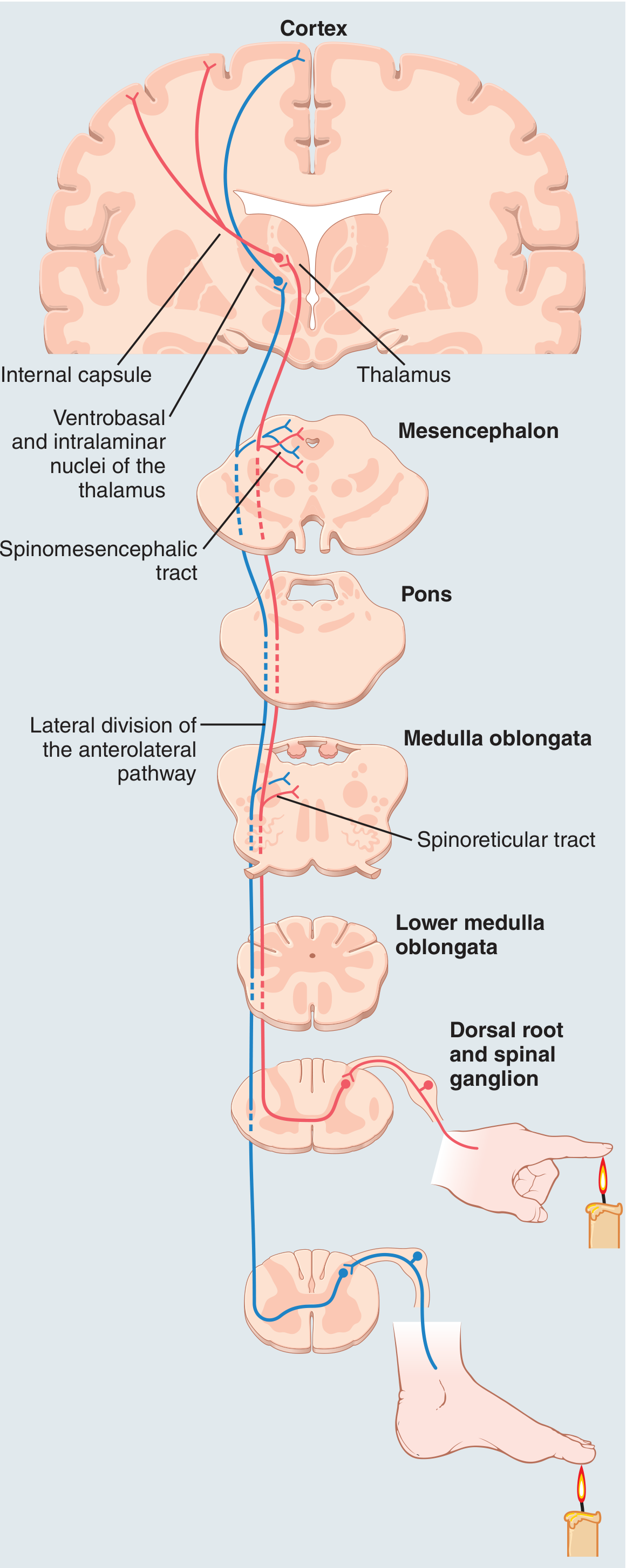
Figure 48.13 — Anterior and lateral divisions of the anterolateral pathway
Neuron 1 (Primary afferent):
- Aδ fibers (fast pain, temperature) and C fibers (slow/chronic pain) — cell bodies in DRG
- Enter via the dorsal root → synapse immediately in the dorsal horn gray matter at laminae I, IV, V, VI (Rexed laminae)
Neuron 2 (Second-order):
- Cross immediately to the opposite side of the spinal cord via the anterior commissure at the same or 1–2 segments above entry level
- Ascend in the anterior and lateral white columns:
- Lateral spinothalamic tract — pain and temperature
- Anterior spinothalamic tract — crude touch and pressure
- En route, collaterals branch off to reticular nuclei of the brain stem (especially for pain signals)
Neuron 3 (Third-order):
- Tactile signals → ventrobasal complex of thalamus → postcentral gyrus (S-I)
- Pain signals → mostly to reticular nuclei of brain stem first → then to intralaminar nuclei of thalamus → widely distributed; only a small fraction go directly to ventrobasal complex
Characteristics of ALS Transmission
- Velocity only 1/3 to 1/2 of DCML (8–40 m/sec)
- Poor spatial localization — only 10–20 gradations of intensity
- Cannot transmit rapidly changing or repetitive signals
- Broad modality capability (pain, temp, itch, crude touch) — something the DCML cannot do
3. Spinal Cord Cross-Section — Tract Locations
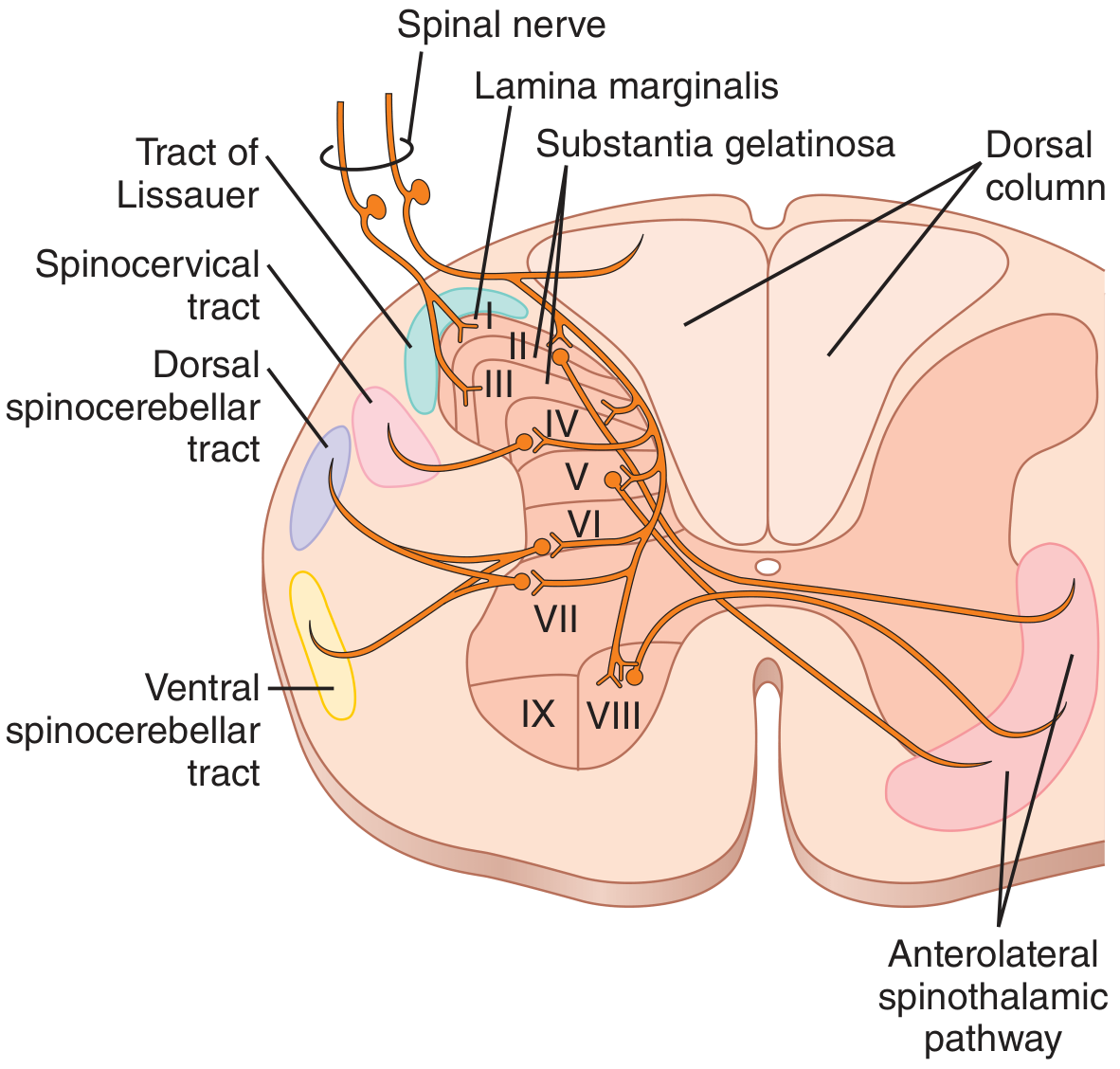
Figure 48.2 — Cross section of spinal cord showing ascending sensory tracts
Key anatomical features:
- Dorsal columns: medial (fasciculus gracilis — lower body) and lateral (fasciculus cuneatus — upper body)
- Anterolateral spinothalamic pathway: ventrolateral white matter
- Substantia gelatinosa (laminae II–III): primary synapse site for C fiber (slow pain) inputs
- Lamina marginalis (lamina I): primary synapse site for Aδ fast pain fibers
- Tract of Lissauer: carries pain fibers 1–2 segments rostrally/caudally before entering dorsal horn
4. Pain Transmission in ALS — Dual Sub-Pathways
| Feature | Neospinothalamic (Fast Pain) | Paleospinothalamic (Slow Pain) |
|---|---|---|
| Fiber type | Aδ | C |
| 1st synapse in cord | Lamina I (lamina marginalis) | Laminae II–III (substantia gelatinosa) → then lamina V |
| Neurotransmitter | Glutamate (fast, milliseconds) | Substance P (slow, builds over seconds) + glutamate |
| Thalamic target | Ventrobasal complex (+ posterior nuclear group) | Intralaminar nuclei (after brain stem reticular relay) |
| Localization | Reasonably good (fast, sharp, well-localized) | Poor (diffuse, burning, poorly localized) |
| Cortical destination | Somatosensory cortex | Widely diffuse; limbic system |
| Brain stem synapses | Few (mostly pass through) | Extensive — reticular formation, periaqueductal gray |
- Glutamate = transmitter of fast pain (Aδ) — brief action
- Substance P = transmitter of slow/chronic pain (C fibers) — builds over seconds to minutes; explains the "double pain" sensation after a pinprick
5. Key Differences Summary
| DCML | ALS | |
|---|---|---|
| Crosses | Medulla (contralateral after dorsal column nuclei) | Spinal cord (at entry level, via anterior commissure) |
| Location in cord | Dorsal white columns | Anterolateral white columns |
| 1st synapse | Dorsal column nuclei (medulla) | Dorsal horn (same level) |
| Speed | Fast (30–110 m/sec) | Slower (8–40 m/sec) |
| Modalities | Fine touch, vibration, proprioception | Pain, temperature, crude touch, itch |
| Discrimination | Precise (~100 gradations) | Crude (10–20 gradations) |
Clinical Correlate
- A hemisection of the spinal cord (Brown-Séquard syndrome) produces:
- Ipsilateral loss of DCML sensations (fine touch, vibration, proprioception) below the lesion
- Contralateral loss of ALS sensations (pain, temperature) 1–2 levels below the lesion
- This is because DCML crosses in the medulla, while ALS crosses immediately in the cord
Source: Guyton and Hall Textbook of Medical Physiology, Chapter 48 (Somatic Sensations I — General Organization) and Chapter 49 (Pain, Headache, and Thermal Sensations), pp. 596–611
This is a shared conversation. Sign in to Orris to start your own chat.