Ecg
Asking for Preferences
Reading File
Finding Sources
Searching Images
ECG basic interpretation waveforms P QRS T
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Now I have enough rich material to build a comprehensive guide. Let me compile it.
ECG Basic Interpretation — A Systematic Guide
1. What the ECG Records
The ECG records the electrical activity of the heart from the body surface. The heart's conduction system generates electrical signals that cause depolarization (contraction) and repolarization (recovery) of cardiac muscle. Each electrical event produces a characteristic waveform on the ECG.
The cardiac conduction pathway:
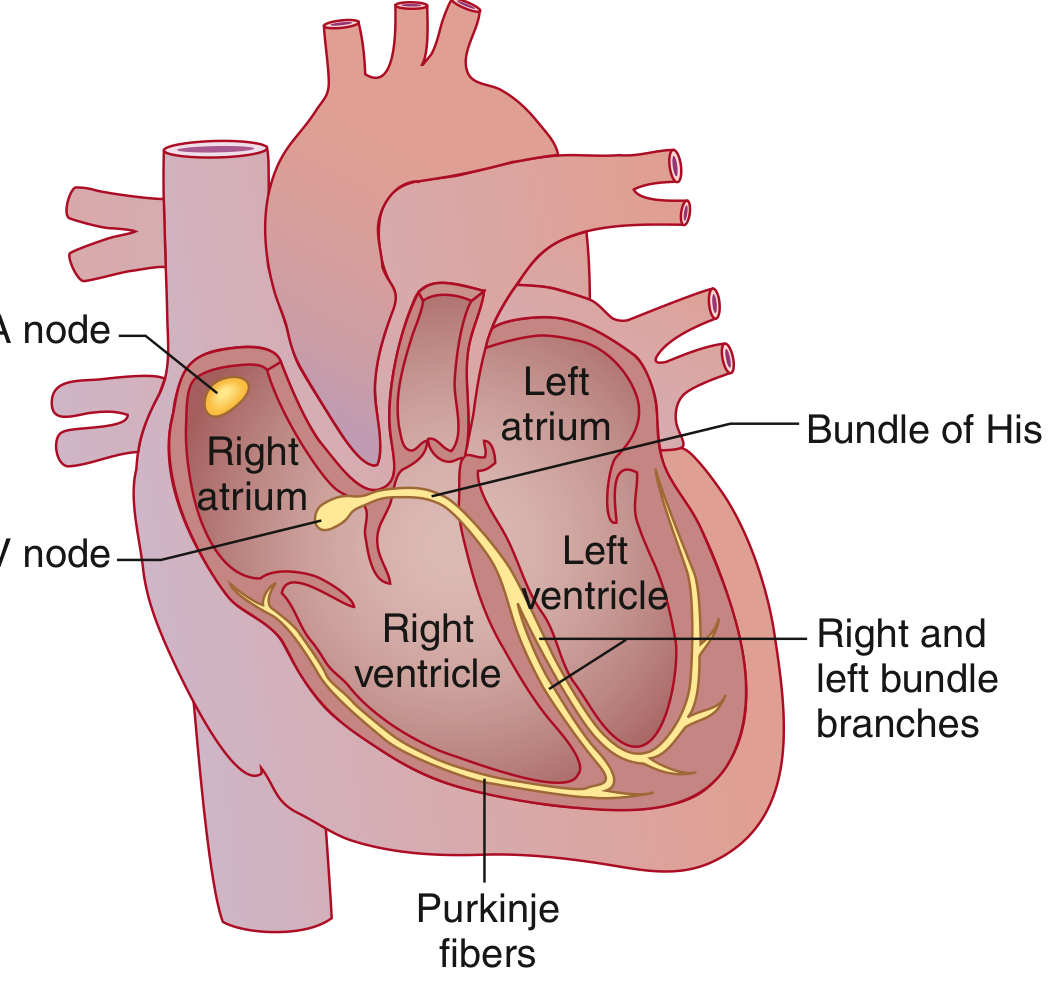
The sequence: SA node (right atrium) → spreads through both atria → AV node (physiological delay) → Bundle of His → right and left bundle branches → Purkinje fibers → ventricular muscle.
(Goldman-Cecil Medicine, Cardiac Conduction System)
2. The ECG Waveforms
| Wave / Interval | What it represents | Normal duration |
|---|---|---|
| P wave | Atrial depolarization | < 120 ms, amplitude < 2.5 mm |
| PR interval | Atrial-to-ventricular conduction (AV node + His-Purkinje) | 120–200 ms (3–5 small boxes) |
| QRS complex | Ventricular depolarization | < 120 ms (< 3 small boxes) |
| ST segment | Early ventricular repolarization | Isoelectric (flat, at baseline) |
| T wave | Ventricular repolarization | Upright in most leads; inverted in aVR normally |
| QT interval | Total ventricular electrical activity | < 440 ms (men), < 460 ms (women) |
| U wave | Afterdepolarizations (late repolarization) | Rarely seen; most prominent in V2–V3 |
Key point: The P wave and QRS complex are depolarization waves. The T wave is a repolarization wave. (Guyton & Hall Medical Physiology)
3. The ECG Paper
- Paper speed: 25 mm/sec (standard)
- Small box (1 mm): 0.04 sec (40 ms) horizontally; 0.1 mV vertically
- Large box (5 mm): 0.20 sec (200 ms) horizontally; 0.5 mV vertically
- Calibration: 1 mV = 10 mm (two large boxes) height
(Goldman-Cecil Medicine)
4. The 12 Leads
A standard ECG uses 12 leads that view the heart from different angles:
Limb leads (frontal plane):
- I, II, III — Standard bipolar leads
- aVR, aVL, aVF — Augmented unipolar leads
Chest (precordial) leads (horizontal plane):
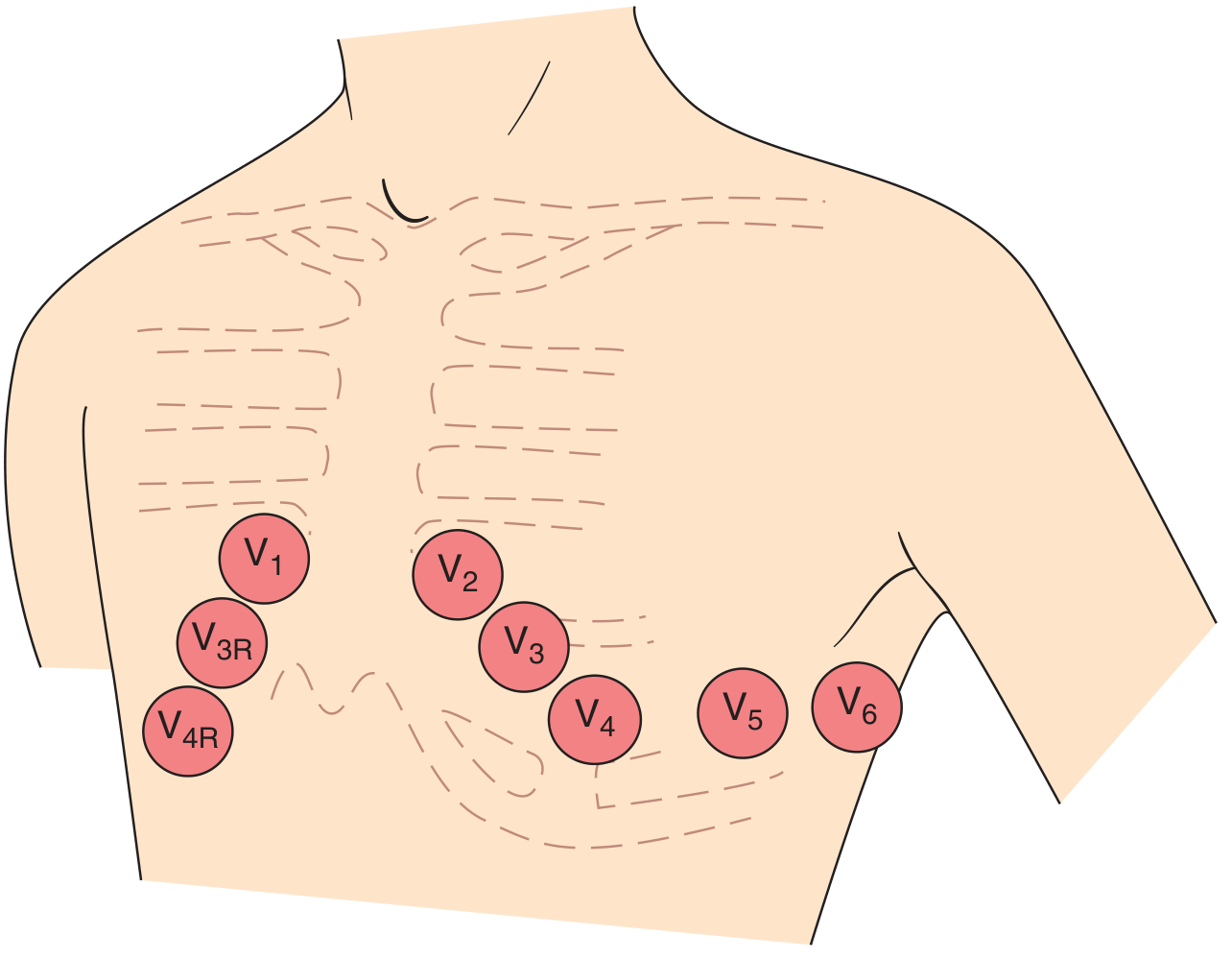
- V1 — Right sternal border, 4th intercostal space
- V2 — Left sternal border, 4th ICS
- V3 — Between V2 and V4
- V4 — Left midclavicular line, 5th ICS
- V5 — Anterior axillary line
- V6 — Midaxillary line
(Harrison's Principles of Internal Medicine, 22nd Ed.)
5. QRS Complex in the Chest Leads: R-wave Progression
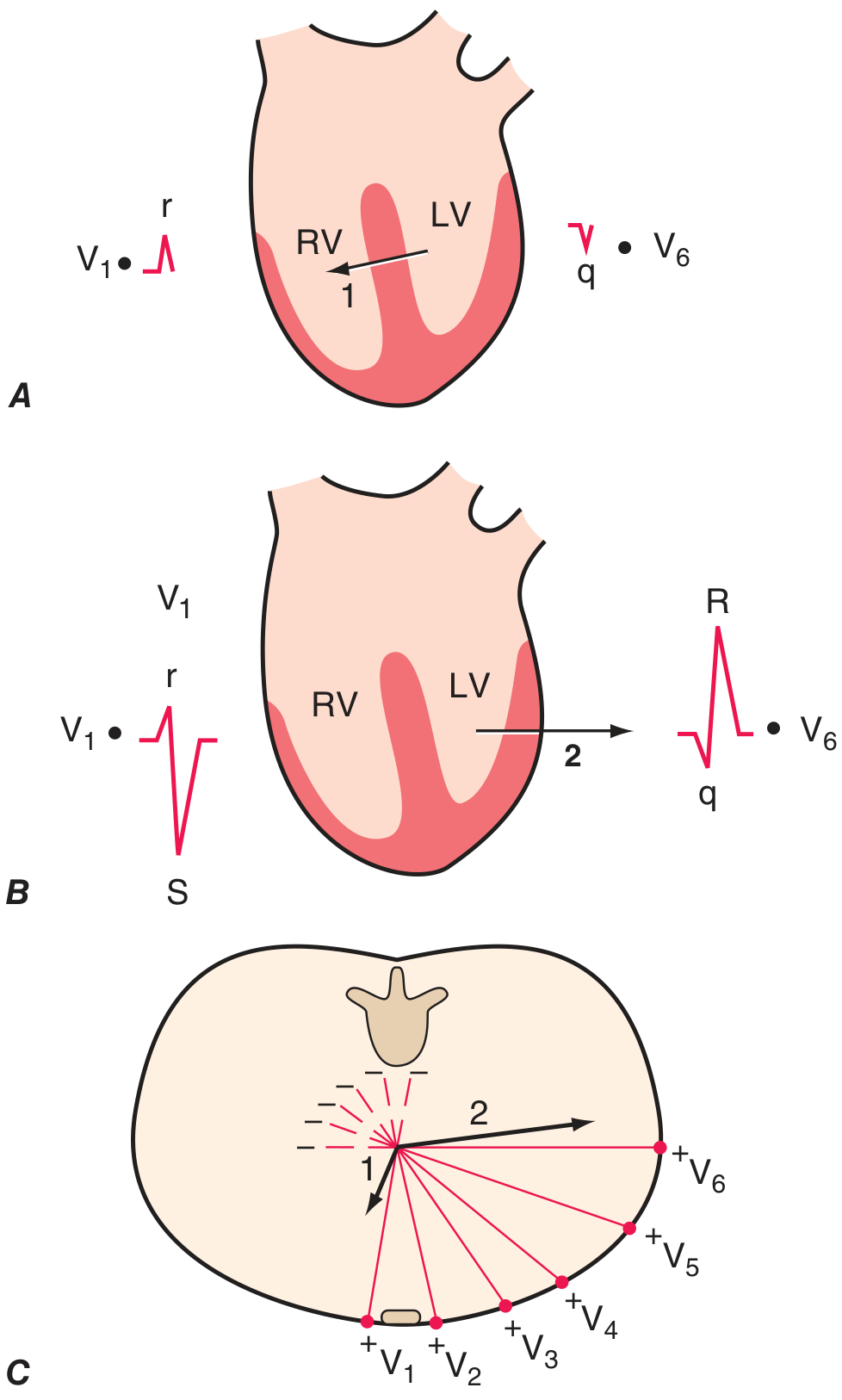
Ventricular depolarization has two phases:
- Septal depolarization (left → right): produces a small r in V1 and small q in V6
- Main ventricular depolarization (left ventricle dominant, pointing left/posteriorly): produces a deep S in V1 and tall R in V6
R waves should progressively increase from V1 → V4/V5 ("R-wave progression"). The transition zone (where R = S) is normally at V3 or V4.
(Harrison's Principles of Internal Medicine, 22nd Ed.)
6. Systematic 14-Step Approach to Every ECG
Harrison's recommends analyzing these parameters on every ECG:
- Standardization & technical features — Is calibration 10 mm/mV? Are all leads present? Any artifact?
- Rhythm — Sinus? Regular? Is there a P before every QRS?
- Heart rate — Count RR intervals (300 ÷ large boxes between R waves, or 1500 ÷ small boxes)
- PR interval — Normal 120–200 ms? Short (pre-excitation) or long (AV block)?
- QRS duration — Normal < 120 ms? Wide QRS = BBB or ventricular rhythm
- QT/QTc interval — Prolonged QTc raises risk of torsades de pointes
- Mean QRS axis — Normal −30° to +100°
- P waves — Morphology, upright in II, biphasic in V1
- QRS voltages — High = ventricular hypertrophy; low = effusion, COPD, obesity
- R-wave progression — V1 → V6 as above
- Abnormal Q waves — Pathologic if ≥ 40 ms wide or ≥ 25% of R amplitude → suggests prior MI
- ST segments — Elevation (injury/STEMI) or depression (ischemia/strain)
- T waves — Inversion, peaking, symmetry
- U waves — Prominent U waves → hypokalemia
Always compare with a prior ECG if available.
(Harrison's Principles of Internal Medicine, 22nd Ed.)
7. Quick Heart Rate Calculation
| Large boxes between R waves | Heart rate (bpm) |
|---|---|
| 1 | 300 |
| 2 | 150 |
| 3 | 100 |
| 4 | 75 |
| 5 | 60 |
| 6 | 50 |
Mnemonic: 300 – 150 – 100 – 75 – 60 – 50
8. Normal ECG Summary
A normal ECG shows:
- Sinus rhythm: regular P waves, each followed by a QRS
- HR: 60–100 bpm
- PR: 120–200 ms
- QRS: < 120 ms, normal axis, normal R-wave progression
- ST segments: isoelectric
- T waves: upright in I, II, V4–V6; inverted in aVR (normal); may be inverted in V1 normally
- Small septal q waves in V5–V6 are normal
- Sinus arrhythmia (slight RR variation with breathing) is normal, especially in young people
(Goldman-Cecil Medicine)
Key Reference Works
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025), Chapter 247
- Goldman-Cecil Medicine, Chapter 42
- Guyton and Hall Textbook of Medical Physiology, Chapter 11
This is a shared conversation. Sign in to Orris to start your own chat.