A 60 year old hypertensive presented with weakness and inability to move his right upper and lower extremities since last 2 hours. After admission in nearby hospital, clinic examination revealed increased muscle tone, exaggerated tendon jerks and extensor plantar response on his right side. i) What can be the probable diagnosis? ii) Explain the reason planter response is altered here? iv) Describe the corticospinal tract with a suitable behind the increased muscle tone and exaggerated tendon jerks in this patient. iii) Why the BJMA diagram.1
Clinical Case Analysis: Right Hemiplegia in a Hypertensive 60-Year-Old
i) Probable Diagnosis
- 60-year-old hypertensive - hypertension is the single most important risk factor for stroke
- Acute onset (2 hours) - sudden neurological deficits are characteristic of vascular events
- Right upper + lower extremity weakness - contralateral hemiplegia (left hemisphere lesion affecting the right side of the body)
- Increased tone, exaggerated tendon jerks, extensor plantar response - the classic triad of UMN (pyramidal tract) involvement
ii) Reason for Increased Muscle Tone and Exaggerated Tendon Jerks (Spasticity and Hyperreflexia)
Spasticity (Increased Muscle Tone)
- Loss of the dorsal reticulospinal tract (inhibitory) removes the brake on spinal motor neurons.
- The medial reticulospinal and vestibulospinal tracts, which facilitate extensor tone, are relatively spared.
- The imbalance results in unopposed excitatory drive on alpha motor neurons in the spinal cord's anterior horn.
- Additionally, there is disinhibition of gamma (fusimotor) motor neurons, which increase the sensitivity of muscle spindles - causing an exaggerated response to muscle stretch.
"Increased tone and hyperreflexia do not occur in experimental animals when a selective lesion is made in the corticospinal tract alone. It has therefore been hypothesized that spasticity is caused by damage to descending inhibitory pathways that travel closely with the corticospinal tract." - Neuroanatomy through Clinical Cases, 3rd Ed.
"The heightened stretch reflexes (tendon jerks) of the spastic state may be a 'release' phenomenon - the result of interruption of descending inhibitory pathways... mediated through disinhibition of spindle efferents (increased tonic activity of gamma motor neurons)." - Adams and Victor's Principles of Neurology, 12th Ed.
iii) Why the Plantar Response is Altered (Babinski Sign / Extensor Plantar Response)
Normal Plantar Response
Extensor Plantar Response (Babinski Sign)
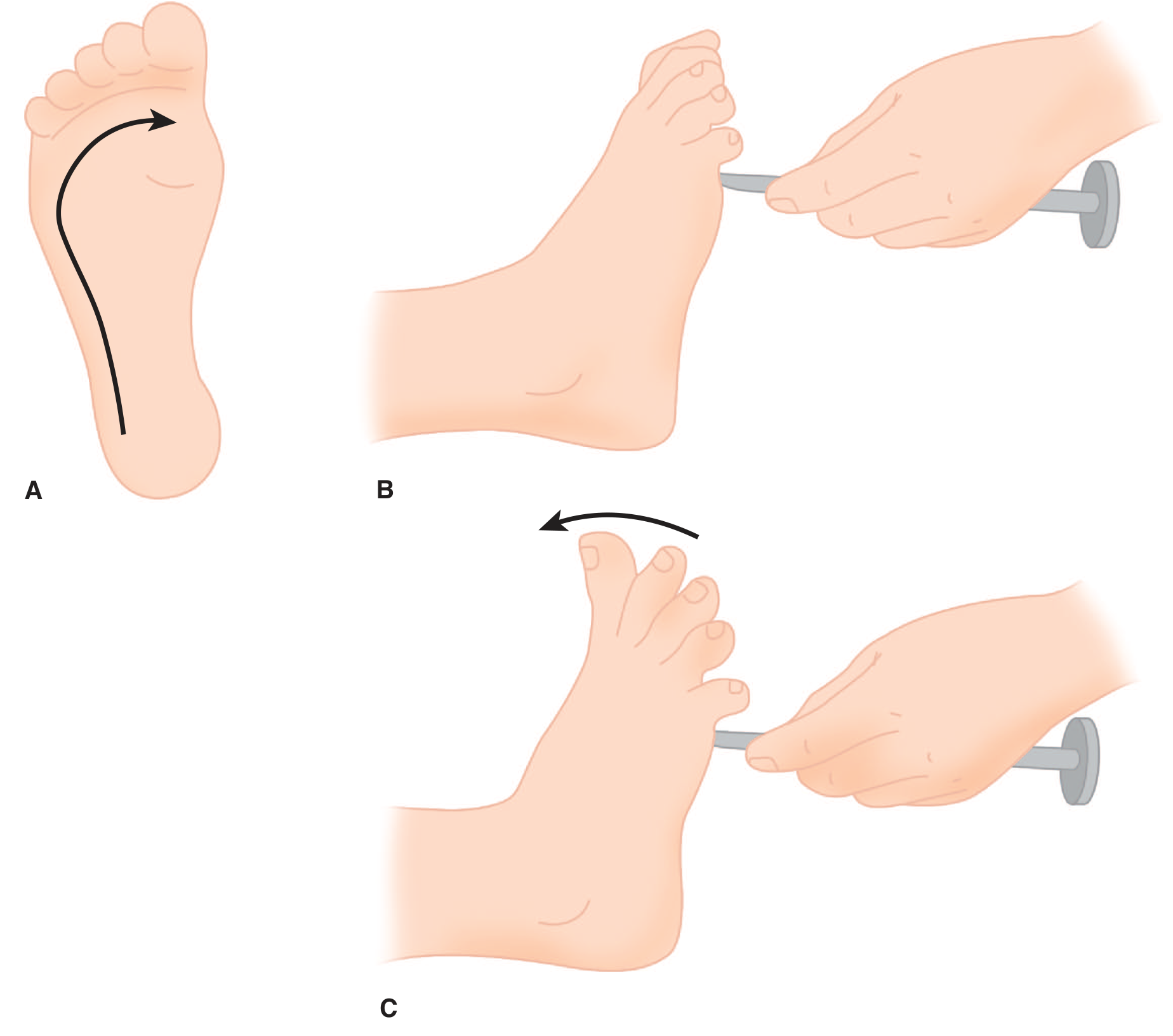
- The UMN normally exerts tonic descending inhibition over a primitive flexion-withdrawal (nociceptive) reflex arc in the spinal cord.
- When the UMN pathway is damaged (stroke), this inhibitory control is removed.
- The plantar reflex is then "released" - it reverts to the primitive spinal reflex pattern: extension of the great toe as part of a generalized leg flexion (withdrawal) synergy.
- As Adams and Victor note: "The extension movement of the great toe is a component of a larger synergistic flexion or shortening reflex of the leg - a protective (nocifensive) response."
- This sign is present normally in infants (before corticospinal myelination is complete) and reappears in adults only when corticospinal pathways are damaged.
iv) The Corticospinal Tract - Course and Description
Diagram
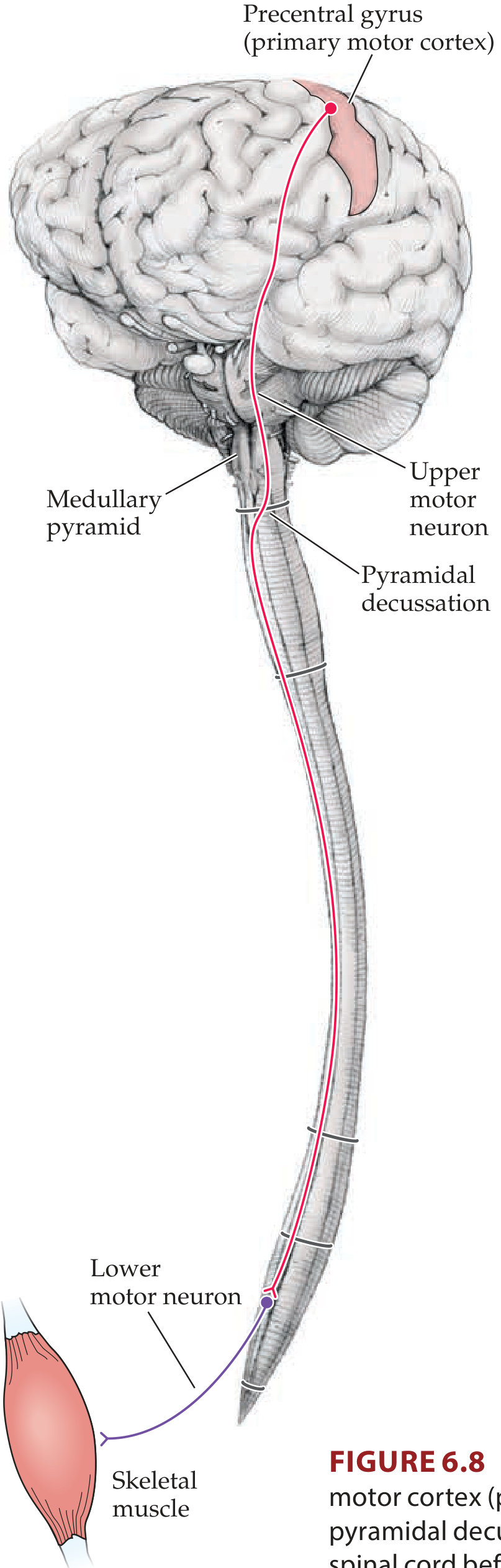
Origin
- Arises from the primary motor cortex (Brodmann area 4) in the precentral gyrus - >50% of fibers
- Additional fibers from premotor/supplementary motor cortex (area 6) and somatosensory cortex (areas 3, 1, 2, 5, 7)
- Special large neurons called Betz cells (giant pyramidal cells, layer V) contribute approximately 3% of fibers - the largest neurons in the human nervous system
- ~1 million axons total in the medullary pyramid (far exceeding the ~25,000-35,000 Betz cells)
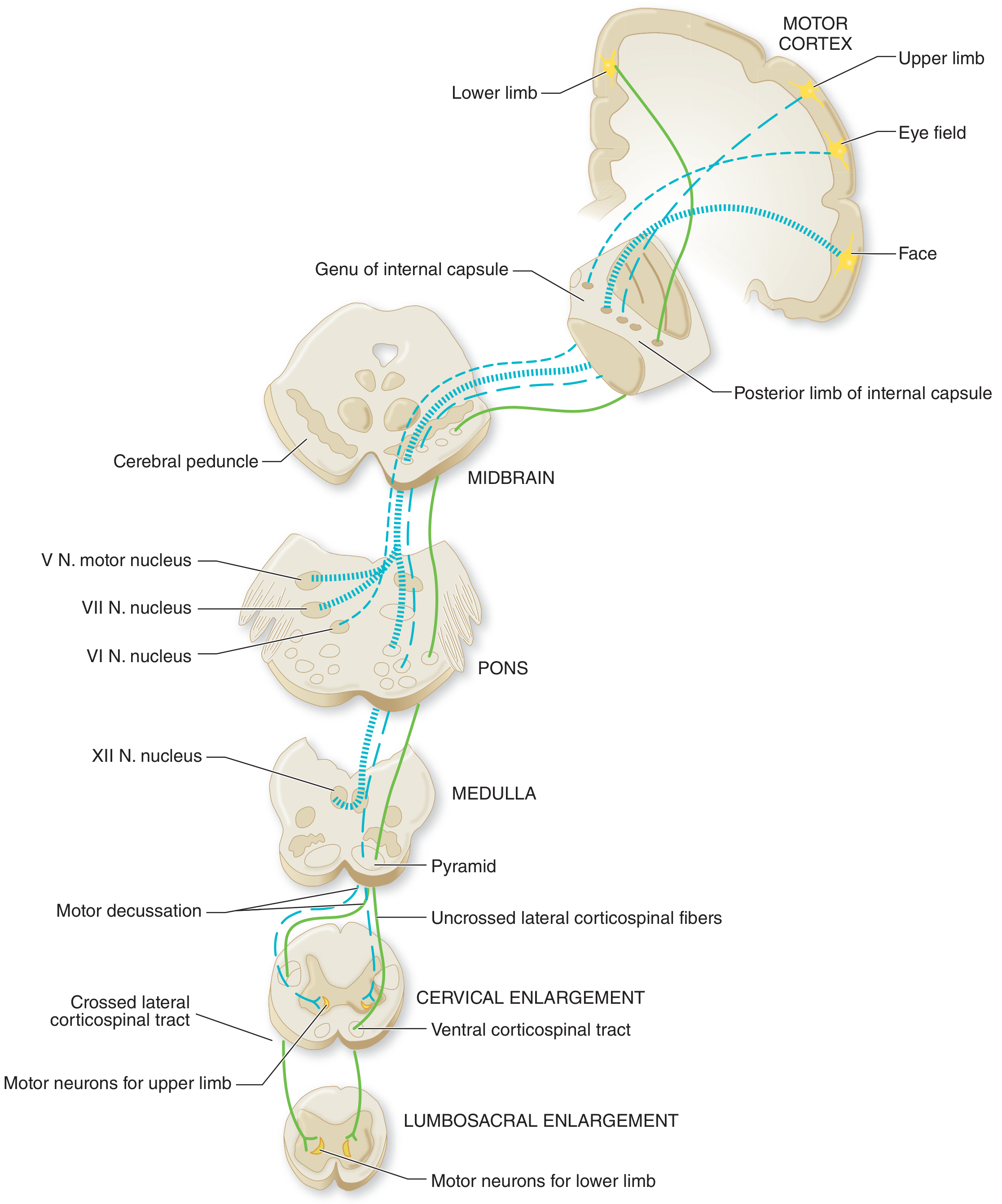
Course (Step-by-Step)
| Segment | Structure | Key Points |
|---|---|---|
| 1 | Cerebral cortex | Origin in precentral gyrus (Brodmann area 4, 6) |
| 2 | Corona radiata | Subcortical white matter fan |
| 3 | Internal capsule - posterior limb | Fibers compacted; face (anterior), arm/hand (central), leg/foot (posterior) |
| 4 | Cerebral peduncle (basis pedunculi, midbrain) | Middle portion; somatotopic arrangement maintained |
| 5 | Basis pontis | Fibers split into bundles interspersed with pontine nuclei |
| 6 | Medullary pyramid | Fibers reunite; visible on ventral surface of medulla |
| 7 | Pyramidal decussation (lower medulla) | ~75-80% of fibers cross to the contralateral side |
| 8 | Lateral corticospinal tract | Descends in the lateral funiculus (posterolateral white matter column) of spinal cord |
| 9 | Ventral corticospinal tract | ~20-25% uncrossed fibers descend ipsilaterally in anterior funiculus |
| 10 | Anterior horn (spinal cord) | Synapses on lower motor neurons (alpha) directly and via interneurons |
Key Facts
- The lateral corticospinal tract is the only direct long-fiber connection between the cerebral cortex and the spinal cord
- "Pyramidal tract" strictly refers to the portion traveling through the medullary pyramid
- The broader term "upper motor neuron" also includes indirect pathways: rubrospinal, reticulospinal, vestibulospinal, tectospinal tracts
- The UMN is a two-neuron pathway: Upper motor neuron (cortex to anterior horn) → Lower motor neuron (anterior horn to muscle)
Summary Table: UMN vs LMN Signs
| Feature | UMN Lesion (this patient) | LMN Lesion |
|---|---|---|
| Weakness | Yes | Yes |
| Muscle atrophy | No (mild disuse later) | Yes (early, prominent) |
| Fasciculations | No | Yes |
| Muscle tone | Increased (spasticity) | Decreased (flaccidity) |
| Tendon reflexes | Increased (hyperreflexia) | Decreased/absent |
| Plantar response | Extensor (Babinski +ve) | Flexor (normal) |
A 60 year old hypertensive presented with weakness and inability to move his right upper and lower extremities since last 2 hours. After admission in nearby hospital, clinic examination revealed increased muscle tone, exaggerated tendon jerks and extensor plantar response on his right side. i) What can be the probable diagnosis? ii) Explain the reason behind increased muscle tone and exaggerated tendon Jerks Iii) why planter response is altered here? iv) Describe the corticospinal tract with a suitable
Clinical Case: Right Hemiplegia in a 60-Year-Old Hypertensive
i) Probable Diagnosis
- 60-year-old + hypertension = strongest risk factor for stroke
- Acute onset (2 hours) = vascular event (ischaemic or haemorrhagic stroke)
- Right upper + lower limb weakness = the left motor cortex/left corticospinal tract controls the right side of the body (crossed pathway)
- Increased tone + exaggerated jerks + extensor plantar = classic triad of UMN (pyramidal tract) damage
ii) Reason for Increased Muscle Tone and Exaggerated Tendon Jerks
The Normal State
What Happens After a Stroke
- Loss of dorsal reticulospinal inhibition → removes the "brake" on anterior horn motor neurons
- Disinhibition of gamma (fusimotor) motor neurons → increases muscle spindle sensitivity → any stretch triggers an exaggerated response
- Relative preservation of the medial reticulospinal and vestibulospinal tracts (which facilitate extensor tone) → these now act unopposed
- Net result: anterior horn alpha motor neurons become hyperexcitable → increased resting tone (spasticity) + exaggerated tendon jerk reflexes (hyperreflexia)
"The heightened stretch reflexes of the spastic state may be a 'release' phenomenon - the result of interruption of descending inhibitory pathways... mediated through disinhibition of spindle efferents (increased tonic activity of gamma motor neurons) and through loss of reticulospinal and vestibulospinal influences on alpha motor neurons."
- Adams and Victor's Principles of Neurology, 12th Ed.
"Increased tone and hyperreflexia do not occur when a selective lesion is made in the corticospinal tract alone. Spasticity is caused by damage to descending inhibitory pathways that travel closely with the corticospinal tract."
- Neuroanatomy through Clinical Cases, 3rd Ed.
iii) Why the Plantar Response is Altered (Extensor Plantar Response / Babinski Sign)
Normal Plantar Response
In This Patient
Mechanism
- The UMN normally exerts tonic inhibition over a primitive nociceptive flexion-withdrawal reflex arc in the spinal cord
- When the corticospinal pathway is damaged, this inhibitory control is lost
- The plantar reflex reverts to the primitive spinal reflex pattern: the great toe extends as part of a generalised leg flexion/withdrawal synergy (also called the "triple flexion response" - hip, knee, ankle dorsiflex)
- From a physiological standpoint, toe extension IS part of limb withdrawal from a noxious stimulus - the dorsum of the great toe moves away from the ground/stimulus
- This response is normal in infants (corticospinal tract not yet myelinated) and reappears in adults only when the corticospinal pathway is damaged
"The extension movement of the great toe is a component of a larger synergistic flexion reflex of the leg - a protective (nocifensive) response. The Babinski sign is the most reliable indication of an upper motor neuron lesion."
- Adams and Victor's Principles of Neurology, 12th Ed.
iv) The Corticospinal Tract
Diagram 1 - Overview of the Two-Neuron Motor Pathway
Diagram 2 - Full Course from Cortex to Spinal Cord
Origin
| Source | Contribution |
|---|---|
| Primary motor cortex - precentral gyrus (Brodmann area 4) | >50% of fibers |
| Premotor + supplementary motor cortex (area 6) | ~30% |
| Somatosensory cortex (areas 3, 1, 2, 5, 7) | ~40% (parietal) |
| Betz cells (giant pyramidal neurons, cortical layer V) | Only ~3% but the largest neurons in the CNS |
Step-by-Step Course
- Face fibers → anterior part of posterior limb
- Arm/hand fibers → middle part
- Leg/foot fibers → posterior part
- Alpha motor neurons directly (especially for fine, skilled movements of distal muscles)
- Spinal interneurons (for most proximal muscle movements)
Summary Table
| Level | Structure |
|---|---|
| Cortex | Precentral gyrus (area 4, 6) - Betz cells |
| White matter | Corona radiata |
| Diencephalon | Posterior limb of internal capsule |
| Midbrain | Cerebral peduncle (basis pedunculi) |
| Pons | Basis pontis (scattered bundles) |
| Medulla | Medullary pyramid |
| Junction | Pyramidal decussation (75-80% cross) |
| Spinal cord | Lateral corticospinal tract (crossed) + Ventral CST (uncrossed) |
| Termination | Anterior horn - alpha motor neurons / interneurons |
Key Terminology Distinctions
- Corticospinal tract = fibers from cortex to spinal cord
- Pyramidal tract = strictly the portion running through the medullary pyramid
- Upper motor neuron (UMN) = broader term including all descending pathways (corticospinal + rubrospinal + reticulospinal + vestibulospinal + tectospinal)
- These terms are not interchangeable, though often loosely used as such in clinical practice
UMN vs LMN Signs - Summary Table
| Feature | UMN Lesion (this patient) | LMN Lesion |
|---|---|---|
| Weakness | Yes (contralateral) | Yes (ipsilateral) |
| Muscle atrophy | Minimal/late (disuse) | Early and pronounced |
| Fasciculations | Absent | Present |
| Muscle tone | Increased (spasticity) | Decreased (flaccidity) |
| Tendon reflexes | Exaggerated (hyperreflexia) | Diminished/absent |
| Plantar response | Extensor - Babinski positive | Flexor (normal) |
| Clonus | May be present | Absent |
Is it will be right or left side
The Lesion is on the LEFT Side
The Corticospinal Tract Crosses (Decussates)
- Left motor cortex → controls → Right side of body
- Right motor cortex → controls → Left side of body
Applying to This Patient
| Finding | Side |
|---|---|
| Weakness, increased tone, exaggerated jerks, Babinski sign | Right side (the affected body side) |
| Brain lesion (stroke in internal capsule / motor cortex) | Left side (opposite side of brain) |
Simple Rule to Remember
"The brain lesion is ALWAYS on the OPPOSITE side to the body weakness in UMN lesions above the pyramidal decussation."
- Symptoms → Right side of body
- Lesion → Left cerebral hemisphere (most likely left internal capsule, posterior limb)
Name the answer correct then
Corrected Diagnosis
Why LEFT Side?
LEFT Motor Cortex → Decussates at Medulla → Controls RIGHT body
Corrected Answer for All Parts
| Question | Corrected Answer |
|---|---|
| i) Diagnosis | Left-sided UMN lesion (Left hemisphere stroke) causing Right Hemiplegia |
| ii) Increased tone + jerks | Due to damage to left corticospinal + inhibitory pathways → releases spinal cord on the right side |
| iii) Extensor plantar | Right foot shows Babinski sign (positive) due to damage of left corticospinal tract |
| iv) Tract lesion site | Left internal capsule (posterior limb) - most likely location |
Key Rule
Body signs = RIGHT side Brain lesion = LEFT side (Because the tract crosses at the medullary pyramidal decussation)
Make the whole answer again with correction
Clinical Case Analysis: Right Hemiplegia in a 60-Year-Old Hypertensive
i) Probable Diagnosis
| Clinical Feature | Significance |
|---|---|
| 60 years old + hypertension | Strongest risk factor for stroke |
| Acute onset (2 hours) | Typical of a vascular (stroke) event |
| Right upper + lower limb weakness | LEFT brain lesion (crossed pathway) |
| Increased tone + exaggerated jerks + extensor plantar | Classic UMN (pyramidal tract) damage |
The corticospinal tract crosses at the pyramidal decussation in the lower medulla - so the LEFT motor cortex controls the RIGHT side of the body. A lesion in the LEFT hemisphere causes RIGHT-sided deficits.
ii) Reason for Increased Muscle Tone and Exaggerated Tendon Jerks
Normal State
After Left-Sided Stroke
"The heightened stretch reflexes of the spastic state may be a 'release' phenomenon - the result of interruption of descending inhibitory pathways... mediated through disinhibition of spindle efferents (increased tonic activity of gamma motor neurons)."
- Adams and Victor's Principles of Neurology, 12th Ed.
iii) Why the Plantar Response is Altered
Normal Plantar Response (in a healthy adult)
In This Patient - RIGHT Foot Shows Babinski Sign
- Dorsiflexion (upward extension) of the great toe
- Fanning (abduction) of the remaining toes
Mechanism
- The LEFT corticospinal tract normally sends tonic inhibitory signals down to suppress a primitive nociceptive flexion-withdrawal reflex arc in the right spinal cord
- The LEFT-sided stroke interrupts this inhibitory control
- The right-sided plantar reflex reverts to the primitive spinal pattern - the great toe extends as part of a generalised leg withdrawal synergy (triple flexion: hip + knee flex, ankle dorsiflexes)
- This response is normal in infants (before corticospinal myelination is complete) and reappears in adults only when the LEFT corticospinal pathway is damaged, causing the sign to appear on the RIGHT (contralateral) foot
"The Babinski sign is the most reliable indication of an upper motor neuron lesion."
- Adams and Victor's Principles of Neurology, 12th Ed.
iv) The Corticospinal Tract - Full Description with Diagrams
Diagram 1 - Two-Neuron Motor Pathway Overview
Diagram 2 - Complete Course from Cortex to Spinal Cord
Origin of the Corticospinal Tract
| Source | Contribution |
|---|---|
| Primary motor cortex - precentral gyrus (Brodmann area 4) | >50% of fibers |
| Premotor + supplementary motor cortex (area 6) | ~30% |
| Somatosensory cortex (areas 3, 1, 2, 5, 7) | ~40% (parietal) |
| Betz cells (giant pyramidal neurons, cortical layer V) | Only ~3% but the largest neurons in the CNS |
Step-by-Step Course
- Face fibers → anterior part of posterior limb
- Arm/hand fibers → middle part
- Leg/foot fibers → posterior part
- ~75-80% of fibers cross to the contralateral (RIGHT) side
- Remaining ~20-25% stay ipsilateral
- Upper limb fibers cross more rostrally than lower limb fibers
- This is why a LEFT brain lesion causes RIGHT body signs
- Alpha motor neurons directly (fine, skilled distal muscle movements)
- Spinal interneurons (proximal muscle movements)
Course Summary Table
| Level | Structure | Side |
|---|---|---|
| Origin | Precentral gyrus (area 4, 6) | LEFT |
| White matter | Corona radiata | LEFT |
| Diencephalon | Posterior limb of internal capsule | LEFT |
| Midbrain | Cerebral peduncle (basis pedunculi) | LEFT |
| Pons | Basis pontis | LEFT |
| Upper medulla | Medullary pyramid | LEFT |
| Lower medulla | Pyramidal decussation - CROSSES HERE | Crosses to RIGHT |
| Spinal cord | Lateral corticospinal tract | RIGHT |
| Termination | Anterior horn alpha motor neurons | RIGHT |
| Muscle | Skeletal muscle | RIGHT body |
Key Terminology
| Term | Definition |
|---|---|
| Corticospinal tract | Fibers from cortex to spinal cord |
| Pyramidal tract | Strictly the portion running through the medullary pyramid |
| Upper Motor Neuron (UMN) | Broader term - includes corticospinal + rubrospinal + reticulospinal + vestibulospinal + tectospinal |
| Lower Motor Neuron (LMN) | Anterior horn cell + its axon to muscle (the "final common pathway") |
UMN vs LMN Signs - Summary Table
| Feature | UMN Lesion - This Patient | LMN Lesion |
|---|---|---|
| Weakness | Yes - RIGHT side | Yes - ipsilateral |
| Muscle atrophy | Minimal (disuse only) | Early and prominent |
| Fasciculations | Absent | Present |
| Muscle tone | Increased (spasticity) - RIGHT | Decreased (flaccidity) |
| Tendon reflexes | Exaggerated (hyperreflexia) - RIGHT | Diminished/absent |
| Plantar response | Extensor Babinski+ - RIGHT foot | Flexor (normal) |
| Clonus | May be present on RIGHT | Absent |
| Lesion site | LEFT hemisphere/internal capsule | Anterior horn / peripheral nerve |
10-year old boy was brought to the clinic with recurrent events of unstable gait and complication of speech. He was diagnosed with cerebellar dysfunction. (i) Highlight the different types of neurons and their location in the cerebellar cortex, (ii) Discuss the physiological significance of the neuronal circuit of the cerebellum with a neat diagram. Identify and explain the divisions of cerebellum based on its function
Cerebellar Dysfunction in a 10-Year-Old Boy: Ataxic Gait and Dysarthria
Diagnosis
i) Neurons of the Cerebellar Cortex - Types and Locations
The Three Layers
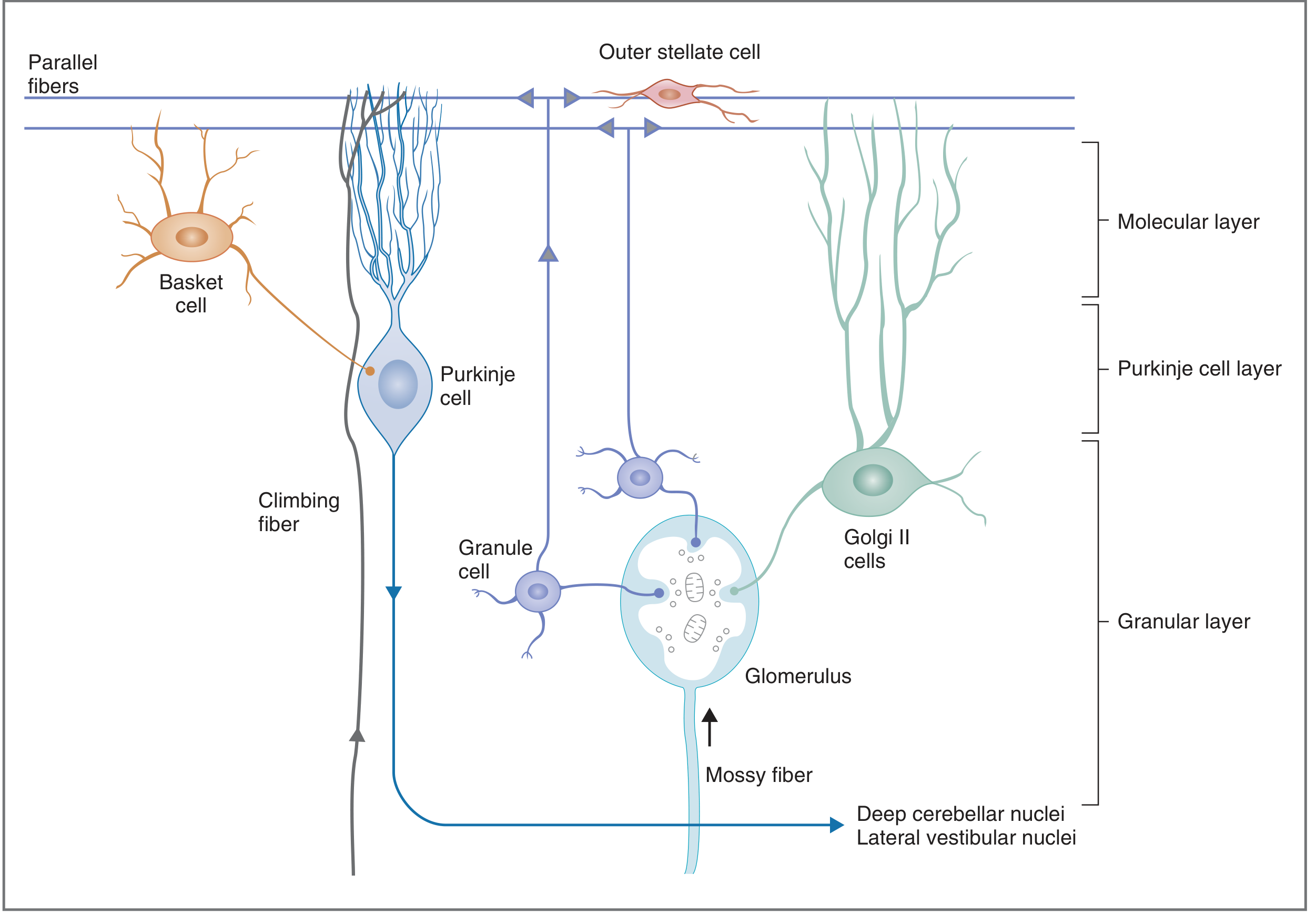
Layer 1: Molecular Layer (Outermost)
| Neuron | Type | Key Features |
|---|---|---|
| Stellate cells (outer stellate cells) | Inhibitory (GABA) | Located in the outer portion of the molecular layer; excited by granule cell parallel fibers; terminate on Purkinje cell dendrites - cause lateral inhibition |
| Basket cells | Inhibitory (GABA) | Located in the inner portion of the molecular layer; excited by parallel fibers; send axons that wrap around Purkinje cell bodies like a basket - powerful perisomatic inhibition |
Layer 2: Purkinje Cell Layer (Middle)
| Neuron | Type | Key Features |
|---|---|---|
| Purkinje cells | Inhibitory (GABA) - the ONLY output cell of the cerebellar cortex | The largest neurons in the cerebellum; have enormous, fan-shaped, highly branched dendritic trees oriented in the sagittal plane; each receives input from ~200,000 parallel fibers but from only ONE climbing fiber; their axons are the sole output of the cerebellar cortex, projecting to the deep cerebellar nuclei |
Layer 3: Granular Layer (Innermost - deepest)
| Neuron | Type | Key Features |
|---|---|---|
| Granule cells | Excitatory (Glutamate) - the ONLY excitatory neuron in cerebellar cortex | Most numerous neurons in the entire brain (~50 billion); receive excitatory input from mossy fibers in cerebellar glomeruli; their axons ascend to the molecular layer and bifurcate in a T-shape to form parallel fibers running along the long axis of the folium |
| Golgi cells (Golgi type II) | Inhibitory (GABA) | Located in the upper part of the granular layer; receive excitatory input from mossy fiber collaterals and parallel fibers; provide feedback inhibition onto granule cell dendrites (shortens duration of mossy fiber excitation - temporal signal sharpening) |
Memory Aid for Inhibitory vs Excitatory
"All axons projecting UPWARD are excitatory (mossy fibers, climbing fibers, granule cell parallel fibers). All axons projecting DOWNWARD are inhibitory (Purkinje cells, stellate cells, basket cells, Golgi cells). Outputs of deep cerebellar nuclei are always excitatory."
- Neuroanatomy through Clinical Cases, 3rd Ed.
ii) Physiological Significance of the Cerebellar Neuronal Circuit
Circuit Diagram
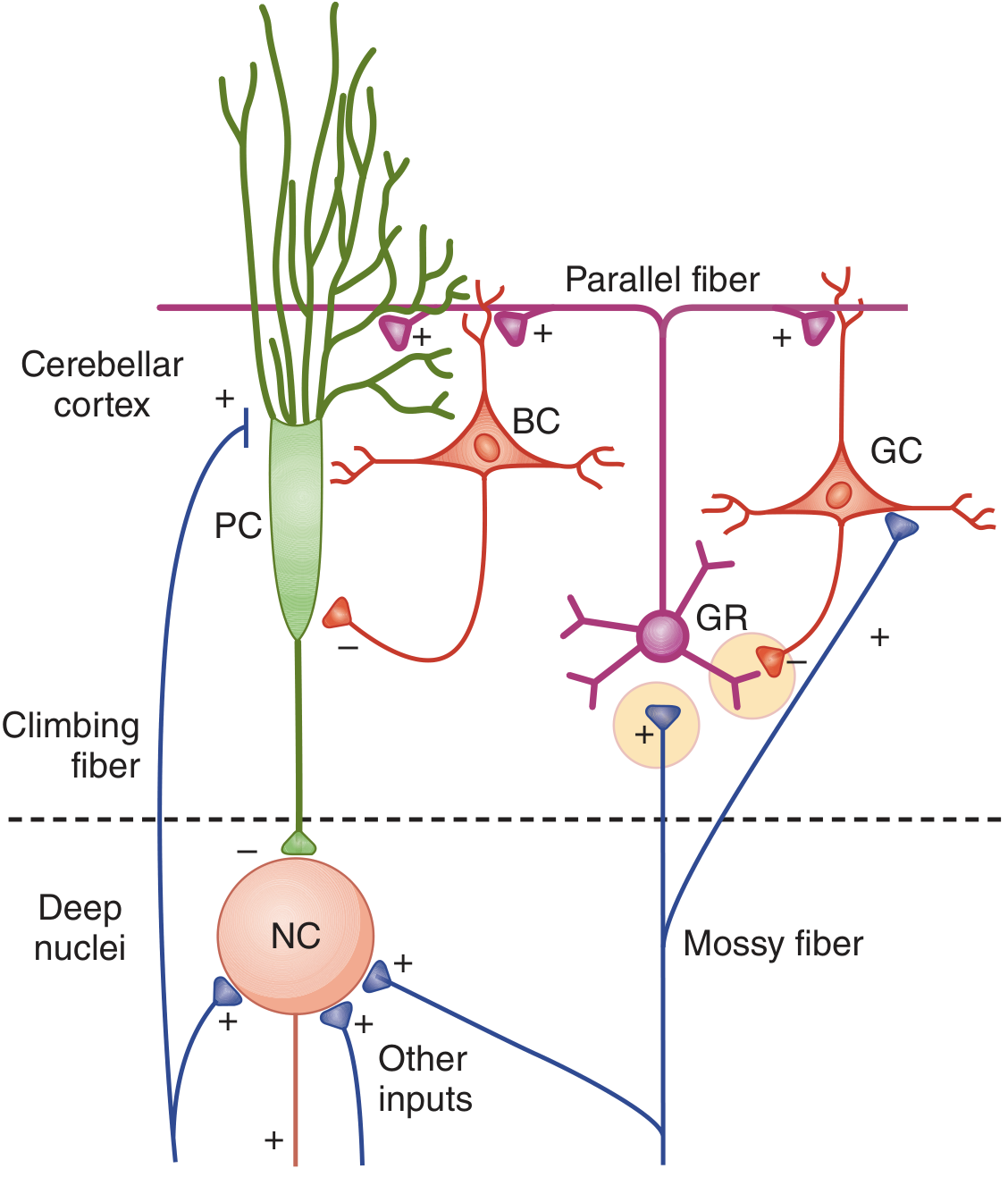

Two Major Input Systems
- Originates from: spinal cord (spinocerebellar tracts), pontine nuclei (corticopontine fibers), vestibular nuclei
- Mossy fibers synapse on granule cells in cerebellar glomeruli
- Granule cell axons → parallel fibers → weakly excite MANY Purkinje cells (divergent, widespread effect)
- Also excite basket cells, stellate cells, and Golgi cells via parallel fibers
- Originates exclusively from: inferior olivary nucleus of the medulla
- Each climbing fiber winds around the Purkinje cell dendrites like a vine
- Each Purkinje cell receives input from only ONE climbing fiber
- A single climbing fiber action potential powerfully excites a single Purkinje cell - produces complex spikes
- Thought to act as an error signal for motor learning (comparison of intended vs actual movement)
The Core Circuit - Step by Step
INPUTS
↓
Mossy fibers ──→ Granule cells ──→ Parallel fibers
↓ ↓ ↓
Purkinje Basket/ Golgi cells
cell(+) Stellate(-) (-)
↓ ↓
Inhibits adjacent Inhibits granule
Purkinje cells cells (feedback)
↓
Climbing fibers ──────────────→ Purkinje cell (powerful +)
PURKINJE CELL AXON (GABA - inhibitory)
↓
DEEP CEREBELLAR NUCLEI (also receive + collaterals from mossy/climbing fibers)
↓
EXCITATORY OUTPUT → Thalamus → Motor Cortex
→ Brainstem
Physiological Significance of Each Circuit Element
| Circuit Component | Physiological Role |
|---|---|
| Mossy fiber → Granule cell → Parallel fiber → Purkinje cell | Broad, convergent excitation; integrates sensory and motor planning information |
| Climbing fiber → Purkinje cell | Powerful error signal; drives motor learning and adaptation (long-term depression of parallel fiber-Purkinje synapse) |
| Basket + Stellate cells → adjacent Purkinje cells | Lateral (spatial) inhibition - sharpens the spatial precision of motor output (like lateral inhibition in the retina) |
| Golgi cell → Granule cells | Feedback (temporal) inhibition - limits the duration of mossy fiber excitation; sharpens timing of motor signals |
| Purkinje cell → Deep cerebellar nuclei | The ONLY output of the cerebellar cortex; tonically inhibits deep nuclei; modulates timing and extent of motor commands |
| Deep cerebellar nuclei → Thalamus/Brainstem | Final excitatory output - modulates motor cortex activity and brainstem motor centers |
Overall Physiological Role
iii) Functional Divisions of the Cerebellum
Diagram
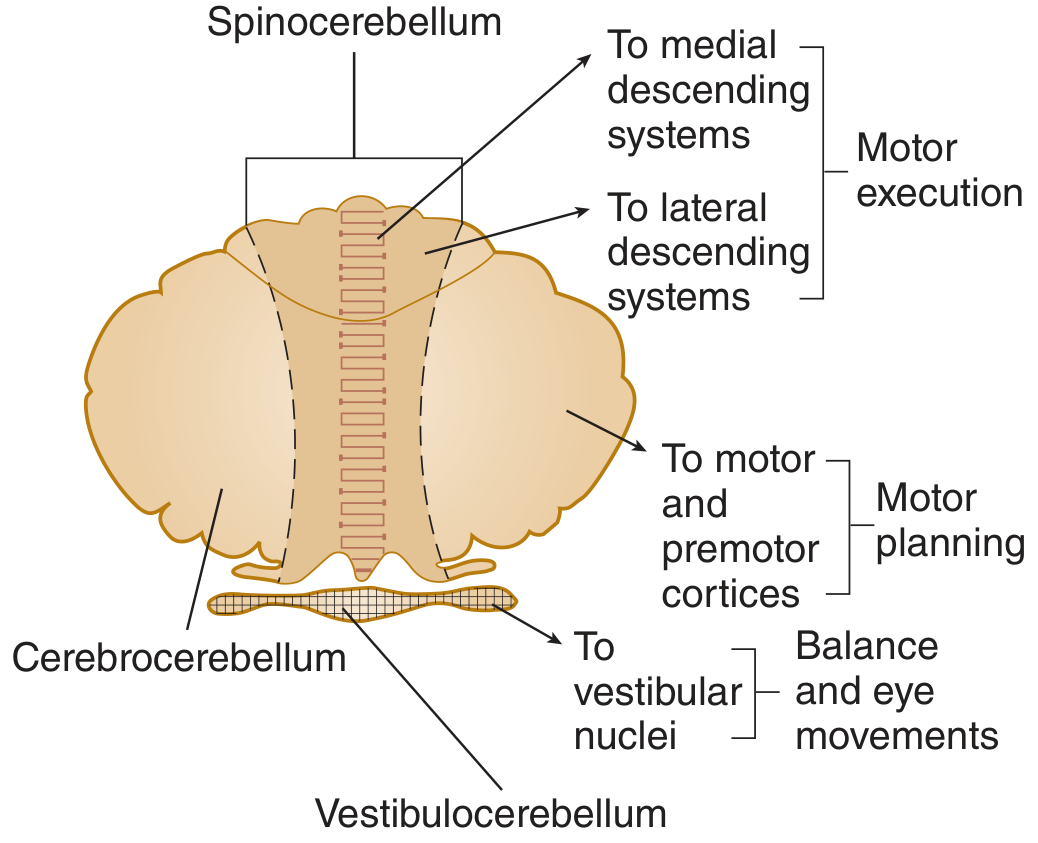
Division 1: Vestibulocerebellum (Archicerebellum)
| Feature | Details |
|---|---|
| Anatomic region | Flocculonodular lobe (flocculus + nodulus) |
| Evolutionary age | Oldest part (archicerebellum) |
| Major inputs | Vestibulocerebellar fibers (from labyrinths and vestibular nuclei) |
| Deep nucleus | No deep nucleus - projects directly to vestibular nuclei (lateral vestibular nucleus of Deiters) |
| Outputs | Vestibular nuclei → vestibulospinal tract |
| Functions | Equilibrium (balance), coordination of head + eye movements, adjusts posture in response to gravity |
| Dysfunction | Truncal ataxia, wide-based gait, nystagmus, inability to maintain balance - this boy's unstable gait could be partly from this division |
Division 2: Spinocerebellum (Paleocerebellum)
| Feature | Details |
|---|---|
| Anatomic region | Vermis + intermediate (paravermal) hemispheres of anterior and posterior lobes |
| Evolutionary age | Intermediate (paleocerebellum) |
| Major inputs | Dorsal + ventral spinocerebellar tracts (proprioception from muscles, tendons, joints); also receives copy of "motor plan" from motor cortex |
| Deep nuclei | Vermis → Fastigial nucleus; Intermediate hemisphere → Interposed nuclei (globose + emboliform) |
| Outputs | Fastigial → vestibulospinal + reticulospinal (axial/postural muscles); Interposed → contralateral red nucleus → rubrospinal tract (limb muscles) |
| Functions | Coordination of ongoing limb and axial movements; postural control during movement; correction of errors in movement execution |
| Dysfunction | Limb ataxia, dysmetria (past-pointing), hypotonia, intention tremor |
Division 3: Cerebrocerebellum / Pontocerebellum (Neocerebellum)
| Feature | Details |
|---|---|
| Anatomic region | Lateral hemispheres of posterior lobe |
| Evolutionary age | Newest, most developed in humans (neocerebellum) |
| Major inputs | Corticopontine fibers → pontine nuclei → middle cerebellar peduncle |
| Deep nucleus | Dentate nucleus (largest deep cerebellar nucleus) |
| Outputs | Dentate → contralateral ventral lateral (VL) thalamus → motor + premotor cortex; also to contralateral red nucleus |
| Functions | Motor planning and programming (before movement starts); procedural memory; fine, skilled distal movements; coordination of speech (explaining this boy's dysarthria) |
| Dysfunction | Poor motor planning, scanning (ataxic) dysarthria, decomposition of movement, dysdiadochokinesia |
Functional Divisions Summary Table
| Division | Old Name | Anatomy | Deep Nucleus | Main Function | Dysfunction |
|---|---|---|---|---|---|
| Vestibulocerebellum | Archicerebellum | Flocculonodular lobe | Vestibular nuclei | Balance, eye movement | Truncal ataxia, nystagmus |
| Spinocerebellum | Paleocerebellum | Vermis + intermediate | Fastigial, Interposed | Limb + postural coordination | Limb ataxia, hypotonia |
| Cerebrocerebellum | Neocerebellum | Lateral hemispheres | Dentate | Motor planning, speech | Dysarthria, dysdiadochokinesia |
Connecting Back to This Patient
- Unstable gait (ataxia) - primarily vestibulocerebellum and spinocerebellum dysfunction
- Difficulty with speech (dysarthria) - primarily cerebrocerebellum (dentate nucleus) involvement
- Both features together point to diffuse or midline cerebellar dysfunction
60-year-old male is suffering from difficulty in initiation of any motor activity. While sitting he is having tremor in his hand which stops during any activity. Doctors also noted, along with change of emotions, there is no change in facial expression. i. What is your probable diagnosis? ii. Explain the pathophysiology of the disease with a diagram. iii.explain the physiological basis of hyperkinesia iv. Name two drugs used to reduce hypokinesia in this patient. v. What type of rigidity is seen in this patient and how does it differ from the rigidity upper motor neuron lesion
Clinical Case: Parkinson's Disease in a 60-Year-Old Male
i) Probable Diagnosis
| Feature in Case | Parkinsonian Sign |
|---|---|
| Difficulty initiating motor activity | Akinesia / Bradykinesia (hypokinesia) |
| Tremor at rest that disappears during activity | Resting (pill-rolling) tremor - 4-6 Hz (or 8 Hz alternating) |
| No change in facial expression | Hypomimia / Mask-like facies (amimia) |
| Emotional changes without facial expression change | Autonomic/emotional dysfunction with rigidity affecting facial muscles |
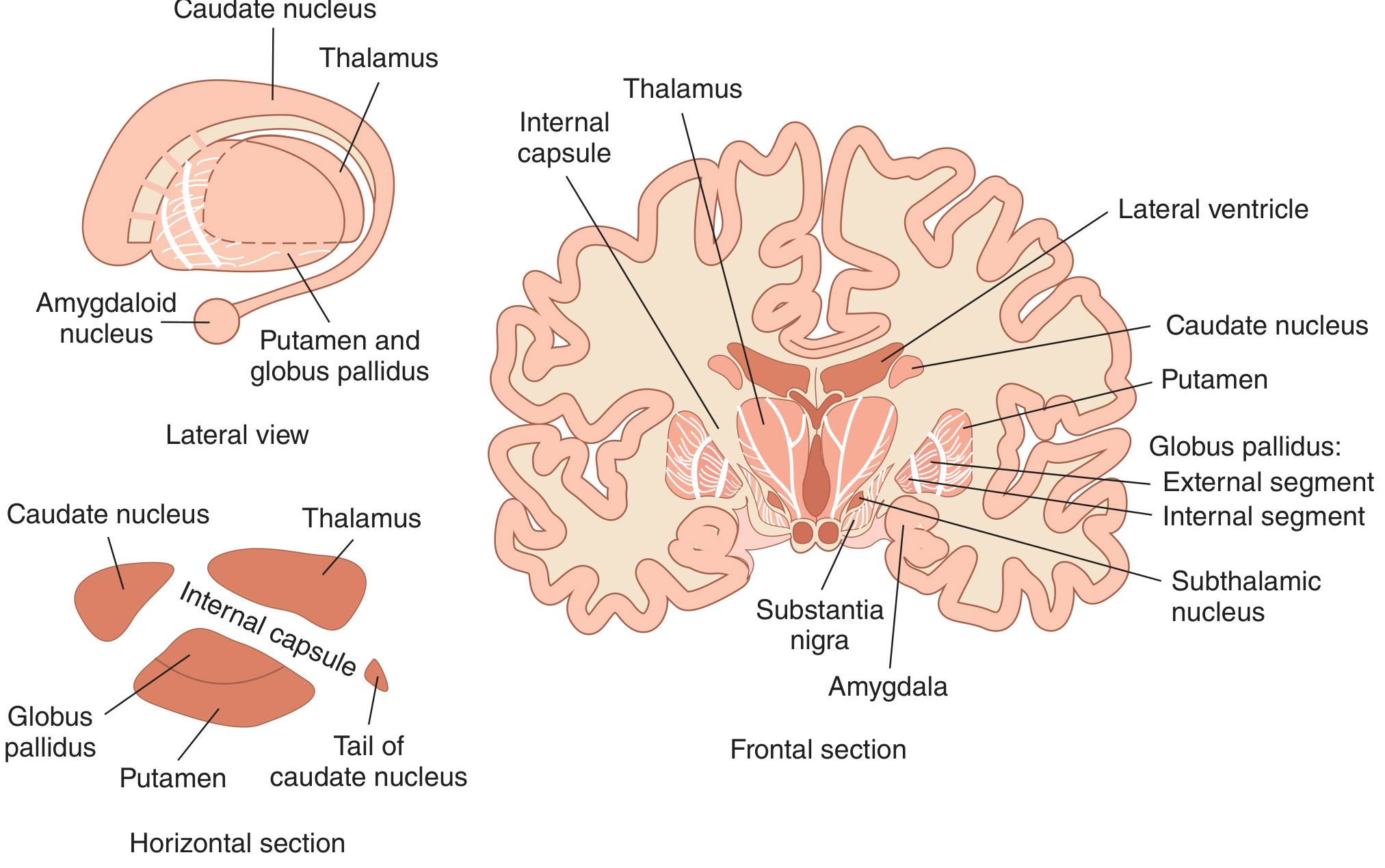
ii) Pathophysiology of Parkinson's Disease
Anatomy of the Basal Ganglia
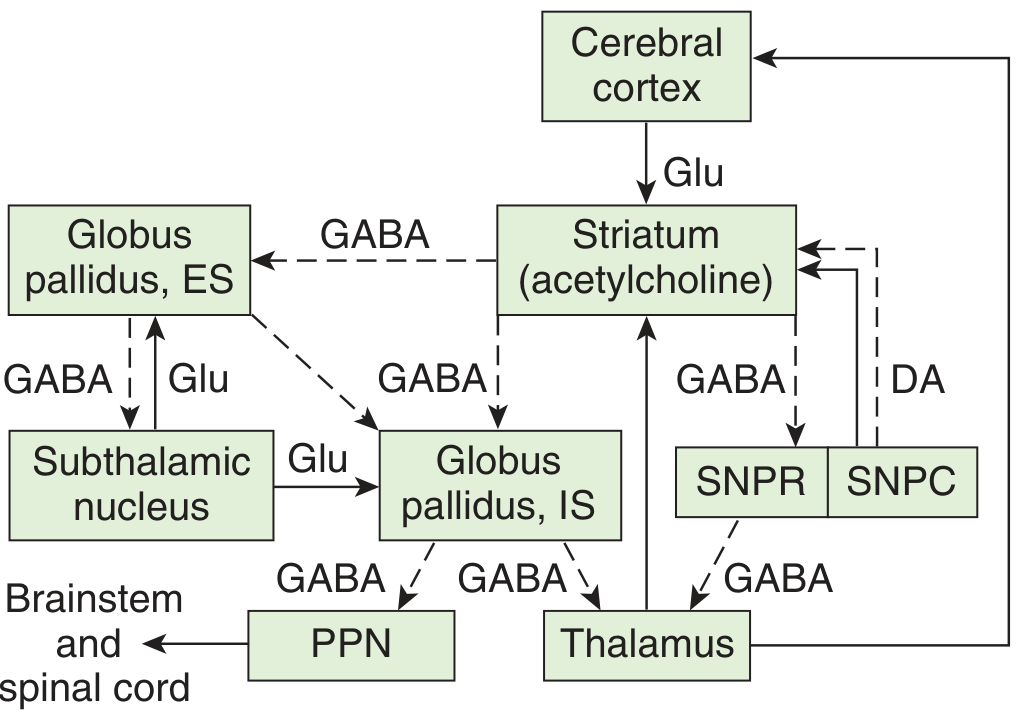
Normal Basal Ganglia Circuit
Cortex (Glu+) → Striatum (D1 receptors)
→ Inhibits GPi (GABA-)
→ GPi inhibition REDUCED → Thalamus disinhibited
→ Thalamus (Glu+) → Motor Cortex ACTIVATED → MOVEMENT
Cortex (Glu+) → Striatum (D2 receptors)
→ Inhibits GPe (GABA-)
→ GPe inhibition REDUCED → STN activated
→ STN (Glu+) → Activates GPi
→ GPi (GABA-) → Inhibits Thalamus
→ Motor Cortex SUPPRESSED → LESS MOVEMENT
- D1 receptors on direct pathway neurons → Dopamine excites → more movement
- D2 receptors on indirect pathway neurons → Dopamine inhibits → less suppression → more movement
- Net effect: dopamine facilitates movement through both pathways
Pathophysiology in Parkinson's Disease
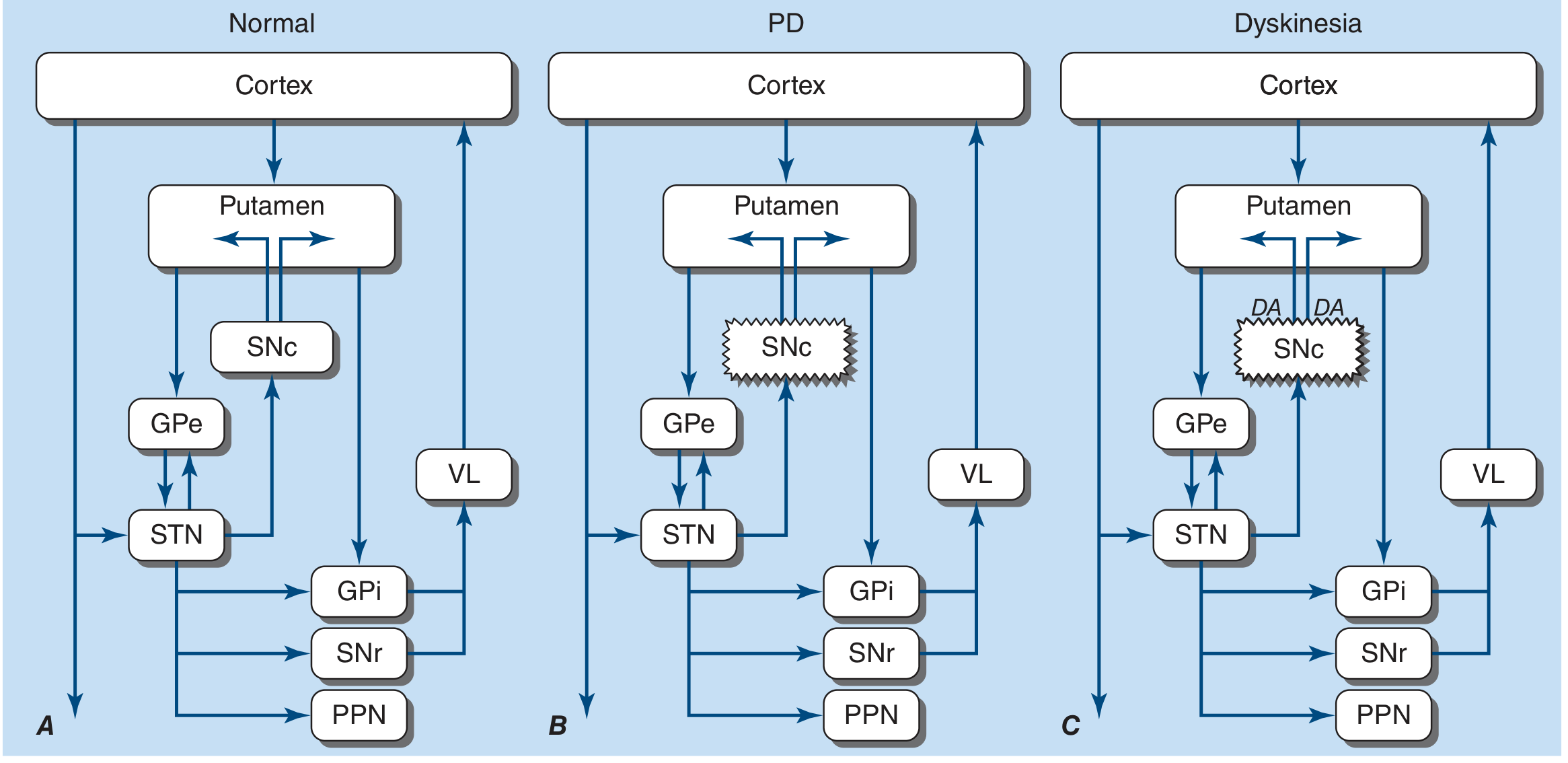
- Direct pathway LESS active → GPi NOT inhibited → GPi remains tonically overactive → Thalamus over-inhibited → Motor cortex under-activated
- Indirect pathway MORE active → GPe MORE inhibited → STN disinhibited and overactive → STN over-stimulates GPi → GPi even MORE overactive → Thalamus even more inhibited
- Excessive GPi/SNr output → Thalamus excessively inhibited → Motor cortex under-activated
- Clinical manifestation: Akinesia, bradykinesia, difficulty initiating movement (hypokinesia)
Step-by-Step Summary Table
| Step | Normal | In Parkinson's Disease |
|---|---|---|
| SNc dopamine output | Normal | Reduced (degenerated neurons) |
| Direct pathway activity | Balanced | Reduced (D1 not stimulated) |
| Indirect pathway activity | Balanced | Increased (D2 not inhibited) |
| GPi/SNr output | Balanced | Overactive (excessive GABA output) |
| Thalamus activity | Moderately active | Excessively inhibited |
| Motor cortex activation | Normal | Reduced |
| Clinical result | Smooth movement | Akinesia / Bradykinesia |
"Dopamine denervation leads to increased firing of neurons in the STN and GPi, excessive inhibition of the thalamus, reduced activation of cortical motor systems, and the development of parkinsonian features."
- Harrison's Principles of Internal Medicine, 22nd Ed.
iii) Physiological Basis of Hyperkinesia in Parkinson's Disease
Normal Balance
In Parkinson's Disease
- Nigrostriatal dopaminergic system
- Intrastriatal cholinergic system
- GABAergic system (striatum → globus pallidus and substantia nigra)
Resting Tremor (Hyperkinetic Feature)
- Caused by rhythmic, alternating 8-Hz contractions of antagonist muscles
- Due to uncoordinated oscillating activity in the basal ganglia - thalamo-cortical loop in the absence of dopaminergic stabilisation
- Tremor is present at rest (when the motor cortex is not actively driving the muscles)
- Disappears with voluntary movement because cortical activation temporarily overrides the oscillating basal ganglia circuit
- This is called "tremor at rest" or "pill-rolling tremor" - the classic feature in this patient
Why it stops with movement
iv) Two Drugs Used to Reduce Hypokinesia
1. Levodopa (L-DOPA) + Carbidopa (Sinemet)
- Mechanism: Levodopa is a precursor to dopamine; it crosses the blood-brain barrier (dopamine itself cannot) and is decarboxylated to dopamine in the brain, replenishing dopamine in the striatum
- Carbidopa inhibits peripheral DOPA decarboxylase, preventing conversion of L-DOPA to dopamine outside the brain - increases CNS delivery and reduces peripheral side effects (nausea, cardiac effects)
- Most effective drug for hypokinesia and bradykinesia in PD
- First drug identified for treating a specific neurotransmitter deficiency
2. Dopamine Agonists (e.g., Pramipexole, Ropinirole, Bromocriptine)
- Mechanism: Directly stimulate dopamine receptors (D1 and D2) in the striatum, bypassing the need for dopamine synthesis by degenerated SNc neurons
- Used as monotherapy (especially in younger patients to delay levodopa complications) or in combination with levodopa
- Also include apomorphine (rapid-acting injectable dopamine agonist)
Additional drug classes used: MAO-B inhibitors (selegiline, rasagiline - prevent dopamine breakdown), COMT inhibitors (entacapone - block L-DOPA breakdown, allowing more to reach brain), Amantadine (increases dopamine release).
v) Type of Rigidity in Parkinson's Disease vs UMN Rigidity
Rigidity in Parkinson's Disease
| Feature | Description |
|---|---|
| Lead-pipe rigidity | Uniform, plastic, "dead-feeling" resistance throughout the entire range of passive movement - like bending a lead pipe - affects BOTH agonist and antagonist muscles equally |
| Cogwheel rigidity | A series of rhythmic "catches" or ratchet-like interruptions during passive movement - caused by the superimposition of resting tremor on the lead-pipe rigidity |
"The rigidity is different from spasticity because motor neuron discharge increases to both the agonist and antagonist muscles. Passive motion of an extremity meets with a plastic, dead-feeling resistance... called lead pipe rigidity. Sometimes a series of 'catches' takes place during passive motion (cogwheel rigidity), but the sudden loss of resistance seen in a spastic extremity is absent."
- Ganong's Review of Medical Physiology, 26th Ed.
- Loss of dopamine → increased GPi output → thalamic inhibition → loss of descending cortical inhibition of spinal stretch reflexes
- Also: dopamine-acetylcholine imbalance → hyperexcitability of spinal interneurons
- Both alpha and gamma motor neurons are overactive → tone increased in ALL muscle groups
Rigidity in UMN Lesion (Spasticity)
| Feature | Description |
|---|---|
| Character | Velocity-dependent resistance - resistance increases with speed of passive stretch |
| Distribution | Affects predominantly anti-gravity muscles (flexors in upper limb, extensors in lower limb) |
| Clasp-knife phenomenon | Initial strong resistance, then sudden collapse of resistance (like a penknife closing) - due to activation of Golgi tendon organs (Ib inhibition) |
Comparison Table: Parkinson's Rigidity vs UMN (Spastic) Rigidity
| Feature | Parkinson's Rigidity (Cogwheel/Lead-pipe) | UMN Rigidity (Spasticity) |
|---|---|---|
| Cause | Loss of dopamine in basal ganglia (SNc degeneration) | Damage to corticospinal tract and descending inhibitory pathways |
| Mechanism | Alpha + gamma motor neurons both hyperactive; dopamine-ACh imbalance | Loss of descending inhibition → gamma motor neuron disinhibition → hyperactive stretch reflex |
| Character | Uniform (plastic), "lead-pipe" feel; cogwheel catches if tremor present | Velocity-dependent; "clasp-knife" - resistance then sudden release |
| Muscles affected | Both agonist AND antagonist equally | Predominantly anti-gravity muscles (flexors in arm, extensors in leg) |
| Clasp-knife phenomenon | ABSENT | PRESENT |
| Associated tremor | Yes - resting tremor (4-8 Hz) | No resting tremor; clonus may be present |
| Tendon reflexes | Normal or mildly increased | Markedly exaggerated (hyperreflexia) |
| Plantar response | Normal (flexor) | Extensor (Babinski sign) |
| Weakness | Present (difficulty initiating movement) | Present (contralateral hemiplegia) |
| Distribution | Bilateral (usually asymmetric at onset) | Contralateral to brain lesion (hemiplegia) |
| Associated features | Mask face, micrographia, festinant gait, hyposmia | Hyperreflexia, Babinski, exaggerated jerks |
Summary - Key Distinction
Parkinson's rigidity = plastic, uniform, lead-pipe + cogwheel quality; both agonist and antagonist equally stiff; NO clasp-knife; tremor at rest disappears with movement.
UMN spasticity = velocity-dependent, clasp-knife quality; anti-gravity muscles predominantly; WITH exaggerated reflexes and Babinski sign; tremor absent.