Screening guidelines for lung cancer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information to provide a thorough answer on lung cancer screening guidelines.
Lung Cancer Screening Guidelines
Why Screen for Lung Cancer?
Lung cancer kills more people than prostate, breast, and colon cancer combined. About 75% of cases are diagnosed at an advanced stage, where 5-year survival is only 6–30%, compared to ~60% for localized disease. Screening aims to detect disease early enough for curative surgical resection.
Neither chest radiography nor sputum cytology has been shown to reduce lung cancer mortality — they are not recommended for screening.
Evidence Base
National Lung Screening Trial (NLST)
- 53,454 participants, 33 US centers
- Ages 55–74, ≥30 pack-year smoking history, former smokers quit within 15 years
- 3 annual rounds of low-dose CT (LDCT) vs. chest X-ray
- Result: 20% reduction in lung cancer mortality and 6.7% reduction in all-cause mortality
- Number needed to screen to prevent one lung cancer death: 320
NELSON Trial (Dutch-Belgian)
- Men and women ages 50–75, current or former smokers who quit within 10 years, ≥15 pack-years
- LDCT at baseline, then 1, 3, and 5.5 years vs. usual care
- At 10-year follow-up: 24% reduction in lung cancer mortality (rate ratio 0.76)
- Greater benefit seen in women
Both trials provide definitive evidence that LDCT screening reduces mortality in high-risk individuals.
Current Eligibility Criteria
USPSTF (2021 update) — Grade B recommendation:
- Age 50–80 years
- ≥20 pack-year smoking history
- Currently smoking or quit within the past 15 years
(Note: Earlier USPSTF criteria, which some sources still reference, used age 55–80 and ≥30 pack-years; the 2021 update expanded the eligible population.)
Discontinuation criteria:
- Has not smoked for ≥15 years, or
- Develops a health problem that substantially limits life expectancy or the willingness/ability to undergo curative surgery
CMS (Medicare) eligibility:
- Age 55–77
- ≥30 pack-years, current or former smoker who quit within 15 years
- Must have a shared decision-making (SDM) counseling visit before the first LDCT
NCCN also recommends screening for:
- Age ≥50, ≥20 pack-years, plus one additional risk factor (e.g., occupational exposure, radon, family history) raising 6-year lung cancer risk to ≥1.3%
Patient Eligibility Algorithm
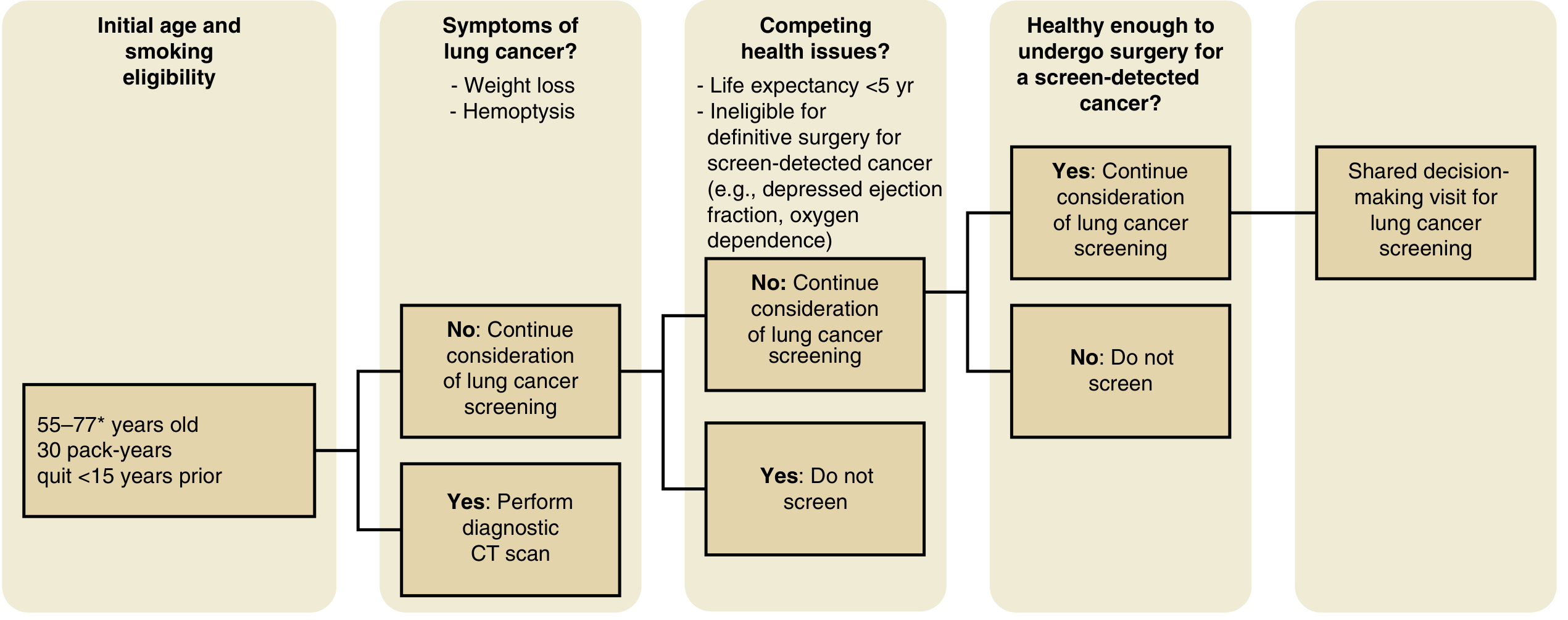
Figure: Algorithm for considering patient eligibility for lung cancer screening (Murray & Nadel's Textbook of Respiratory Medicine)
Key decision points:
- Meets age and smoking eligibility criteria
- No symptoms suggestive of lung cancer (weight loss, hemoptysis) — if symptomatic, proceed to diagnostic CT, not screening
- No competing health issues (life expectancy <5 yr, ineligible for surgery due to depressed EF, O₂ dependence)
- Able and willing to undergo surgery if cancer is found
- Proceed to shared decision-making visit
Modality: Low-Dose CT (LDCT)
- Radiation dose: ~8 mSv (vs. ~32 mSv for standard CT)
- Performed annually
- Reported using the Lung-RADS structured reporting system (ACR)
Nodule Management (Lung-RADS Framework)
| Finding | Management |
|---|---|
| Clearly benign (calcified, subpleural lymph node) | No further surveillance |
| Solid nodule ≤8 mm | Serial CT (interval based on size) |
| Pure ground-glass nodule | Monitor until solid component appears |
| Partly solid nodule | Manage based on solid component size |
| Solid nodule >8 mm | Risk stratify; PET, biopsy, or resection based on malignancy probability |
Most nodules found on screening are benign. The key challenge is minimizing unnecessary invasive procedures for benign findings while rapidly identifying malignant ones.
Harms of Screening
- False positives: majority of detected nodules are benign; risk of unnecessary biopsies/surgeries
- Overdiagnosis: especially subsolid nodules (pure ground-glass and partly solid), which may represent cancers that would never have become clinically significant
- Radiation exposure from serial annual CT scans
- Psychological distress from indeterminate findings
Shared Decision-Making
CMS mandates a formal SDM visit before the first screening LDCT for Medicare patients. The visit should cover:
- Benefits and harms of screening
- The meaning of positive and negative results
- Follow-up procedures for positive findings
- Use of decision aids (printed or video-based)
- Smoking cessation counseling for active smokers
Smoking Cessation
Smoking cessation reduces lung cancer mortality more effectively than screening alone. In the NLST, 7 years of abstinence achieved the same 20% mortality reduction as LDCT. Combining cessation with LDCT achieved a 38% mortality reduction. Cessation counseling must be integrated into any screening program.
Sources: Murray & Nadel's Textbook of Respiratory Medicine, pp. 1695–1702; The Washington Manual of Medical Therapeutics, p. 318; Fishman's Pulmonary Diseases and Disorders
This is a shared conversation. Sign in to Orris to start your own chat.