Fluid Replacement in Dengue
Reading File
Finding Sources
Finding Sources
Searching PubMed
"dengue" AND "fluid resuscitation"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a comprehensive, well-illustrated answer. Here is the full response:
Fluid Replacement in Dengue
Dengue fluid management is driven by disease severity. The plasma leakage phase (days 3-7 of illness) is the most dangerous window, and fluid therapy must be calibrated to the grade of disease. Haematocrit and vital signs are the primary guides throughout.
WHO Grading - Quick Reference
| Grade | Classification | Key Feature |
|---|---|---|
| DF | Dengue Fever | No plasma leakage; Hct rise 5-10% |
| DHF I | Mild DHF | Hct rise ≥20%, platelet <100,000; positive tourniquet test |
| DHF II | Moderate DHF | Above + spontaneous bleeding |
| DHF III | Compensated Shock | Pulse pressure ≤20 mmHg, weak rapid pulse, cold clammy extremities |
| DHF IV | Profound Shock | Undetectable BP/pulse (Dengue Shock Syndrome) |
1. Dengue Fever (DF) - Outpatient Oral Therapy
Patients tolerating oral fluids with urine output at least once every 6 hours and no warning signs can be managed at home:
- Oral rehydration solution (ORS), fruit juices, and electrolyte-containing fluids - preferred over plain water, as plain water does not replace electrolytes lost from fever and vomiting
- Caution: Glucose-containing fluids may exacerbate hyperglycaemia in diabetics and during physiological stress
- Paracetamol for fever; dose interval not less than 6 hours. Tepid sponging for persistent high fever
- Avoid aspirin, ibuprofen, and all NSAIDs - they aggravate gastritis, bleeding, and aspirin may precipitate Reye's syndrome
- IV fluids indicated only if persistent vomiting or refusal to feed
Return immediately if: no improvement, abdominal pain, persistent vomiting, black tarry stools, cold extremities, lethargy, or no urine for >4-6 hours.
2. DHF Grades I & II - IV Fluid Algorithm
Haemoconcentration (Hct rise ≥20%) with thrombocytopenia is the trigger for IV therapy.
Starting point: IV crystalloid at 6 ml/kg/h for 1-2 hours, then check Hct.
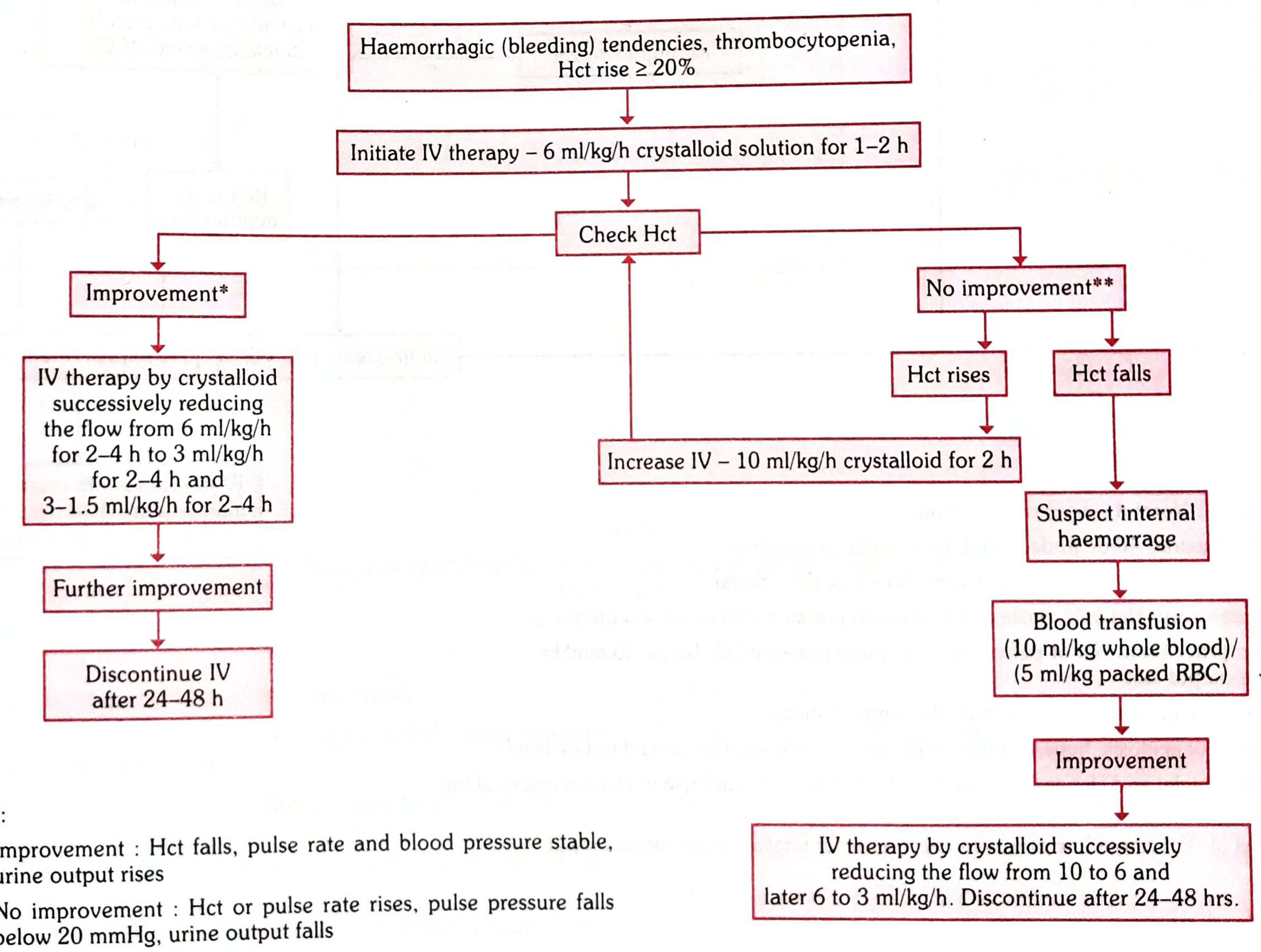
If improvement (Hct falls, pulse and BP stable, urine output rises):
- Reduce IV crystalloid stepwise: 6 ml/kg/h → 3 ml/kg/h (2-4 h) → 1.5 ml/kg/h (2-4 h)
- Discontinue IV after 24-48 hours
If no improvement - Hct rises:
- Increase to 10 ml/kg/h crystalloid for 2 hours, reassess
If no improvement - Hct falls (suspect internal haemorrhage):
- Blood transfusion: 10 ml/kg whole blood or 5 ml/kg packed RBCs
- After improvement: step down to 10 → 6 → 3 ml/kg/h, discontinue after 24-48 h
3. DHF Grade III (Compensated Shock) - IV Fluid Algorithm
Trigger: Pulse pressure ≤20 mmHg, SBP <90 mmHg, Hct rise >20% from baseline.
Starting point: IV crystalloid at 10-20 ml/kg/h for 1 hour, then assess vital signs (VS) and Hct.
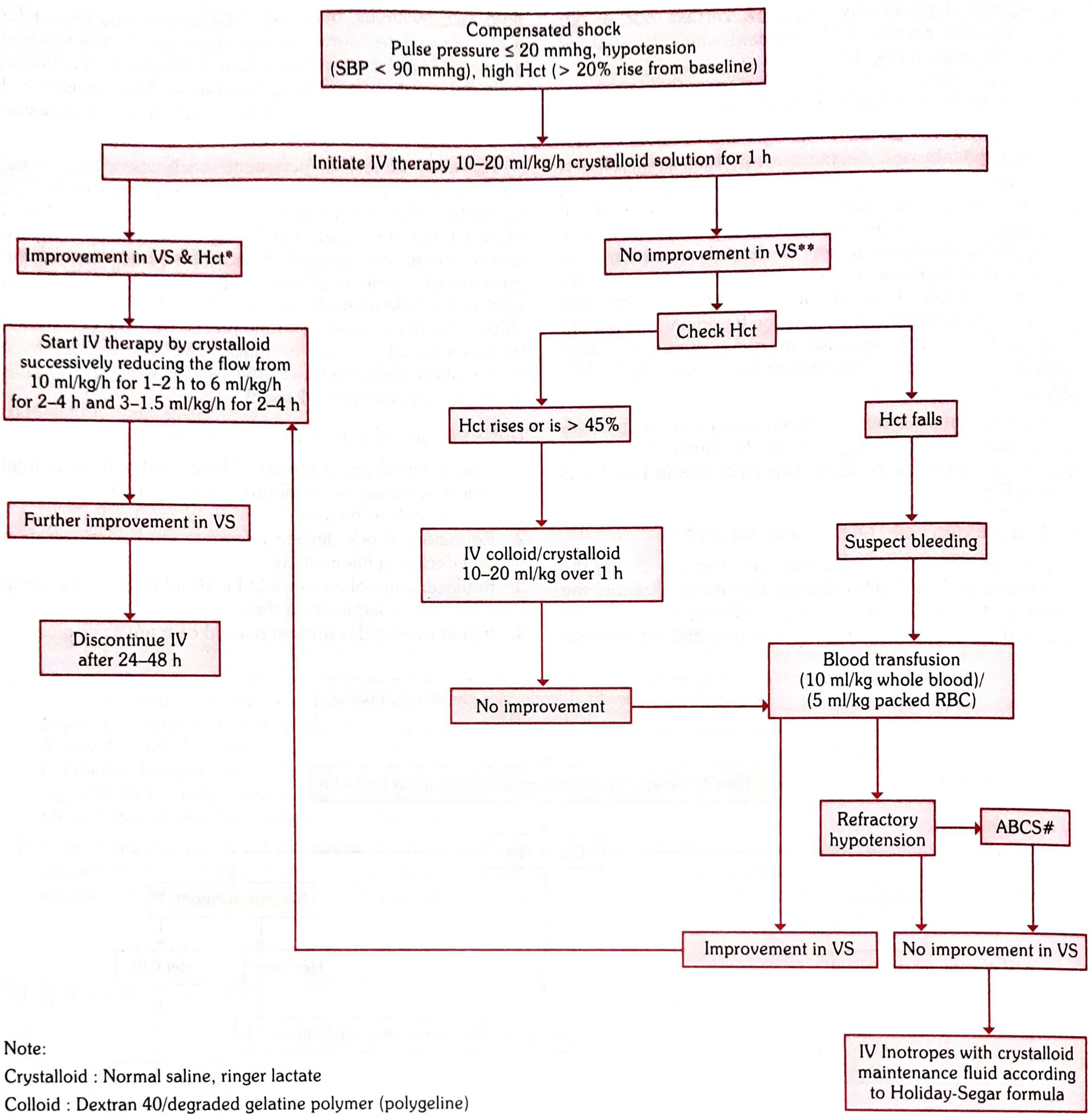
If improvement in VS and Hct:
- Step down: 10 ml/kg/h → 6 ml/kg/h (2-4 h) → 1.5 ml/kg/h (2-4 h)
- Discontinue IV after 24-48 hours
If no improvement - Hct rises or stays >45%:
- Give IV colloid OR crystalloid 10-20 ml/kg over 1 hour
- Colloids used: Dextran 40 or degraded gelatine polymer (polygeline)
If no improvement - Hct falls (suspect bleeding):
- Blood transfusion: 10 ml/kg whole blood or 5 ml/kg packed RBCs
- If still refractory hypotension → check ABCS (Acidosis, Bleeding, Calcium/electrolytes, Sugar)
- If VS still not improving → IV inotropes with crystalloid maintenance by Holliday-Segar formula
4. DHF Grade IV (Profound Shock / DSS)
- Same algorithm as Grade III but shock is more profound (undetectable BP/pulse)
- Oxygen to all patients in shock - mandatory
- IV crystalloid resuscitation initiated immediately on hospitalization
- If already received ~1000 ml IV fluid and no improvement: switch to colloidal solution (Dextran 40/haemaccel) or, if Hct is declining, fresh whole blood 10-20 ml/kg/h
- For persistent shock with declining Hct despite colloid - suspect internal bleeding; give fresh whole blood 10 ml/kg/h routinely as a precaution
5. Indications for Red Cell Transfusion
- Overt blood loss ≥10% of total blood volume - give whole blood or components
- Refractory shock despite adequate IV fluids with declining Hct
- Replacement volume: 10 ml/kg body weight at a time; obtain coagulogram first
- If fluid overload is present: use packed cells instead of whole blood
6. Types of IV Fluid - What to Use
| Type | Examples | When to Use |
|---|---|---|
| Crystalloid | Normal saline (0.9% NaCl), Ringer's lactate | First-line for all grades |
| Colloid | Dextran 40, polygeline (degraded gelatine) | When crystalloid fails, Hct rising, shock persists |
| Blood/pRBC | Fresh whole blood, packed RBCs | Declining Hct + shock, overt/suspected internal bleeding |
Note: In cases of acidosis, Ringer's lactate (hyperosmolar solution) should NOT be used.
7. Monitoring Parameters
- Haematocrit: Serial monitoring every hour in shock; daily from day 3 until afebrile for 1-2 days
- Platelet count: Drop in platelets + rise in Hct = early warning for DHF
- Vital signs and urine output: Every hour in DHF grades III/IV
- Improvement defined as: Hct falls, pulse rate and BP stabilise, urine output rises
- No improvement / deterioration: Hct or pulse rate rises, pulse pressure falls below 20 mmHg, urine output falls
8. Key Principles - Summary
- Fluid therapy is entirely supportive - no specific antivirals exist for dengue
- The goal is to bridge the plasma leakage phase (typically 24-48 hours during defervescence) without causing fluid overload
- Over-resuscitation is as dangerous as under-resuscitation - fluid overload causes pulmonary oedema, particularly once plasma reabsorption begins (recovery phase)
- IV fluids should be discontinued within 24-48 hours of clinical improvement
- NSAIDs and aspirin are absolutely contraindicated in all dengue grades
- DSS patients require ICU admission
Sources: Park's Textbook of Preventive and Social Medicine, pp. 293-297; Rosen's Emergency Medicine: Concepts and Clinical Practice, p. 2630; Creasy & Resnik's Maternal-Fetal Medicine, p. 12.
Recent evidence: A 2025 systematic review (PMID: 41037858) on dengue pathogenesis, diagnosis, and management confirms the WHO-based supportive fluid approach remains standard of care with no new antivirals approved.
This is a shared conversation. Sign in to Orris to start your own chat.