


Help me out how to assess and write the positive findings
Reading File
search_medical_text
CT brain ischemic stroke findings reporting acute infarct
search_medical_image
MRI DWI FLAIR acute ischemic stroke positive findings
GradeResponse
GradeResponse
Here is a structured assessment and reporting guide for this case based on the imaging films.
Patient Details
Basanagouda Patil | 59Y/M | Date: 03-Jul-2025
Studies: NCCT Brain + MRI Brain (Stroke Protocol: DWI, FLAIR, T2, GRE/FFE, MR Angiography)
Step-by-Step Assessment Approach
1. NCCT Brain — What to Look For
| Region | Key Findings to Assess |
|---|---|
| Parenchyma | Hypodensity, loss of grey-white differentiation, cortical ribbon sign |
| Hyperdense vessel sign | Look for dense MCA/basilar (acute thrombus) |
| Cerebellum / Brainstem | Hypodensity, mass effect |
| Ventricles | Size, shift, effacement |
| Basal ganglia | Lenticular nucleus obscuration |
| Skull/Calvarium | Fracture, bony lesions |
From the NCCT images, the posterior fossa slices and supratentorial cuts need careful review. Small cortical or posterior fossa infarcts can be missed on CT.
2. MRI DWI — Critical Sequence
- Positive finding: Focal bright (hyperintense) signal on DWI = restricted diffusion = acute infarct
- Confirm with ADC map: corresponding dark (hypointense) signal confirms true restriction (not T2 shine-through)
- From the DWI panel (left half of MRI film), there appear to be areas of hyperintensity in the posterior fossa / cerebellar region on lower cuts and supratentorial white matter on mid-level cuts — these are the key positive findings
3. FLAIR — DWI-FLAIR Mismatch Rule
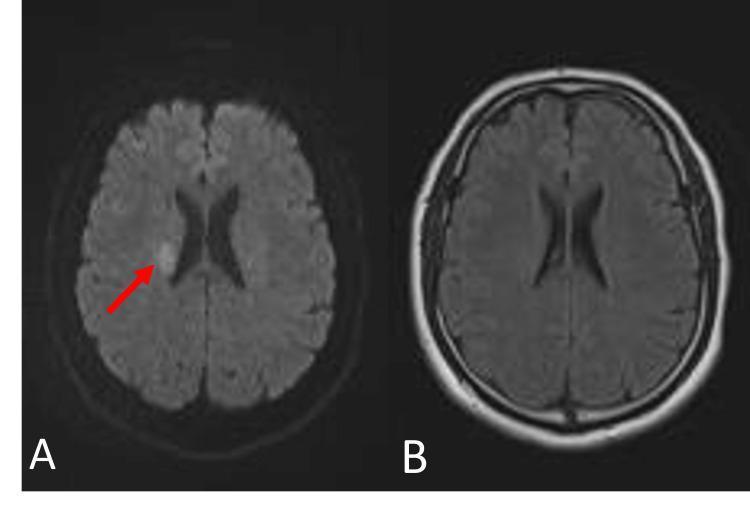
- If DWI bright but FLAIR normal → infarct is < 4.5 hours old (thrombolysis window)
- If DWI bright AND FLAIR bright → infarct is > 4.5–6 hours (established)
- The FLAIR sequence (right half of MRI film, T2W FLAIR AXIAL labeled) should be compared slice-by-slice with DWI
4. T2W / GRE (FFE) Sequences
- T2W: Bright signal in infarct territory (may lag behind DWI in hyperacute phase)
- *GRE/FFE (T2)**: Look for blooming artifact = hemorrhagic transformation or microbleeds (dark spots)
- From the GRE panel (third film, right side labeled T2W FFE/GRE), check for any dark foci
5. MR Angiography — Vessel Assessment
From the MRA panel (third film, left side):
- Normal: Both carotid systems and vertebrobasilar system show well-opacified vessels with smooth tapering
- Positive findings to report:
- Stenosis: Focal narrowing / signal dropout
- Occlusion: Abrupt cutoff of vessel
- Atherosclerotic irregularity: Irregular contour of vessel walls
- Assess: ICAs, MCAs (M1/M2), ACAs, basilar artery, vertebral arteries, PCAs
How to Write the Positive Findings Report
Template
NCCT BRAIN:
- Hypo/isodense area noted in [location] suggestive of [acute/subacute] infarct
/ No significant hypodensity / No intracranial hemorrhage
- Hyperdense MCA sign: Present / Absent
- Midline shift: Present [X mm to left/right] / Absent
- Ventricles: Normal / Dilated / Effaced
- Posterior fossa: Normal / Hypodensity in [cerebellum/brainstem]
MRI BRAIN — STROKE PROTOCOL:
DWI/ADC:
- Focal area of restricted diffusion (DWI bright, ADC dark) noted in [location — e.g.,
left MCA territory / right cerebellar hemisphere / right internal capsule]
measuring approximately [X × Y cm], consistent with ACUTE INFARCT.
FLAIR:
- Corresponding FLAIR [hyperintensity / no signal change] at the above-described site,
suggesting infarct age [>4.5 hrs if FLAIR positive / <4.5 hrs if FLAIR negative —
DWI-FLAIR mismatch].
T2W:
- [T2 hyperintensity / no signal change] in the infarcted territory.
GRE/T2*:
- No blooming artifact to suggest hemorrhagic transformation / microbleeds.
[OR: Foci of blooming artifact noted in [location] — hemorrhagic transformation /
microbleeds cannot be excluded.]
MR ANGIOGRAPHY (Intracranial + Neck vessels):
- [Normal flow signal in bilateral ICAs, MCAs, ACAs, PCAs, vertebral arteries,
and basilar artery]
[OR: Focal signal dropout / stenosis / occlusion noted at [location].]
- Carotid bifurcation: Normal / Atherosclerotic changes with [mild/moderate/severe] stenosis
- Vertebral arteries: Symmetrical / Dominant right/left / Hypoplastic [side]
IMPRESSION:
1. Acute ischemic infarct in [territory/location] — [size if measurable]
2. DWI-FLAIR mismatch [present/absent] — [thrombolysis window open/closed]
3. [MRA findings — occlusion/stenosis if present, or normal intracranial vasculature]
4. No intracranial hemorrhage / hemorrhagic transformation
Key Teaching Points for This Case
- Stroke protocol MRI is far superior to CT for acute infarct detection — especially posterior fossa (where CT has bone artifact)
- Always correlate DWI ↔ ADC ↔ FLAIR for confirmation and timing
- MRA without contrast (Time of Flight) is sufficient to assess large vessel occlusion (LVO) — the key treatable target
- Report territory (MCA/PCA/ACA/PICA/basilar), side, and approximate size
- GRE/FFE is the sequence to exclude hemorrhage before thrombolysis decisions
This is a shared conversation. Sign in to Orris to start your own chat.