Pelvic drop
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I have comprehensive information from multiple textbooks. Here is a thorough answer:
Pelvic Drop
Definition
Pelvic drop (also called contralateral pelvic drop) is the inferior displacement of the pelvis on the non-stance (swing) side during single-leg stance or walking. It results from failure of the hip abductor muscles on the stance leg to generate sufficient moment to keep the pelvis level. This is the motion seen during Trendelenburg gait.
- Firestein & Kelley's Textbook of Rheumatology, Statics
- Imaging Anatomy Vol. 3, Function of the Pelvis
Biomechanical Basis
During single-limb stance, the ground reaction force passes medial to the hip joint, creating an external hip adduction moment (clockwise rotation of the pelvis). To counterbalance this, the stance-side hip abductors must generate an internal hip abduction moment (counterclockwise).
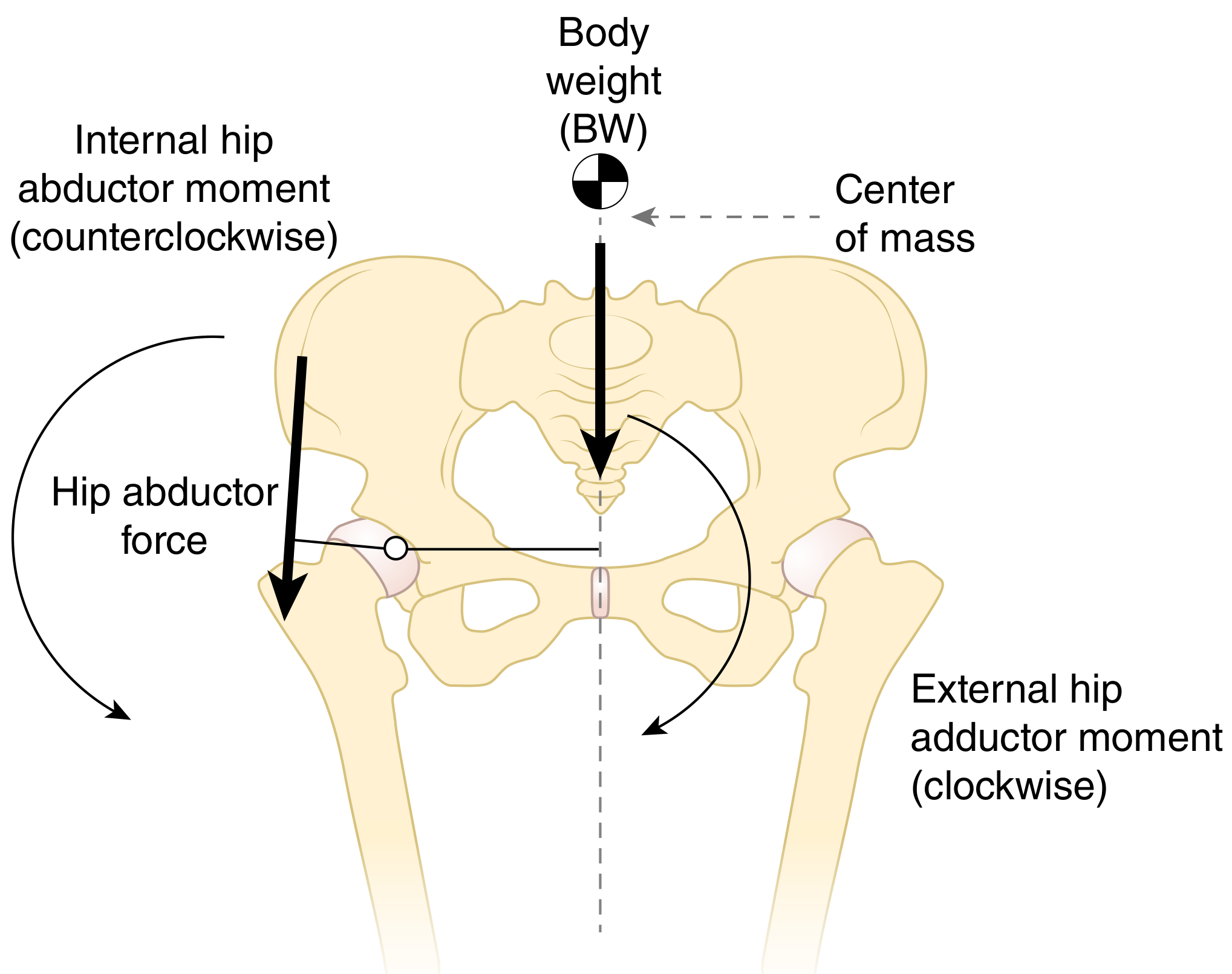
If the abductors fail to generate an adequate counterbalancing moment, the contralateral side of the pelvis drops - this is pelvic drop. The magnitude of the required abductor force depends on the moment arm of the abductor muscles:
-
A shorter moment arm (e.g., coxa valga, reduced femoral offset) demands a greater muscle force for the same stabilizing moment.
-
This increases joint contact force and articular stress.
-
Firestein & Kelley's Textbook of Rheumatology, p. Statics section
Muscles Responsible
The primary muscles preventing pelvic drop are the hip abductors of the stance leg:
| Muscle | Innervation | Function |
|---|---|---|
| Gluteus medius | Superior gluteal nerve (L4, L5, S1) | Primary hip abductor; holds pelvis over stance leg; prevents contralateral pelvic drop |
| Gluteus minimus | Superior gluteal nerve (L4, L5, S1) | Assists abduction; same stabilizing role |
During midstance, the gluteus medius acts eccentrically to control pelvic tilt.
- Gray's Anatomy for Students, Table 6.2
- Miller's Review of Orthopaedics, Table 10.1
Normal vs. Abnormal Pelvic Motion in Gait
In normal walking, the pelvis moves in all three planes. Frontal-plane motion (pelvic drop and pelvic hike) has a total excursion of approximately 6-10 degrees at preferred walking speed. This controlled, small-amplitude drop is a normal determinant of gait that helps minimize vertical center-of-mass displacement.
Pathological pelvic drop occurs when this motion becomes excessive due to abductor weakness.
- Imaging Anatomy Vol. 3, p. 236
Trendelenburg Sign and Gait
Trendelenburg's sign is the clinical test for hip abductor weakness:
-
The patient stands on the affected limb (the one with weak abductors).
-
Positive sign: the pelvis drops markedly on the swing (unaffected) side.
-
In gait, the patient compensates by lurching the trunk toward the affected (stance) side - this is the Trendelenburg lurch (gluteus medius lurch). By shifting the body's center of gravity over the hip, the external adduction moment is reduced, decreasing the abductor force required.
-
Gray's Anatomy for Students, Trendelenburg's sign
Causes of Pelvic Drop / Positive Trendelenburg Sign
| Cause | Mechanism |
|---|---|
| Superior gluteal nerve damage | Direct denervation of gluteus medius and minimus |
| Pelvic fractures | Nerve injury in greater sciatic foramen |
| Hip surgery (THR, etc.) | Disruption of gluteus medius/minimus tendon insertions on greater trochanter |
| Abductor tendon tears | Direct muscle-tendon unit failure |
| Hip dislocation (congenital) | Altered bony geometry, shortened abductor moment arm |
| Neuromuscular disease (e.g., post-polio) | Global lower motor neuron weakness |
| Coxa valga | Reduced abductor moment arm, insufficient moment generation |
Bilateral weakness produces a waddling gait (bilateral positive Trendelenburg).
- Gray's Anatomy for Students; Miller's Review of Orthopaedics; Campbell's Operative Orthopaedics
Clinical Relevance
- Gait analysis: Pelvic drop is classified as a midstance gait abnormality. Miller's Review lists it under pathological gait with causes of either contralateral or bilateral gluteus medius weakness.
- Hip arthroplasty: Reduced femoral offset post-THR shortens the abductor moment arm, increasing joint reaction force and risk of a Trendelenburg sign/gluteus medius lurch - a known complication requiring appropriate component sizing.
- Running injuries: Excessive contralateral pelvic drop during running is associated with iliotibial band syndrome, patellofemoral pain, and hip stress fractures due to altered lower-limb mechanics.
- Rehabilitation: Strengthening the gluteus medius (hip abductor) is the cornerstone of treatment - exercises include side-lying hip abduction, clamshells, single-leg stance drills, and lateral band walks.
This is a shared conversation. Sign in to Orris to start your own chat.