Pyogenic liver abscess, Amoebic liver abscess .Clinical, course, diagnosis, differential diagnosis of methods of surgical treatment. Complications of parasitic diseases of the liver. Everything in detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed to compile a comprehensive, detailed answer. Let me synthesize everything from the sources.
Liver Abscess: Pyogenic and Amoebic — Comprehensive Review
PART I — PYOGENIC LIVER ABSCESS (PLA)
Epidemiology & Pathogenesis
Pyogenic liver abscess is the most common type of visceral abscess, with an annual incidence of ~2.3 cases per 100,000 persons and a slight male predominance. Historically caused by portal pylephlebitis complicating appendicitis in young patients, the epidemiology has shifted: biliary tract disease (cholangitis, cholecystitis, malignant biliary obstruction) is now the most frequent identifiable source, followed by portal vein pyemia from enteric infections (diverticulitis, appendicitis, perforated peptic ulcer, IBD) and direct extension.
Routes of hepatic infection:
- Biliary (ascending cholangitis) — most common; via the bile duct
- Portal venous pyemia — from intra-abdominal septic foci
- Hematogenous — via hepatic artery from systemic bacteremia
- Direct extension/trauma — penetrating injury or adjacent septic focus
- Cryptogenic — ~40% of cases; no identifiable source; associated with Klebsiella pneumoniae and linked to underlying colorectal cancer (4× higher incidence; colonoscopy recommended)
Risk factors: Diabetes mellitus, immunosuppression, liver transplantation, biliary instrumentation, pre-existing hepatobiliary or pancreatic disease, proton pump inhibitor use (loss of gastric acid barrier), elderly age, atrophic gastritis.
Microbiology
Most PLAs are polymicrobial:
- Gram-negative bacilli: E. coli, Klebsiella spp., Proteus, Pseudomonas
- Gram-positive: Streptococcus spp. (particularly S. milleri/anginosus group); US studies identify streptococci as most common
- Anaerobes: Bacteroides fragilis, Fusobacterium necrophorum, anaerobic streptococci
- Special circumstances: S. aureus (children, septicemia); Candida spp. (immunocompromised); K. pneumoniae monomicrobic (cryptogenic PLA — high virulence, metastatic spread to eye/CNS)
- Biliary origin: E. coli, Klebsiella, Enterococcus; enteric origin: anaerobes predominate
Clinical Presentation
| Feature | Frequency |
|---|---|
| Fever (often spiking) | ~90% |
| Right upper quadrant pain/tenderness | 50–75% |
| Malaise, weight loss, anorexia | Common |
| Jaundice | ~50% (hyperbilirubinemia) |
| Hepatomegaly | Variable |
| Chills, nausea | Common |
In the preantibiotic era, presentation was acute with spiking fevers, RUQ pain, and shock. Today the presentation is more subacute, with vague symptoms for weeks before diagnosis.
Laboratory findings:
- Leukocytosis: ~90%
- Elevated alkaline phosphatase: ~80%
- Hyperbilirubinemia: ~50%
- Transaminitis: ~50%
- Hypoalbuminemia, normochromic normocytic anemia
- Blood cultures positive in ~50% of cases
Diagnosis
Imaging is the cornerstone:
- CT with IV contrast — most sensitive (~95%); shows hypoattenuated lesion with peripheral rim enhancement; identifies loculations, communicating biliary pathology, and extrahepatic disease. First-line imaging of choice.
- Ultrasound — sensitivity ~85–90%; preferred initial modality in pediatrics; guides percutaneous drainage
- Plain chest X-ray — right pleural effusion, elevated right hemidiaphragm in ~50%
- MRI — alternative; superior for cyst wall delineation; less commonly used
- Tagged WBC scan — rarely used, reserved for specific scenarios
CT showing pyogenic liver abscess with rim enhancement:
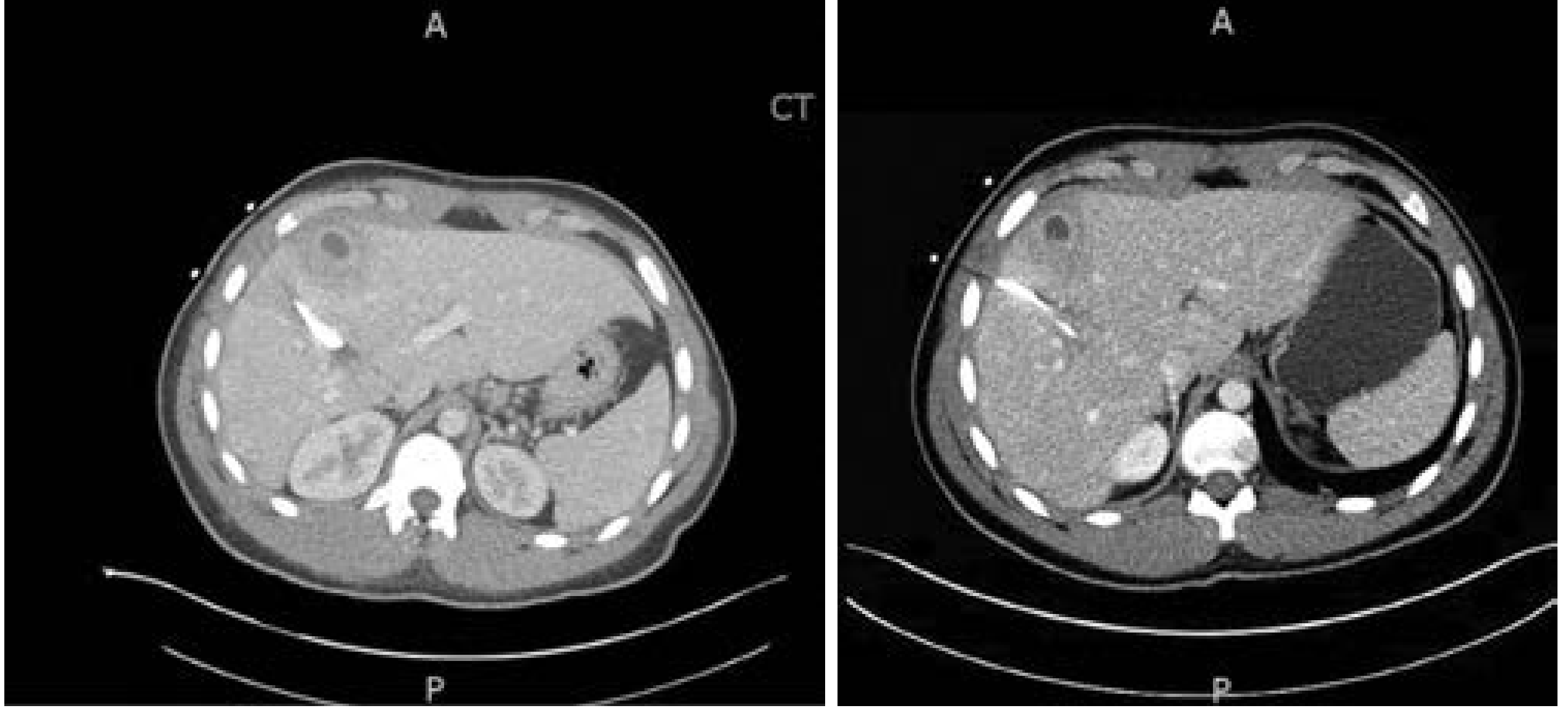
CT images showing liver abscess with peripheral rim enhancement — Current Surgical Therapy 14e
Microbiologic workup:
- Blood cultures (ideally before antibiotics)
- Image-guided aspiration with Gram stain, culture & sensitivity
- Serologic and fecal testing for E. histolytica in patients with epidemiologic risk factors
Differential Diagnosis
- Amoebic liver abscess — single, right-lobe, "anchovy paste" content; travel history; serology positive
- Hepatocellular carcinoma or metastatic liver disease (cystic/necrotic)
- Simple hepatic cyst / biloma
- Echinococcal (hydatid) cyst
- Hepatitis (acute, fulminant)
- Cholangitis
- Subphrenic or subhepatic abscess
- Pancreatic or perihepatic collections
Multiple abscesses strongly suggest pyogenic etiology; a solitary right-lobe abscess with travel history favors amoebic origin. Imaging alone cannot reliably distinguish the two — serology is essential.
Treatment
1. Antibiotics
Empiric broad-spectrum therapy covering streptococci, gram-negative bacilli, and anaerobes:
- First-line: Piperacillin/tazobactam monotherapy or ceftriaxone + metronidazole
- High-risk/biliary instrumentation/transplant: Carbapenems (for ESBL coverage)
- Duration: IV therapy for 14 days → oral completion for total 4–6 weeks, guided by clinical response and imaging resolution
2. Percutaneous Drainage (standard of care)
- Catheter placement recommended for abscesses >5 cm — superior outcomes vs. needle aspiration alone
- Safe for very large (>10 cm) abscesses (may require multiple catheters)
- Abscesses <3 cm: aspiration alone if technically feasible (guides antibiotic choice)
- Catheters remain until output is low and clear (usually ~7 days)
- Bile in drain output → suspect biliary communication → investigate with HIDA/MRCP/ERCP → may require sphincterotomy or percutaneous biliary drain
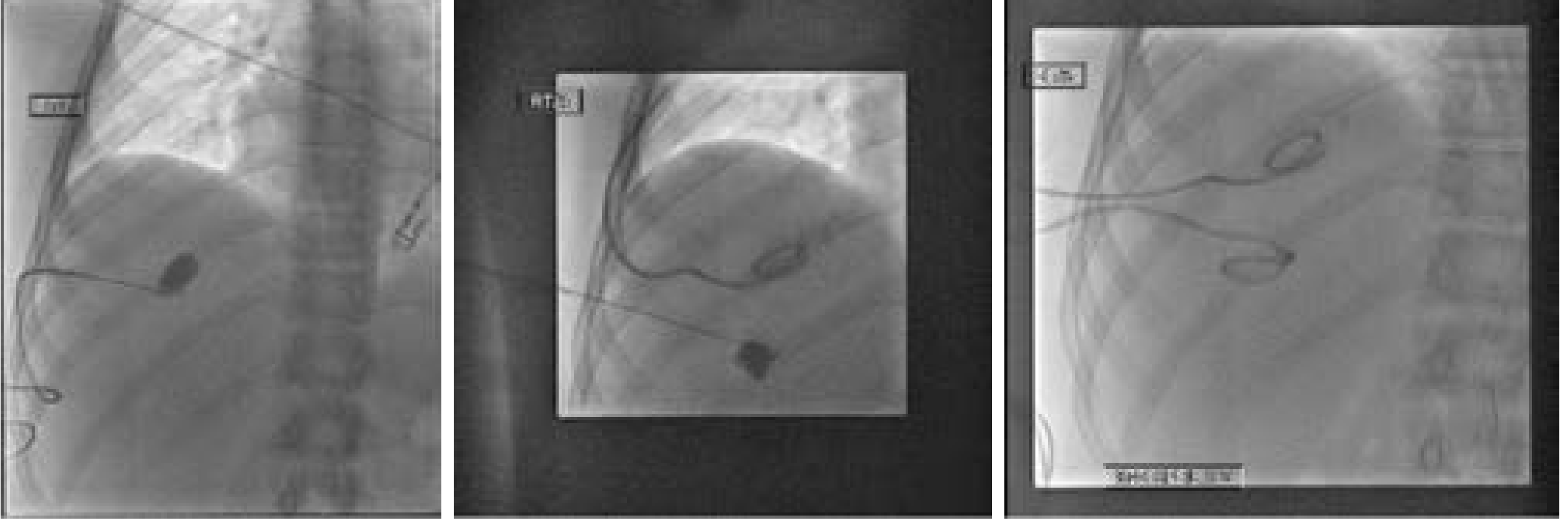
Radiographic images showing drainage catheter in place — Current Surgical Therapy 14e
3. Surgical Drainage or Resection
Indicated when:
- Percutaneous drainage fails or is incomplete
- Multiloculated abscess not amenable to catheter drainage
- Ruptured abscess with peritonitis
- Concurrent intra-abdominal pathology requiring surgery (e.g., simultaneous diverticulitis)
- Unresolved jaundice or renal impairment preventing recovery
- Biliary reconstruction needed
Approach: Minimally invasive (laparoscopic) preferred when feasible. Open laparotomy for complex cases (ruptured abscess + peritonitis, combined pathology). Surgical drainage with irrigation and drain placement is standard; partial hepatectomy (hepatic resection) has been advocated for large multiloculated abscesses failing percutaneous drainage, though no evidence it is superior to surgical drainage — and carries risk of acute septic shock from manipulation of the diseased liver.
Efficacy: antibiotics + percutaneous drainage effective in 80–90% of patients.
Outcomes & Complications
Mortality: 4–10% even with modern treatment. Worse prognosis with:
- Delayed diagnosis
- Multiple abscesses / multiple organisms in blood cultures
- Fungal etiology
- Shock, jaundice, hypoalbuminemia
- Pleural effusion, underlying biliary malignancy
- Diabetes, cirrhosis, multiorgan dysfunction
Complications of pyogenic liver abscess:
- Rupture with purulent peritonitis (abscesses >10 cm carry increased risk)
- Empyema (direct pleural extension)
- Pleural effusion (reactive or infectious)
- Pericardial effusion / rupture into pericardium (rare but life-threatening)
- Portal or splenic vein thrombosis
- Thoracoabdominal fistula
- Septic metastatic endophthalmitis — in up to 10% of diabetic patients with K. pneumoniae PLA
- Sepsis / multiorgan failure
PART II — AMOEBIC LIVER ABSCESS (ALA)
Epidemiology & Pathogenesis
ALA is the most common extraintestinal manifestation of amebiasis caused by the protozoan Entamoeba histolytica. Endemic in tropical/subtropical regions: Africa, Southeast Asia, Mexico, Venezuela, Colombia. 10% of the world's population is infected. In developed countries, cases occur in travelers and migrants from endemic areas.
Demographics:
- Males affected 8–10× more than females (striking predominance)
- Peak incidence: third to fifth decade of life
- In the USA: predominantly young, often Hispanic, adult males with travel history
Life cycle and pathogenesis:
- Ingestion of mature E. histolytica cysts or trophozoites via fecally contaminated food/water
- Cyst wall degraded in intestine → trophozoites released → multiply in colonic lumen
- Trophozoites invade intestinal mucosa → enter mesenteric veins → portal circulation → liver (typically 2–4 months after colitis)
- In the liver: trophozoites obstruct venules → thrombosis and infarction of hepatic parenchyma → liquefactive necrosis ("anchovy paste" content — thick, brown, proteinaceous fluid with necrotic hepatocytes and trophozoites)
Host factors increasing severity: Younger age, pregnancy, malnutrition, alcoholism, corticosteroid use, malignancy, HIV/AIDS (immunosuppression).
Clinical Presentation
- Onset: typically 8–20 weeks after return from endemic area
- Fever: ~80% (may be less dramatic than PLA)
- Right upper quadrant pain (often dull, constant): ~60%
- Cough, night sweats, malaise, weight loss, hiccough — common
- Diarrhea: only ~30% (concurrent active intestinal amebiasis is uncommon)
- Jaundice: ~10% (less common than PLA)
- Marked hepatomegaly — especially in travelers vs. endemic residents
Laboratory:
- Leukocytosis (eosinophilia is NOT typically seen — E. histolytica is a protozoan, not a tissue-invasive helminth)
- Elevated ALP (~80%)
- Elevated transaminases
- No eosinophilia (distinguishes from parasitic worm infections)
Diagnosis
Imaging:
- Ultrasound: round, well-defined, hypoechoic (sometimes anechoic) mass; predominantly in right lobe; tends to be solitary (vs. multiple in PLA)
- CT: low-density mass with peripheral enhancing rim; cannot reliably distinguish from PLA
- MRI: low signal on T1, high signal on T2; superior capsule delineation
- CXR: elevation of right hemidiaphragm in ~50%; right pleural effusion
Sonogram and CT showing multiple amebic abscesses:
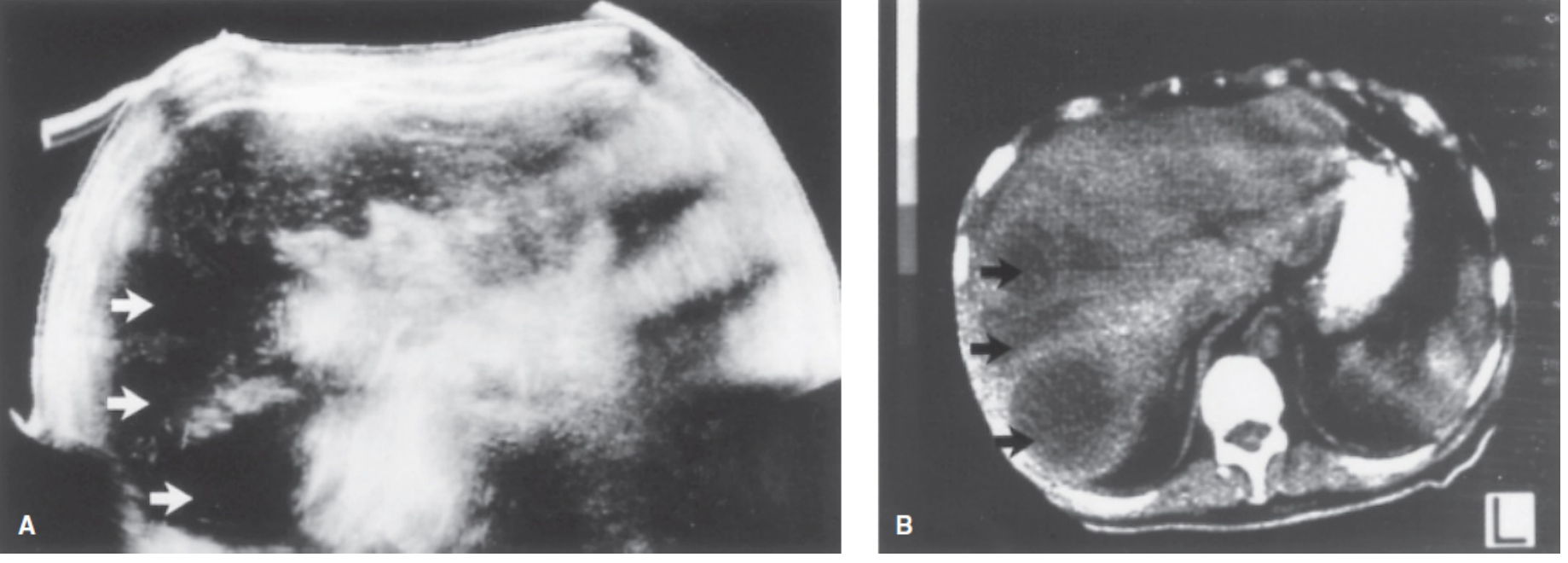
Sonogram (A) and CT (B) showing multiple amebic liver abscesses (arrows) — Mulholland & Greenfield's Surgery 7e
Serologic testing — key diagnostic tool:
- Amebic serology (antibody): sensitive, but 1/3 of patients with prior E. histolytica infection have persistent antibodies without active disease
- Antigen testing (stool or serum): more specific for active infection
- Antibodies detectable in serum 7–10 days after symptom onset in >90% of patients
- Stool examination for trophozoites/cysts: unreliable (intermittent shedding; simultaneous intestinal disease uncommon in those with ALA)
Aspiration / PCR:
- Content: "anchovy paste" — dark brown, thick, acellular, proteinaceous fluid; trophozoites found at abscess wall, not in the central pus
- Aspirate antigen or PCR testing: most sensitive method; sensitivity 75–100%, specificity >90%
- PCR is 100% sensitive before treatment (vs. ~70% after treatment begins)
Differential Diagnosis (ALA vs. PLA — Key Distinctions)
| Feature | Amoebic (ALA) | Pyogenic (PLA) |
|---|---|---|
| Age / Sex | Young male, 8–10:1 M:F | Older, slight male predominance |
| Geography | Travel to/from tropics | Any setting; biliary disease |
| Number | Usually single | Often multiple |
| Lobe | Right lobe predominant | Either, right more common |
| Content | "Anchovy paste" (brown) | Creamy yellow-white pus |
| Diarrhea | ~30% | Rare |
| Eosinophilia | Absent | Absent |
| Serology | Positive >90% | Negative |
| Blood cultures | Negative | Positive ~50% |
| Response to metronidazole | Dramatic (>90%) | No response |
| Microbiology | E. histolytica | Polymicrobial bacteria |
Additional differential includes: hydatid cyst (echinococcosis), hepatocellular carcinoma (necrotic), biloma, simple cyst, hepatic metastases.
Treatment
1. Medical Treatment (mainstay — >90% respond without drainage)
Tissue amebicides (kill liver organisms):
- Metronidazole 500–750 mg orally/IV 3× daily × 7–10 days — first-line; clinical improvement in >90%
- Tinidazole 2 g orally once daily × 5 days — alternative; better tolerated
Followed by luminal amebicides (eradicate intraluminal cysts — essential to prevent relapse):
- Paromomycin 25–30 mg/kg/day orally in 3 divided doses × 7 days
- Diiodohydroxyquin (iodoquinol) 650 mg orally 3× daily × 20 days
- Diloxanide furoate 500 mg orally 3× daily × 10 days
2. Percutaneous Aspiration / Drainage (selective)
Indications for aspiration in ALA:
- Large abscess (especially >10 cm) — risk of spontaneous rupture
- Failure to respond to metronidazole within 72–96 hours
- Left lobe abscess (high risk of rupture into pericardium)
- Diagnostic uncertainty (cannot exclude PLA)
- Imminent rupture
ALA almost never requires surgical drainage under non-complicated circumstances.
3. Surgical Treatment
Reserved for:
- Rupture into peritoneal cavity — peritonitis (emergency laparotomy, peritoneal lavage, drainage)
- Rupture into pericardium (rare, life-threatening emergency)
- Thoracoabdominal fistula not amenable to percutaneous management
- Secondary bacterial superinfection not responding to antibiotics + aspiration
Complications of ALA (Parasitic Liver Disease)
- Rupture into peritoneal cavity (most common complication, ~7% of cases): severe peritonitis, septic shock
- Pleuropulmonary extension (most common route after peritoneal): right pleural effusion, empyema, hepatobronchial fistula, lung abscess — the lung is the second most common extraintestinal site after the liver
- Rupture into pericardium (left lobe abscesses): pericardial tamponade, constrictive pericarditis — high mortality
- Secondary bacterial superinfection — converts to mixed pyogenic-amoebic abscess
- Cerebral amebiasis (hematogenous spread — rare but nearly uniformly fatal)
- Cutaneous amebiasis (perianal extension)
PART III — PARASITIC DISEASES OF THE LIVER: COMPLICATIONS OVERVIEW
Echinococcosis (Hydatid Disease)
Etiology: Echinococcus granulosus (cystic, common) or E. multilocularis (alveolar, more aggressive). Dog is definitive host; sheep/cattle are intermediate hosts; humans acquire infection by ingesting eggs from contaminated food or contact with infected dogs.
Pathogenesis: Eggs hatch in duodenum → oncospheres penetrate intestinal wall → portal circulation → lodge in hepatic capillaries → develop into hydatid cysts. Right lobe in 60–85%.
Clinical: Usually asymptomatic until cyst is large (≥10 cm). Symptoms: RUQ pain, hepatomegaly, nausea/vomiting, biliary obstruction/jaundice, portal hypertension. Cysts grow 1–3 cm/year.
Diagnosis: US (90–95% sensitivity): smooth, anechoic cyst with "hydatid sand" on movement. CT: can demonstrate intraperitoneal rupture. MRI: superior cyst capsule delineation. Serology (ELISA) — most sensitive.
Complications:
- Rupture into peritoneal cavity → anaphylaxis, secondary seeding (catastrophic)
- Biliary communication → cholangitis, obstructive jaundice
- Secondary infection → pyogenic superinfection
- Venous obstruction → portal hypertension
- Sepsis
Treatment — Surgical (treatment of choice for large/complicated cysts):
- Goal: remove cyst intact without spillage of scoleces
- Pre-operative aspiration of cyst contents + injection of scolicidal agent (ethyl alcohol or 20% sterile saline) before resection
- If aspirate is bilious (biliary communication suspected): resect without alcohol injection (risk of sclerosing cholangitis)
- Approach: open or laparoscopic depending on cyst features/location
- Albendazole started 4 days before surgery, continued ≥4 weeks postoperatively (mebendazole as alternative, less well-absorbed, ≥3 months)
- PAIR (Puncture-Aspiration-Injection-Reaspiration): minimally invasive option for select cases
Summary Table: Key Comparative Features
| Pyogenic Abscess | Amoebic Abscess | Hydatid Cyst | |
|---|---|---|---|
| Etiology | Bacteria (polymicrobial) | E. histolytica | Echinococcus spp. |
| Transmission | Biliary/portal/hematogenous | Fecal-oral | Fecal-oral (dog contact) |
| Sex ratio | Slight male predominance | 8–10:1 M:F | Male predominance |
| Multiplicity | Often multiple | Usually single | Usually single |
| Content | Pus | "Anchovy paste" | "Water lily" cyst fluid, scoleces |
| Key diagnosis | CT, blood/aspirate culture | Serology, PCR | US ("hydatid sand"), ELISA |
| Primary treatment | Antibiotics + percutaneous drainage | Metronidazole + luminal agent | Surgery + albendazole |
| Surgical indications | Failure of perc drainage, rupture, multiloculated | Rupture, pericardial extension | Large/complicated cysts |
| Mortality | 4–10% | Low with treatment | Variable |
Sources:
- Current Surgical Therapy, 14th edition (Mulholland/Cameron)
- Mulholland and Greenfield's Surgery: Scientific Principles and Practice, 7th edition
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
Anatomy and physiology in detail
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.