Here is your complete, MUHS exam-ready Pathology notes on Neoplasia - covering all the topics you listed, with diagrams, H&E morphology, gross pathology, and easy-to-remember points.
NEOPLASIA - Complete MUHS Exam Notes
Based on Robbins & Kumar Basic Pathology | Harsh Mohan | Robbins Pathology
PART 1: NEOPLASIA - Definition, Classification
Definition (learn this by heart)
Neoplasia = "New growth." A neoplasm is a mass of cells showing uncontrolled, purposeless proliferation that is autonomous - it persists even after the stimulus causing it is removed.
- Oncology = study of tumors (oncos = tumor)
- All neoplasms consist of: (1) parenchyma (proliferating neoplastic cells) + (2) stroma (supporting connective tissue + blood vessels)
Classification of Neoplasms
| Feature | Benign | Malignant |
|---|
| Growth rate | Slow | Rapid |
| Capsule | Present (well-encapsulated) | Absent / irregular |
| Borders | Well-defined | Ill-defined, infiltrative |
| Differentiation | Well-differentiated | Poorly differentiated / anaplastic |
| Mitoses | Rare, normal | Frequent, abnormal |
| Metastasis | ABSENT | PRESENT |
| Necrosis | Absent | Common (outgrows blood supply) |
| Recurrence after surgery | Rare | Common |
| Effect on host | Local pressure effects | Local invasion + distant spread + systemic effects |
| Vascularity | Less | More (angiogenesis) |
Naming Convention:
| Origin | Benign | Malignant |
|---|
| Epithelial - squamous | Squamous cell papilloma | Squamous cell carcinoma |
| Epithelial - glandular | Adenoma | Adenocarcinoma |
| Fibroblasts | Fibroma | Fibrosarcoma |
| Smooth muscle | Leiomyoma | Leiomyosarcoma |
| Striated muscle | Rhabdomyoma | Rhabdomyosarcoma |
| Bone | Osteoma | Osteosarcoma |
| Cartilage | Chondroma | Chondrosarcoma |
| Fat | Lipoma | Liposarcoma |
| Blood vessels | Hemangioma | Angiosarcoma |
| Lymphoid | - | Lymphoma / Leukemia |
| Melanocytes | Nevus | Melanoma |
| Mixed (germ cell) | Teratoma (mature) | Teratoma (immature/malignant) |
PART 2: TERATOMA
- Arise from totipotent germ cells (gonads - testis/ovary, or extragonadal - mediastinum, retroperitoneum, sacrococcygeal region)
- Contain tissues from all 3 germ layers (ecto, meso, endoderm) in a disorganized arrangement
- Mature (benign) teratoma: Dermoid cyst of ovary - most common. Contains skin, hair, teeth, sebaceous glands
- Immature (malignant) teratoma: Contains immature fetal-type tissues (neuroepithelium). More common in males. AFP elevated
- Exam tip: Benign teratoma = mature (differentiated); Malignant teratoma = immature (poorly differentiated, AFP +ve)
PART 3: PRECANCEROUS LESIONS (Premalignant Lesions)
These are non-neoplastic lesions that carry a significantly higher risk of transforming into cancer than normal tissue.
A. Precancerous Conditions (Acquired)
| Precancerous Condition | Cancer Risk |
|---|
| Leukoplakia (oral, vulvar) | Squamous cell carcinoma |
| Oral submucous fibrosis (OSMF) | Oral squamous cell carcinoma |
| Cervical erosion / CIN (Cervical Intraepithelial Neoplasia) | Cervical carcinoma |
| Barrett's esophagus | Adenocarcinoma of esophagus |
| Ulcerative colitis (>10 yrs) | Colorectal carcinoma |
| Cirrhosis of liver | Hepatocellular carcinoma |
| Paget's disease of bone | Osteosarcoma |
| Xeroderma pigmentosum | Skin carcinoma / melanoma |
| Chronic atrophic gastritis | Gastric carcinoma |
| Actinic (solar) keratosis | Squamous cell carcinoma of skin |
| Undescended testis (cryptorchidism) | Seminoma |
| Villous adenoma of colon | Colorectal carcinoma |
| Bowen's disease | Squamous cell carcinoma |
B. Precancerous Epithelial Changes (Histological)
- Dysplasia: Loss of uniformity + architectural disorientation of epithelial cells. Cells show variation in size, shape; increased N:C ratio; nuclear hyperchromatism; abnormal mitoses
- Carcinoma in situ (CIS): Full-thickness epithelial dysplasia with intact basement membrane. This is the final premalignant stage
- Progression: Normal → Hyperplasia → Dysplasia (mild → moderate → severe) → CIS → Invasive carcinoma
PART 4: ANAPLASTIC TUMOR CELLS - MORPHOLOGY
Anaplasia = Loss of differentiation. Hallmark of malignancy. From Greek - "to form backward."
Morphological Features of Anaplastic Cells (H&E - Easy to draw):
ANAPLASTIC CELL - KEY FEATURES:
┌─────────────────────────────────┐
│ PLEOMORPHISM │
│ (variable cell/nuclear size) │
│ │
│ ■ Large hyperchromatic nucleus│
│ ■ N:C ratio markedly increased│
│ ■ Coarse, clumped chromatin │
│ ■ Prominent nucleoli │
│ ■ Abnormal mitotic figures │
│ (tripolar/quadripolar) │
│ ■ Giant cells (tumor giant │
│ cells) - mono/multinucleate │
│ ■ Loss of polarity │
└─────────────────────────────────┘
Features in Detail:
| Feature | Description |
|---|
| Pleomorphism | Cells and nuclei vary widely in size and shape |
| Nuclear hyperchromatism | Dark-staining nuclei (excess DNA) |
| Increased N:C ratio | Nucleus occupies most of cell (> 1:1, normally 1:4-6) |
| Prominent nucleoli | Large, multiple, irregular nucleoli ("owl eye") |
| Abnormal mitoses | Tripolar, quadripolar, dispersed spindles |
| Loss of polarity | No orderly arrangement; cells pile on each other |
| Tumor giant cells | Huge cells with single huge nucleus or multiple nuclei |
| Loss of cell cohesion | Due to decreased E-cadherin |
| Necrosis | Central necrosis (outgrows blood supply) |
Exam tip: The 3 most important features = Pleomorphism + Hyperchromatism + Abnormal mitoses
PART 5: BENIGN vs MALIGNANT - DIFFERENCES (★★★★)
| Feature | Benign | Malignant |
|---|
| Differentiation | Well-differentiated; resembles tissue of origin | Poorly differentiated to anaplastic |
| Rate of growth | Slow, progressive; may cease/regress | Erratic; generally rapid |
| Mitoses | Few, normal | Numerous, abnormal |
| Capsule | Usually encapsulated | Non-encapsulated, invasive |
| Invasion | No local invasion | Locally invasive; infiltrates |
| Metastasis | Never | Frequently present |
| Recurrence | Rare after excision | Tends to recur |
| Necrosis/ulceration | Absent | Common |
| Effect on host | Usually not life-threatening (except location/hormones) | Often fatal |
| Vasculature | Scant, well-formed | Abundant, abnormal |
| Nuclei | Normal; regular | Enlarged; irregular; hyperchromatic |
PART 6: METASTASIS - Definition, Mechanism, Routes (★★★)
Definition
Metastasis = Spread of a malignant tumor to a site discontinuous from the primary tumor, via lymphatics, blood vessels, or body cavities.
It is the most reliable indicator that a tumor is malignant.
The Metastatic Cascade (Steps of Metastasis)
METASTATIC CASCADE:
PRIMARY TUMOR
↓
1. DETACHMENT from primary mass
(↓ E-cadherin expression; SNAIL/TWIST TF activation)
↓
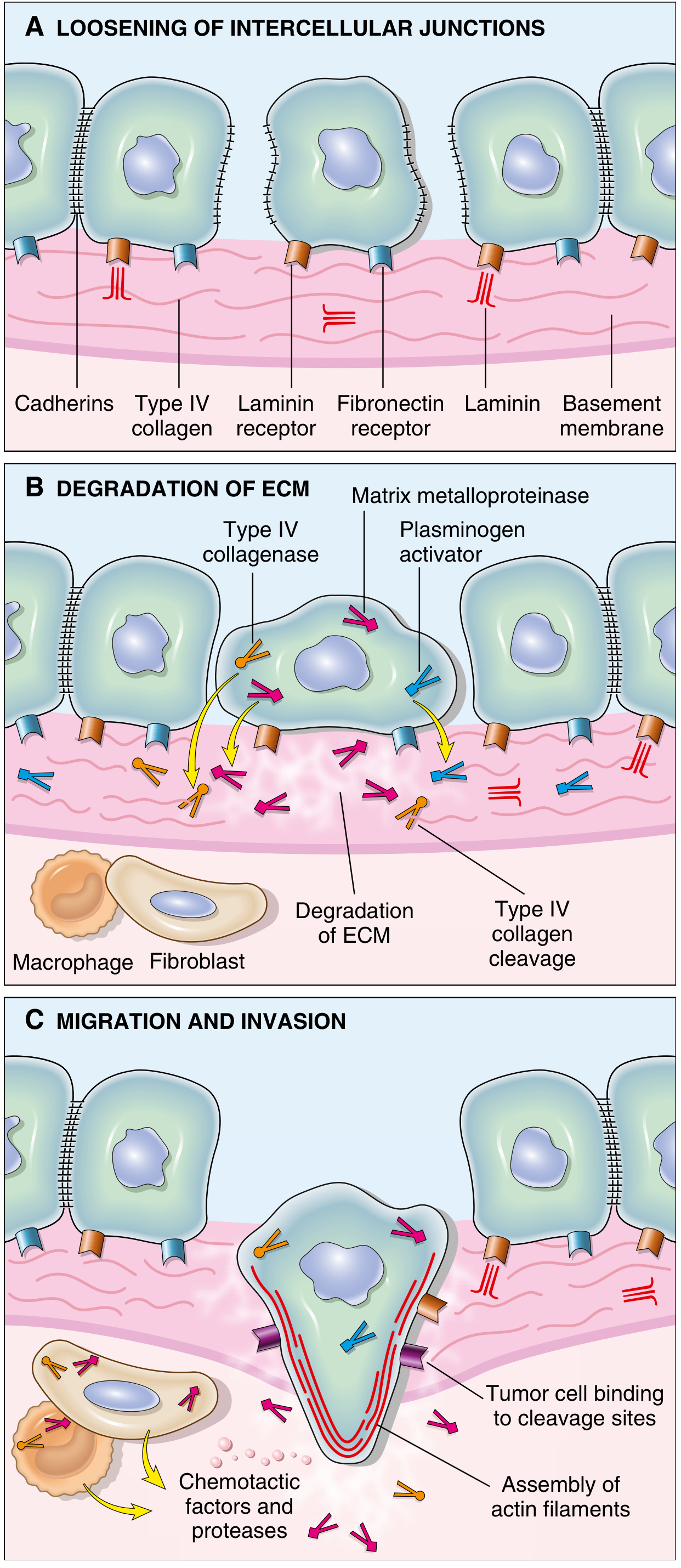
2. INVASION of ECM (basement membrane)
- Secretion of MMPs (matrix metalloproteinases)
- Type IV collagenase digests BM
- Cathepsin D, urokinase plasminogen activator
↓
3. INTRAVASATION
(enter blood/lymph vessels)
↓
4. SURVIVAL IN CIRCULATION
(evade immune surveillance, form tumor emboli)
↓
5. ARREST in distant organ capillaries
(via integrins binding to endothelial laminin)
↓
6. EXTRAVASATION
(exit vessels at distant site)
↓
7. PROLIFERATION at new site
(seed + soil hypothesis - Paget, 1889)
+ Angiogenesis (VEGF)
↓
METASTATIC COLONY
Invasion of ECM - 3 Key Steps (Diagram from Robbins):
Step A: Loosening of intercellular junctions (↓ E-cadherin)
Step B: Degradation of ECM (MMPs, Type IV collagenase, plasminogen activator)
Step C: Migration along degraded matrix (actin cytoskeleton assembly, chemotaxis)
PART 7: ROUTES / PATHWAYS OF SPREAD OF MALIGNANT NEOPLASMS (★★★)
1. Lymphatic Spread (most common in Carcinomas)
- Tumor cells enter lymphatics → regional lymph nodes → distant nodes → thoracic duct → bloodstream
- Sentinel lymph node = first draining lymph node from primary tumor (assessed by dye/radiolabeled tracers)
- Skip metastases: Cells bypass regional nodes and lodge in distant nodes
- Examples:
- Breast carcinoma → Axillary lymph nodes (upper outer quadrant)
- Lung carcinoma → Bronchial → Tracheobronchial → Hilar nodes
- Gastric carcinoma → Left supraclavicular node (Virchow's node = Troisier's sign)
- Testicular carcinoma → Para-aortic nodes
2. Hematogenous Spread (most common in Sarcomas)
- Tumor cells invade thin-walled veins (not arteries)
- Portal vein drainage → Liver (most common hematogenous metastasis site)
- Systemic veins → Lungs (second most common)
- Paravertebral plexus → Spine (prostate, thyroid)
- Organ tropism ("seed and soil"):
- Breast carcinoma → Bone, liver, lungs, brain
- Bronchogenic carcinoma → Adrenals, brain
- Prostate carcinoma → Bone (osteoblastic)
- Neuroblastoma → Liver, bone
- Renal cell carcinoma → Grows as a "plug" in IVC up to heart
3. Transcoelomic / Peritoneal Spread
- Tumor implants on peritoneal, pleural, or pericardial surfaces without invading underlying tissue
- Classic example: Ovarian carcinoma → Peritoneal seeding
- Pseudomyxoma peritonei (mucinous implants in peritoneum)
- Mesothelioma of pleura
4. Spread Along Body Cavities / CSF
- CNS tumors (medulloblastoma, ependymoma) → Penetrate ventricles → carried by CSF → implant on meninges of brain/spinal cord
5. Spread Along Epithelial Surfaces (Direct / Contiguous)
- Tumor invades directly into adjacent structures
- Carcinoma rectum → bladder; Carcinoma cervix → urinary bladder/rectum
Gross Pathology - Liver with Metastasis:
Gross: Multiple pale creamy-white nodules scattered throughout liver parenchyma with umbilication (central depression due to necrosis) - "Cannon-ball deposits."
PART 8: CHEMICAL CARCINOGENESIS (★★★)
Definition
Chemical carcinogens cause cancer through DNA mutations. Most are mutagenic (electrophilic species that form covalent DNA adducts).
Classification of Chemical Carcinogens
A. Direct-Acting Carcinogens (do not require metabolic activation)
- Alkylating agents: Nitrogen mustard, cyclophosphamide, busulfan (iatrogenic cancers)
- Acylating agents: Dimethylcarbamyl chloride
B. Indirect-Acting Carcinogens / Procarcinogens (require metabolic activation to form "ultimate carcinogen")
- Polycyclic aromatic hydrocarbons (PAH): Benzo[a]pyrene (tobacco smoke) → lung cancer
- Aromatic amines / azo dyes: Beta-naphthylamine → bladder cancer; Dimethylaminoazobenzene (DAB, "butter yellow") → liver cancer
- Nitrosamines: N-nitrosodimethylamine → liver, esophagus
- Aflatoxin B1 (from Aspergillus flavus on peanuts/grains) → hepatocellular carcinoma; causes characteristic TP53 codon 249 mutation
- Vinyl chloride → Angiosarcoma of liver
- Benzene → Leukemia
- Asbestos → Mesothelioma + lung carcinoma
- Chromium, nickel, arsenic → Lung cancer
C. Hormones as Promoters
- Estrogen → Endometrial carcinoma, breast carcinoma
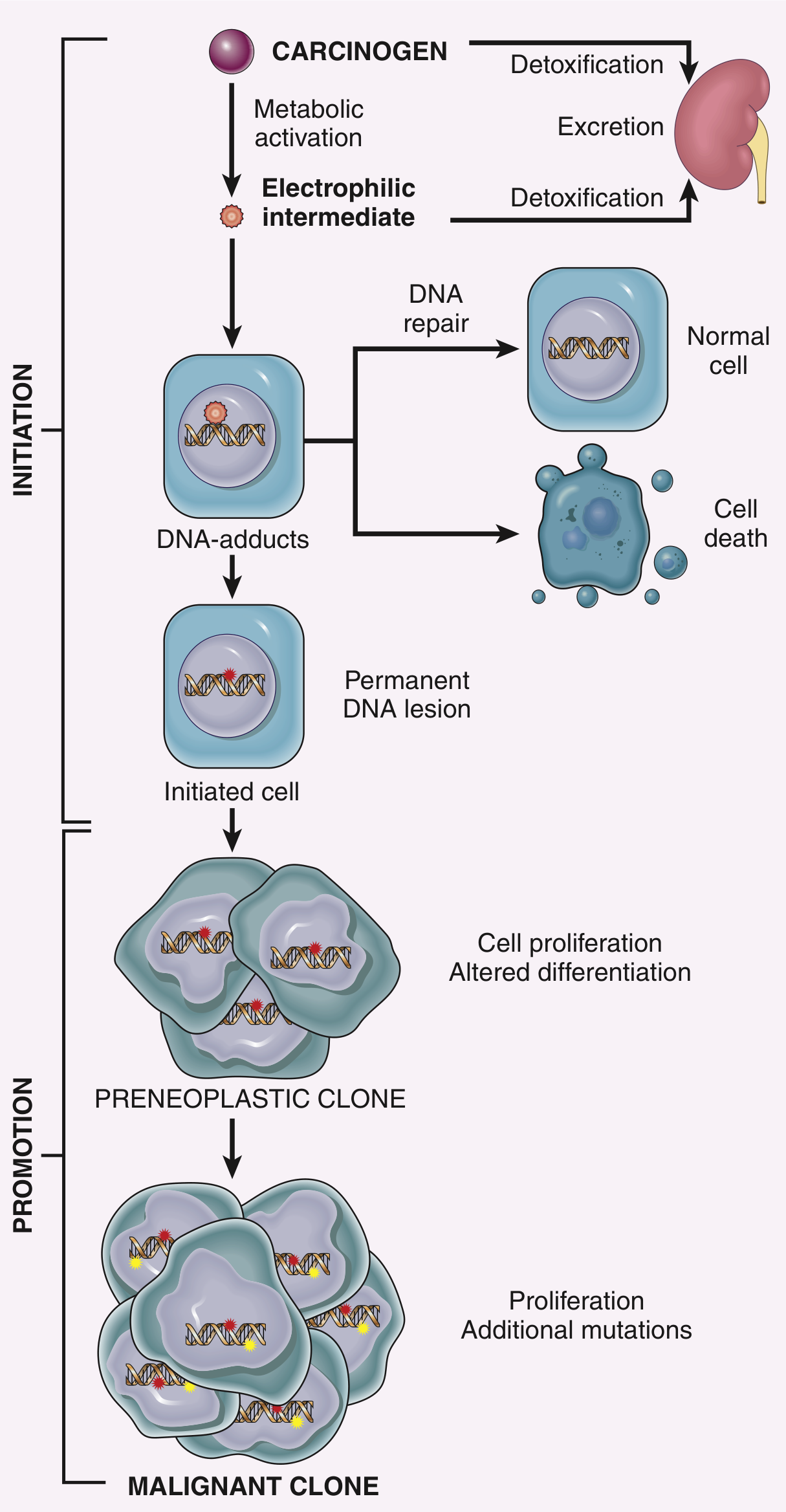
Steps of Chemical Carcinogenesis (★★★)
STEP 1: INITIATION
- Exposure to carcinogen → metabolic activation → electrophilic intermediate forms
- Electrophile forms DNA adducts (covalent bond with DNA)
- If DNA repair fails → Permanent mutation in initiated cell
- Initiation is rapid, irreversible, permanent
- Single exposure sufficient
- Key mutations: RAS, TP53 oncogenes
STEP 2: PROMOTION
- Repeated/sustained exposure to promoters (not mutagenic themselves)
- Promoters cause clonal expansion of initiated cells
- Initiated cells accumulate more mutations → Preneoplastic clone
- Further proliferation + additional mutations → Malignant clone
- Promotion is reversible (if promoter is withdrawn before malignancy established)
- Examples of promoters: Phorbol esters (TPA), hormones, phenols
INITIATION → PROMOTION SEQUENCE:
(Carcinogen) (Promoter - repeated)
↓ ↓
DNA mutation → Clonal expansion → Additional mutations → CANCER
(irreversible) (reversible if (irreversible)
stopped early)
Key Mnemonics:
- INITIATION = Irreversible, Immediate
- PROMOTION = Prolonged, Partially reversible
PART 9: ONCOGENIC VIRUSES (Viral Carcinogenesis)
DNA Viruses (most important)
| Virus | Cancer Caused |
|---|
| HPV (Human Papillomavirus) | Cervical carcinoma (types 16, 18, 31, 33), penile cancer, oropharyngeal cancer |
| EBV (Epstein-Barr Virus) | Burkitt's lymphoma, Hodgkin lymphoma, Nasopharyngeal carcinoma, Post-transplant B-cell lymphoma |
| HBV (Hepatitis B Virus) | Hepatocellular carcinoma (HCC) |
| HHV-8 (Kaposi Sarcoma Herpesvirus) | Kaposi sarcoma, Primary effusion lymphoma |
| MCPV (Merkel Cell Polyomavirus) | Merkel cell carcinoma (skin) |
RNA Viruses (Retroviruses)
| Virus | Cancer Caused |
|---|
| HTLV-1 (Human T-cell Leukemia Virus-1) | Adult T-cell leukemia/lymphoma |
| HCV (Hepatitis C Virus) | Hepatocellular carcinoma; Hepatosplenic lymphoma |
Mechanisms:
- HPV: E6 protein degrades p53 (tumor suppressor); E7 binds and inactivates RB → uncontrolled cell cycle
- EBV: Latent membrane protein (LMP-1) acts as constitutively active receptor mimicking CD40 → activates NF-κB, Bcl-2 → immortalization
- HBV: Integration into host genome; HBx protein activates growth-promoting genes; chronic injury + inflammation → HCC
- HTLV-1: Tax protein activates cell cycle regulatory genes; suppresses TP53
PART 10: PARANEOPLASTIC SYNDROMES (★★)
Definition
Symptoms and signs in cancer patients not explained by local tumor effects, metastasis, or therapy - caused by ectopic hormone secretion or immune/autoimmune reactions triggered by the tumor.
Common Paraneoplastic Syndromes:
| Syndrome | Manifestation | Most Common Tumor |
|---|
| Cushing syndrome | Hypercortisolism | Small cell lung carcinoma (ectopic ACTH) |
| SIADH | Hyponatremia | Small cell lung carcinoma (ectopic ADH) |
| Hypercalcemia | Polyuria, confusion | Squamous cell lung carcinoma (PTHrP); also breast, myeloma |
| Polycythemia | Elevated RBC | Renal cell carcinoma, hepatocellular carcinoma (ectopic EPO) |
| Carcinoid syndrome | Flushing, diarrhea, wheezing | Carcinoid tumors (serotonin) |
| Lambert-Eaton syndrome | Proximal muscle weakness (improves with use) | Small cell lung carcinoma (anti-VGCC antibodies) |
| Acanthosis nigricans | Dark velvety skin in axilla/neck | Gastric carcinoma |
| Dermatomyositis | Muscle weakness, rash | Lung, breast carcinoma |
| Migratory thrombophlebitis (Trousseau's sign) | Recurrent DVT at unusual sites | Pancreatic carcinoma |
| Non-bacterial thrombotic endocarditis (NBTE) | Sterile vegetations on heart valves | Mucin-secreting adenocarcinomas |
| Eaton-Lambert syndrome | Muscle weakness, hyporeflexia | Small cell lung carcinoma |
| Cerebellar degeneration | Ataxia | Ovarian, lung carcinoma |
Exam tip: Small cell lung carcinoma produces the most paraneoplastic syndromes (ACTH, ADH, Lambert-Eaton)
PART 11: TUMOR MARKERS - Role in Diagnosis (★★)
Definition
Tumor markers = Biochemical substances (proteins, hormones, enzymes, antigens) produced by tumor cells or in response to tumor cells, detectable in blood, urine, or tissues.
Important Tumor Markers:
| Marker | Tumor | Normal Value | Notes |
|---|
| AFP (Alpha-fetoprotein) | Hepatocellular carcinoma, Testicular yolk sac tumor, Embryonal carcinoma | <10 ng/mL | Also ↑ in cirrhosis; normal in pregnancy |
| CEA (Carcinoembryonic Antigen) | Colorectal, Pancreatic, Gastric, Breast, Lung carcinoma | <5 ng/mL | Non-specific; used for monitoring recurrence |
| PSA (Prostate Specific Antigen) | Prostatic carcinoma | <4 ng/mL | Also ↑ in BPH; used to monitor treatment |
| CA-125 | Ovarian carcinoma (fallopian tube) | <35 U/mL | Also ↑ in endometriosis |
| CA 19-9 | Pancreatic carcinoma, colorectal | <37 U/mL | Best marker for pancreatic cancer |
| CA 15-3 | Breast carcinoma | | Used for monitoring |
| β-hCG | Choriocarcinoma, Testicular germ cell tumors | - | Also ↑ in normal pregnancy |
| LDH | Lymphoma, testicular cancer | | Reflects tumor bulk |
| Calcitonin | Medullary carcinoma of thyroid | | Highly specific |
| TRAP (Acid phosphatase) | Prostatic carcinoma | | Old marker; replaced by PSA |
| Chromogranin A | Carcinoid tumors, pheochromocytoma | | Neuroendocrine marker |
| 5-HIAA (urine) | Carcinoid tumor | | Serotonin metabolite |
Role of Tumor Markers in Diagnosis:
- Screening (limited use due to low sensitivity/specificity): PSA for prostate cancer
- Diagnosis: AFP for hepatocellular carcinoma; β-hCG for choriocarcinoma
- Staging: LDH in lymphoma; AFP + β-hCG in testicular germ cell tumors
- Monitoring treatment response: CEA levels fall with successful surgery
- Detecting recurrence: CEA / PSA reappearance after surgery = recurrence
- Prognosis: High AFP = advanced HCC; high LDH = poor prognosis lymphoma
Limitations: No tumor marker is 100% specific or sensitive. False positives (e.g., PSA in BPH; CEA in smokers) and false negatives occur.
PART 12: LABORATORY DIAGNOSIS OF CANCER (★★★)
A. HISTOPATHOLOGY (Gold Standard)
- Biopsy and H&E staining - most definitive method
- Types of biopsy:
- Excision biopsy: Complete excision of small lesion with margins
- Incision biopsy: Partial removal of large lesion
- Core needle biopsy (Tru-cut): Cylinder of tissue
- Fine Needle Aspiration Cytology (FNAC): Aspirate cells only; no tissue architecture
- Frozen section: Rapid intraoperative diagnosis (30 min) to assess margins during surgery
B. CYTOLOGY
- Exfoliative cytology: Cells shed naturally
- Pap smear (cervical carcinoma) - gold standard screening test for cervical cancer
- Sputum cytology (lung carcinoma)
- Urine cytology (bladder carcinoma)
- Pleural/peritoneal fluid analysis
- FNAC (Fine Needle Aspiration Cytology):
- For thyroid, lymph node, breast, salivary gland masses
- Minimally invasive; quick result
- Limitation: No tissue architecture, so cannot distinguish invasion
C. IMMUNOHISTOCHEMISTRY (IHC)
- Uses antibodies tagged with color/fluorescent labels to detect specific antigens in tumor tissue
- Used to:
- Identify tissue of origin of metastasis (e.g., PSA = prostate origin; TTF-1 = lung/thyroid)
- Classify tumors: ER/PR/HER2 in breast cancer (determines therapy)
- Identify lymphoma subtypes: CD20 (B-cell), CD3 (T-cell)
- Prognostication: Ki-67 index (proliferation rate)
D. FLOW CYTOMETRY
- Used in leukemias and lymphomas to identify surface immunophenotype (CD markers)
- Determines cell lineage: B-cell vs T-cell vs myeloid
- Detects aneuploidy (abnormal DNA content)
E. MOLECULAR / GENETIC DIAGNOSIS
- PCR (Polymerase Chain Reaction):
- Detect BCR-ABL transcripts in CML
- Detect minimal residual disease after treatment
- Detect gene rearrangements in lymphoid malignancies
- FISH (Fluorescence In Situ Hybridization):
- Detect chromosomal translocations: t(9;22) in CML; t(8;14) in Burkitt lymphoma
- HER2 amplification in breast cancer
- ALK gene rearrangement in lung cancer
- Next-generation sequencing / Gene panels:
- Comprehensive mutation profiling (EGFR, KRAS, BRAF, etc.)
- Guides targeted therapy decisions
- Liquid biopsy:
- Detection of circulating tumor DNA (ctDNA) in blood
- Detects recurrence early; non-invasive
F. TUMOR MARKERS (BIOCHEMICAL)
(See Part 11 above)
G. IMAGING
- CT scan, MRI, PET-CT scan, Ultrasound
- PET-CT: Uses 18F-FDG (glucose analogue) - cancer cells show high uptake (Warburg effect)
Summary Table - Lab Diagnosis:
CANCER - LAB DIAGNOSIS:
A. HISTOPATHOLOGY - Biopsy (H&E) - GOLD STANDARD
B. CYTOLOGY - Pap smear, FNAC, sputum cytology
C. IHC - Tissue typing, receptor status (ER, PR, HER2)
D. FLOW CYTOMETRY - Leukemia/lymphoma immunophenotyping
E. MOLECULAR - PCR, FISH, NGS, Liquid biopsy
F. TUMOR MARKERS - AFP, CEA, PSA, CA-125, β-hCG
G. IMAGING - CT, MRI, PET-CT
PART 13: EASY-TO-DRAW DIAGRAMS FOR EXAM
Diagram 1: Benign vs Malignant Tumor (H&E appearance)
BENIGN TUMOR MALIGNANT TUMOR
(e.g. Adenoma) (e.g. Adenocarcinoma)
○ ○ ○ ○ ○ ⊕ ◉ ◎ ○ ⊕
○ ○ ○ ○ ○ ◉ ◉ ⊕ ◎ ○
○ ○ ○ ○ ○ ⊕ ○ ◉ ⊕ ◉
───────────── ─ ─ ─ ─ ─ ─ (broken BM)
INTACT BM INVADED STROMA
[uniform cells] [pleomorphic, hyperchromatic
gland formation] nuclei, abnormal mitoses,
invasion of BM]
Diagram 2: Metastatic Cascade (Draw as flow chart)
PRIMARY TUMOR
↓ (↓E-cadherin)
DETACHMENT
↓ (MMPs digest BM)
ECM INVASION
↓
INTRAVASATION → Blood/Lymph
↓ (tumor emboli)
CIRCULATION
↓ (integrins)
ARREST in capillaries
↓
EXTRAVASATION
↓ (VEGF, angiogenesis)
SECONDARY TUMOR
Diagram 3: Chemical Carcinogenesis (2-Step)
CHEMICAL CARCINOGEN (e.g. Benzo[a]pyrene)
↓ Liver CYP450 enzymes (Metabolic activation)
ULTIMATE CARCINOGEN (electrophile)
↓
DNA ADDUCTS
↓ (failed repair)
MUTATION in RAS / TP53
↓ = INITIATION (permanent, irreversible)
PROMOTER (e.g. phorbol ester) - repeated exposure
↓
CLONAL EXPANSION of initiated cells
↓
ADDITIONAL MUTATIONS
↓
MALIGNANT NEOPLASM
Diagram 4: Routes of Metastasis
PRIMARY TUMOR
├─── 1. LYMPHATIC → Lymph nodes → Thoracic duct → Blood
├─── 2. HEMATOGENOUS → Vein → Liver / Lung / Bone
├─── 3. TRANSCOELOMIC → Peritoneum / Pleura / Pericardium
└─── 4. CSF SPREAD → Meninges
QUICK REVISION BOX: HIGH-YIELD ASSOCIATIONS
| Topic | Key Point |
|---|
| Virchow's node | Left supraclavicular - gastric carcinoma |
| Sentinel node | First draining node from primary tumor |
| Seed and Soil theory | Paget, 1889 - explains organ tropism |
| Burkitt lymphoma | t(8;14) - MYC overexpression - EBV |
| Philadelphia chromosome | t(9;22) - BCR-ABL - CML |
| Aflatoxin B1 | TP53 codon 249 mutation → HCC |
| HPV E6 | Degrades p53 |
| HPV E7 | Inactivates RB |
| HTLV-1 Tax protein | Activates cell cycle genes |
| Warburg effect | Aerobic glycolysis in cancer cells - basis of PET scan |
| Teratoma | All 3 germ layers; mature (benign) = dermoid cyst |
| CIS | Full thickness dysplasia, intact basement membrane |
| Lambert-Eaton | Anti-VGCC antibodies; proximal weakness + small cell lung Ca |
| PSA | Prostate cancer; also BPH (false positive) |
| β-hCG | Choriocarcinoma, testicular germ cell tumors |
| AFP | HCC + testicular yolk sac tumor |
Source: Robbins & Kumar Basic Pathology (10th Edition), Chapter 6 - Neoplasia, pp. 214-278. All diagrams and gross images from Robbins Pathology textbook.
EXAM STRATEGY for MUHS:
- For 5-mark questions: Definition + Classification table + 3-4 key features
- For 10-mark questions: Full notes above with diagrams
- Always draw: Metastatic cascade flowchart, Initiation-Promotion diagram, Benign vs Malignant comparison table
- Frequently asked in MUHS: Metastasis routes, Chemical carcinogenesis steps, Benign vs Malignant differences, Tumor markers table, Paraneoplastic syndromes table