Give me complete information about inferior wall mi including ecg findings,sign , symptoms, presentation, management with drugs dose all in short and according to standard guidlines
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
inferior wall MI ECG ST elevation leads II III aVF
Now I have comprehensive data. Let me compile the complete answer.
Inferior Wall MI — Complete Clinical Reference
ANATOMY & CULPRIT VESSEL
| Structure | Detail |
|---|---|
| Territory | Inferior wall of left ventricle (diaphragmatic surface) |
| Culprit artery | Right Coronary Artery (RCA) — ~80% of cases |
| Alternative | Left Circumflex (LCx) — ~20% of cases |
| RV involvement | ~30% of inferior MIs extend to the right ventricle |
| Posterior extension | Common — posterior descending artery territory |
CLINICAL PRESENTATION
Symptoms
- Chest pain — central/epigastric, pressure-like, radiating to jaw, left arm, or back
- Nausea and vomiting — more prominent than in anterior MI (vagal stimulation from RCA territory)
- Diaphoresis
- Dizziness / near-syncope — from bradycardia or hypotension
- Dyspnea
- Epigastric discomfort — often misdiagnosed as GI pathology
Inferior MI classically presents with more prominent vagal features (nausea, vomiting, bradycardia, hypotension) than other MI locations.
Signs
- Bradycardia — sinus bradycardia or AV block (very common; RCA supplies AV node in 90%)
- Hypotension — may indicate RV infarction; worsened by nitrates
- Kussmaul's sign (JVP rise on inspiration) — if RV infarction present
- Clear lung fields — with RV infarction (unlike LV failure)
- Pericardial friction rub — if pericarditis develops (more common with inferior/RV infarction)
- New holosystolic murmur — papillary muscle rupture (posteromedial, 3–5 days post-MI; more common in inferior MI)
- S3/S4 gallop, signs of cardiogenic shock in severe cases
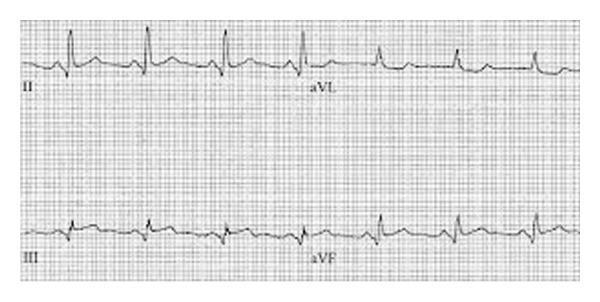
ECG FINDINGS
Primary Changes (Inferior Leads: II, III, aVF)
| Phase | Finding |
|---|---|
| Hyperacute | Tall, broad (hyperacute) T waves in II, III, aVF |
| Acute STEMI | ST elevation ≥1 mm in ≥2 of: II, III, aVF |
| Evolving | Q waves develop in II, III, aVF; T-wave inversion |
| Completed/Old | Pathological Q waves ± persistent T-wave inversion in II, III, aVF |
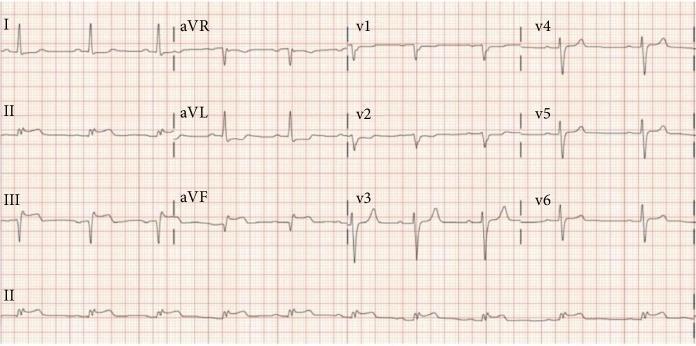
Reciprocal Changes (Highly Specific)
- ST depression in aVL — most consistent reciprocal change; aVL is 150° removed from lead III
- ST depression in lead I — also common
- Reciprocal changes increase specificity and indicate larger infarct + greater mortality risk
RCA vs. LCx Differentiation
| Feature | RCA | LCx |
|---|---|---|
| ST elevation III > II | ✓ Yes | ✗ No |
| ST depression aVL | Prominent | Minimal/isoelectric |
| ST elevation in V1 | RV involvement | Absent |
| Sensitivity for RCA | 90% when III > II + ↓ aVL | — |
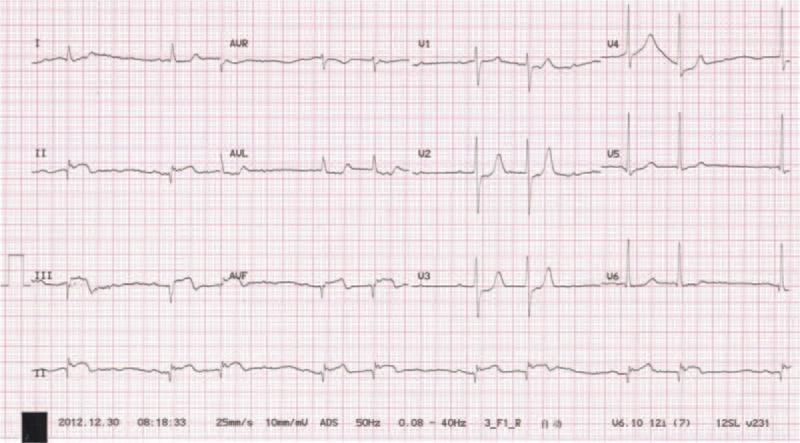
Right Ventricular Infarction (30% of inferior MIs)
- Obtain right-sided leads (V3R–V6R) in ALL inferior MI patients
- ST elevation ≥0.5–1 mm in V4R — highly specific for RV infarction
- ST elevation in V1 with inferior STEMI (elevation III > II) suggests RV involvement
Posterior Extension
- ST depression + tall R wave in V1–V3 = reciprocal of posterior ST elevation
- Obtain posterior leads V7–V9: ST elevation confirms posterior MI
Conduction Abnormalities (Inferior MI specific)
| Block | Frequency |
|---|---|
| Sinus bradycardia | 35–40% |
| First-degree AV block | 4–15% |
| Second-degree (Wenckebach/Type I) | 4–10% |
| Complete (Third-degree) AV block | 5–8% |
AV blocks in inferior MI are usually nodal (narrow QRS, rate ~40–60, vagally mediated, often transient, responsive to atropine) — unlike anterior MI blocks which are infranodal and more dangerous.
ECG IMAGES
MANAGEMENT (AHA/ACC Guidelines)
Immediate (First 10 Minutes)
- IV access, continuous ECG monitoring, O₂ only if SpO₂ <90%
- 12-lead ECG → right-sided leads (V3R–V6R) if inferior MI confirmed
- Serial cardiac biomarkers (troponin, CK-MB)
- Chest X-ray
⚠️ Critical Inferior MI Rule: Avoid nitrates if systolic BP <90 mmHg or if RV infarction suspected — may cause catastrophic hypotension. Adequate IV fluid preload is the treatment for RV infarction hypotension.
Drug Therapy — Doses (AHA/ACC Standard)
ANTIPLATELET AGENTS
| Drug | Dose | Notes |
|---|---|---|
| Aspirin | 162–325 mg PO (chewed, immediately) | Class I; reduces mortality 23% |
| Clopidogrel | 600 mg PO loading, then 75 mg/day | No loading dose if >75 yrs + fibrinolytic; alternative if aspirin allergy |
| Ticagrelor | 180 mg PO loading, then 90 mg twice daily | Preferred over clopidogrel; reversible P2Y12 blocker |
| Prasugrel | 60 mg PO loading, then 10 mg/day (only after PCI + known anatomy) | Contraindicated in prior stroke/TIA; avoid if age ≥75 or weight <60 kg |
ANTITHROMBINS
| Drug | Dose |
|---|---|
| Unfractionated Heparin (UFH) | 60 units/kg IV bolus (max 4,000 units) → infusion 12 units/kg/h (max 1,000 units/h); titrate to aPTT 1.5–2.5× control |
| Enoxaparin (LMWH) | 30 mg IV bolus → 1 mg/kg SC every 12 h |
| Fondaparinux | 2.5 mg SC once daily |
FIBRINOLYTIC THERAPY (if PCI unavailable within 120 min)
| Drug | Dose |
|---|---|
| Alteplase (tPA) | 15 mg IV bolus; then 0.75 mg/kg over 30 min (max 50 mg); then 0.5 mg/kg over 60 min (max 35 mg) |
| Reteplase | 10 units IV over 2 min; repeat 10 units 30 min later |
| Tenecteplase (TNK) | Weight-based single bolus: <60 kg → 30 mg; 60–70 kg → 35 mg; 70–80 kg → 40 mg; 80–90 kg → 45 mg; ≥90 kg → 50 mg |
| Streptokinase | 1.5 million units IV over 60 min |
Time targets: PCI-capable hospital: door-to-balloon ≤90 min | Transfer for PCI: ≤120 min | Fibrinolysis if PCI not achievable: within 30 min of ED arrival
NITROGLYCERIN
| Route | Dose | Caution |
|---|---|---|
| Sublingual | 0.4 mg every 5 min × 3 PRN | Hold if SBP <90 or RV infarction |
| IV | Start 10 mcg/min; titrate up; reduce MAP by 10% (normotensive) or 30% (hypertensive) | — |
MORPHINE
- 2–5 mg IV every 5–15 min PRN for pain
BETA-BLOCKERS
- Metoprolol: 25–50 mg PO (or 5 mg IV q5min × 3 if needed)
- Atenolol: 25–50 mg PO
- Withhold if: HR <60, SBP <100, PR >0.24s, 2nd/3rd degree AV block, active asthma, signs of cardiogenic shock
- ⚠️ Inferior MI with bradycardia/AV block — use with extreme caution
ACE INHIBITORS (start within 24 h if tolerated)
- Ramipril: 2.5–5 mg PO twice daily (titrate up)
- Lisinopril: 5 mg PO once daily, then 10 mg after 24 h
- Indicated for EF ≤40%, anterior MI, heart failure — also beneficial in inferior MI
STATINS
- Atorvastatin 40–80 mg PO — high-intensity statin, start immediately
Reperfusion Strategy
| Strategy | Indication | Target Time |
|---|---|---|
| Primary PCI | Preferred; PCI-capable center available | Door-to-balloon ≤90 min |
| Transfer for PCI | No on-site PCI | ≤120 min total |
| Fibrinolysis | PCI not available within timeframe, no contraindications | Within 30 min of arrival |
COMPLICATIONS (Inferior MI Specific)
| Complication | Details |
|---|---|
| AV block | Common; usually transient Wenckebach; responds to atropine 0.5–1 mg IV; temporary pacing if refractory |
| RV infarction | Hypotension + clear lungs + JVD; treat with IV fluids (500–1000 mL NS challenge), avoid nitrates/diuretics |
| Papillary muscle rupture | Posteromedial papillary muscle (single blood supply from RCA); acute MR; pulmonary edema; holosystolic murmur → surgical emergency |
| Pericarditis | 2–4 days post-MI; pleuritic chest pain; friction rub; treat with aspirin 650 mg q4–6h or colchicine 0.6 mg twice daily |
| Dressler's syndrome | 2–10 weeks post-MI; fever + pleuropericarditis; treat with aspirin + colchicine |
| Sinus bradycardia | Very common; treat with atropine 0.5–1 mg IV if symptomatic |
| Posterior extension | Concurrent in many inferior MIs; identify with posterior leads V7–V9 |
KEY CLINICAL PEARLS
- ST III > ST II + reciprocal ↓ aVL = RCA occlusion (~90% sensitive, 71% specific)
- ST II > ST III + isoelectric/elevated aVL = LCx occlusion (often ECG-silent on standard 12-lead)
- Always get right-sided leads in inferior MI — missing RV infarction has lethal consequences
- Nitroglycerin + RV infarction = cardiovascular collapse — always check right-sided leads first
- AV blocks in inferior MI are usually benign and transient — the AV node recovers with reperfusion
- Nausea/vomiting/epigastric pain in a middle-aged patient with risk factors = rule out inferior MI first
Sources: Tintinalli's Emergency Medicine (9th ed.), Rosen's Emergency Medicine (10th ed.), Goldman-Cecil Medicine — medical-library textbooks
This is a shared conversation. Sign in to Orris to start your own chat.