Exercise to train swing phase and stance phase in hemiplegia patient and correct walking
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have solid textbook content to provide a comprehensive answer. Let me compile everything.
Gait Rehabilitation in Hemiplegia: Training Swing and Stance Phases
Understanding the Normal Gait Cycle First
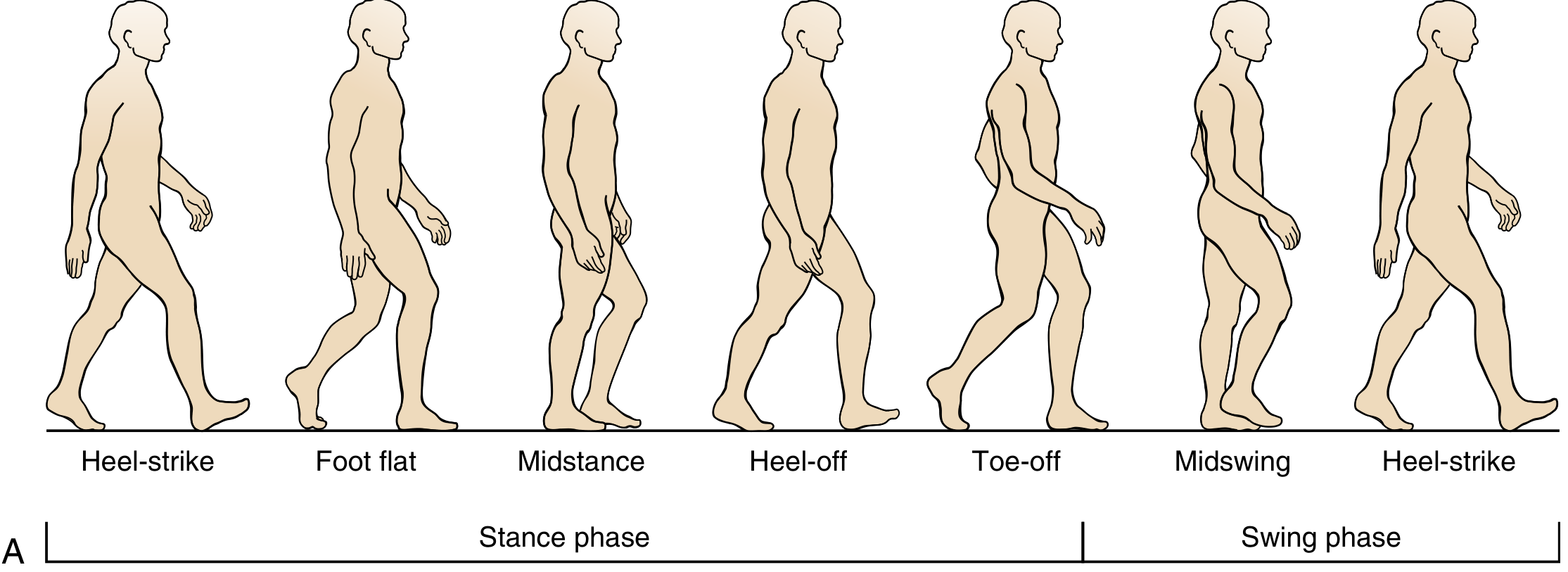
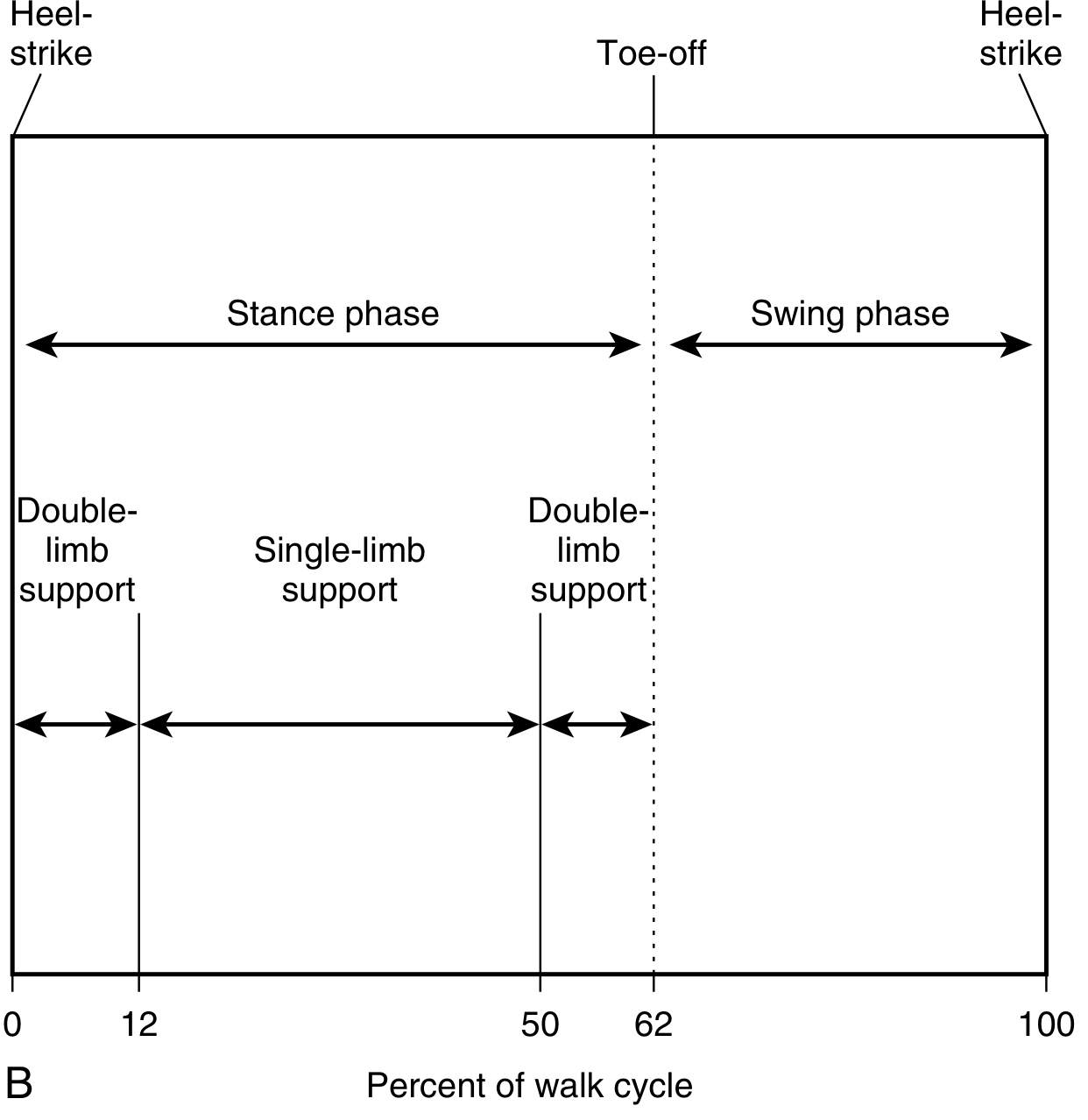
Normal gait = Stance phase (62%) + Swing phase (38%). In hemiplegia, stance is pathologically prolonged and double-limb support time increases.
Hemiplegic Gait: Key Impairments
The hemiplegic gait pattern is characterized by:
- Prolongation of stance and double-limb support on the affected side
- Excessive plantar flexion (equinus foot) → prevents heel strike
- Weakness of ankle dorsiflexors, hip flexors, and knee flexors
- Spasticity of plantar flexors → foot drop / flat-foot landing during swing
- Limited knee flexion during swing → circumduction or hip hiking to clear the foot
- Increased hip flexion
- Balance impairment
— Miller's Review of Orthopaedics, 9th Ed. | Bradley and Daroff's Neurology in Clinical Practice
Exercises to Correct the Swing Phase
The primary problems in swing are: foot drop (inadequate dorsiflexion), inadequate knee flexion, and compensatory hip hiking / circumduction.
1. Ankle Dorsiflexion Training (Anti-Foot Drop)
- Active assisted dorsiflexion: therapist assists the paretic foot into dorsiflexion repeatedly; patient attempts to hold the position.
- Resisted dorsiflexion (Theraband around forefoot): sitting, patient pulls foot upward against band resistance — trains tibialis anterior concentrically (the muscle that contracts concentrically during swing to clear the foot).
- Heel slides on mat: supine, slide heel toward buttocks while maintaining foot dorsiflexed.
- Functional electrical stimulation (FES) to the peroneal nerve can trigger dorsiflexion at swing initiation.
2. Hip and Knee Flexion for Limb Clearance
- Step-through with high knee lift: patient practices exaggerated hip and knee flexion on the affected side to clear the foot, progressing to normal step length.
- Seated knee curls: sitting on edge of bed/chair, patient actively flexes the knee to 90° or beyond — trains hamstrings for swing initiation.
- Treadmill gait training with partial body weight support (BWS): reduces fall risk while allowing repetitive swing phase practice at varied speeds.
- Step-up/step-over obstacles: placing a small obstacle (cone or roll) on the floor forces hip and knee flexion to step over it — directly challenges swing clearance.
- Hip flexor strengthening (supine): straight leg raises or marching in place to improve hip flexion initiation at swing.
3. Reducing Circumduction
- Side-stepping with mirror feedback: patient watches and corrects abnormal hip hiking or trunk lean.
- Treadmill with visual biofeedback or gait labs where applicable.
- Constraint on the sound side (shortened step length training) encourages proper swing mechanics on the affected side.
Exercises to Correct the Stance Phase
The main stance phase problems are: knee instability (hyperextension or buckling), absent heel strike (flat-foot landing due to equinus), impaired single-limb balance, and reduced push-off.
1. Weight-Bearing Stability and Knee Control
- Parallel bar standing: patient bears weight through the affected limb with therapist guarding; focus on avoiding knee hyperextension.
- Weight shifting side to side: standing, therapist guides pelvis to shift weight onto the paretic leg and back — trains single-limb stance loading.
- Mini-squats / sit-to-stand: trains quadriceps eccentrically (controls knee flexion at loading response) and concentrically (terminal stance extension).
- Step-up on affected leg: step up onto a low step with the paretic leg leading — strengthens quadriceps for stance-phase stability.
2. Heel Strike and Push-Off Training
- Rocking on a rocker board (heel to toe): trains the coordinated sequence of heel strike → foot flat → heel off → toe off.
- Calf raises (with support): standing at parallel bars, rise onto toes on the affected side — trains gastrocnemius-soleus for push-off (toe-off phase).
- Heel walks: patient walks on heels, training tibialis anterior eccentrically at heel strike and maintaining dorsiflexion through mid-stance.
- Treadmill incline walking: forward inclination encourages a more heel-dominant contact pattern.
3. Single-Limb Balance and Pelvic Stability
- Tandem standing on the affected leg (with support progressing to unsupported): improves single-limb stance duration.
- Gluteus medius strengthening (side-lying hip abduction): weakness of the gluteus medius causes Trendelenburg/pelvic drop in midstance — resisted hip abduction in side-lying trains this directly.
- Lateral step-overs: stepping sideways over a low obstacle while keeping trunk upright — challenges hip abductor stability in stance.
- Perturbation training: therapist applies gentle perturbations while patient stands on affected leg — improves reactive balance and ankle strategy.
Orthotic Support During Gait Training
An ankle-foot orthosis (AFO) is critical for many patients:
- A solid AFO prevents foot drop during swing and provides a stable base at heel strike.
- A hinged AFO (with heel stop at ~5° dorsiflexion) allows some dorsiflexion for midstance and sit-to-stand while still supporting swing.
- In patients with combined knee instability + ankle drop, a KAFO (knee-ankle-foot orthosis) allows the knee to lock in stance while clearing the toes for swing.
"These fabricated ankle-foot orthoses are designed for ankle and knee control in a hemiparetic patient... A wider lateral flange with hook-and-loop straps across the front of the ankle provides greater ankle and knee control. The thermoplastic hinged ankle orthotic includes a heel stop to allow about 5 degrees of dorsiflexion for standing up and in the early stance phase of gait." — Bradley and Daroff's Neurology in Clinical Practice
Summary Table
| Phase | Main Problem in Hemiplegia | Target Exercises |
|---|---|---|
| Swing | Foot drop (↓ dorsiflexion) | Resisted dorsiflexion, FES, Theraband |
| Swing | ↓ Knee / hip flexion → circumduction | Step-over obstacles, seated knee curls, high-knee marching |
| Stance — Loading | Absent heel strike (equinus) | Rocker board, heel walks, treadmill incline |
| Stance — Mid | Knee hyperextension / buckling | Weight shifting, mini-squats, step-ups |
| Stance — Mid | Trendelenburg (gluteus medius weak) | Side-lying hip abduction, lateral step-overs |
| Stance — Push-off | Reduced propulsion | Calf raises, toe-off practice |
| All phases | Balance & safety | Parallel bars → unsupported standing → perturbation training |
Progression principle: start in parallel bars with body weight support → advance to assistive device (quad cane, hemi-walker) → progress to independent walking with AFO → community distances. Treadmill training with partial body-weight support accelerates repetition volume especially early post-stroke.
Make a protocol to train lower linb
Asking for Preferences
Reading File
Running Command
Writing File
Running Command
Running Command
Running Command
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Make atext
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.