Give about CT angiography and its correlation in ENT practice
Reading File
Finding Sources
Finding Sources
Searching PubMed
"CT angiography" AND "head and neck"
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Searching PubMed
"CT angiography" AND "otolaryngology"
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have extensive material to write a comprehensive answer. Let me compile everything into a well-structured, authoritative response.
CT Angiography and Its Correlation in ENT Practice
CT angiography (CTA) uses rapid intravenous contrast injection followed by ultrafast helical CT acquisition to image blood vessels with multiplanar and 3D reconstructions. In ENT, it has become a cornerstone for evaluating vascular structures of the head, neck, and temporal bone - replacing or supplementing conventional angiography in many settings. Below is a systematic account of its applications across the major domains of ENT practice.
1. Principles of CTA Relevant to ENT
With multidetector (multislice) CT technology, a rapidly injected IV contrast bolus is tracked through arteries and veins in the region of interest. The continuous acquisition allows reconstruction in any plane, enables 3D volume rendering, and simultaneously images extravascular structures (bone, soft tissue, aerodigestive tract). This makes it uniquely powerful in the head and neck, where vascular, bony, and soft-tissue pathology frequently coexist.
"In CT angiography, the continuous acquisition of images allows following the rapidly injected intravenous bolus of contrast through the arteries and veins of the areas under investigation. The reconstructed images can be rotated in the plane that best demonstrates the vessels."
- Shambaugh Surgery of the Ear
Combined CTA/CTV (angiography + venography) of the temporal bone is now a standard first-line imaging tool for several otologic conditions.
2. Neck Trauma
2a. Penetrating Neck Injuries
Conventional angiography was the traditional gold standard for evaluating vascular injuries from penetrating neck wounds. However, its invasive nature and low yield in hemodynamically stable patients led to a shift toward CTA.
- Multislice helical CTA is a sensitive, noninvasive diagnostic screening test that evaluates both the vascular structures and the aerodigestive structures of the neck simultaneously.
- One study of multislice helical CTA in 91 penetrating neck injuries reported high sensitivity and specificity.
- For Zone I and Zone III injuries in stable patients, arteriography (increasingly CTA) is typically required. Zone II injuries may or may not need vascular imaging depending on clinical signs.
- Indications for vascular imaging after penetrating trauma include: persistent hemorrhage, expanding hematoma, neurologic deficits, Horner syndrome (suggesting sympathetic plexus injury/carotid sheath violation), hoarseness (recurrent laryngeal nerve), and suspected carotid or vertebral injury.
"In stable patients with nonemergent injuries, multislice helical CT angiography can be a useful diagnostic screening test to noninvasively assess cervical vascular structures."
- Cummings Otolaryngology Head and Neck Surgery
2b. Blunt Neck Trauma
Blunt neck injuries from motor vehicle accidents and sports often produce occult vascular injury - thrombosis, intimal tears, dissection, and pseudoaneurysm - that may be delayed in presentation.
- CTA with multiplanar and 3D reconstruction is particularly valuable here because clinical signs are often absent or delayed.
- Specifically, CTA assists in evaluation of carotid artery dissection, vertebral artery injury, and pseudoaneurysm in blunt trauma settings.
- Treatment decisions (surgery, anticoagulation, or observation) are guided by CTA findings including mechanism, type, and location of injury.
"CT angiography is very useful in the diagnosis of arterial injuries in the neck. Specifically, CT angiography using multiplanar and three-dimensional reconstruction capabilities has been described to assist in the evaluation of blunt neck trauma injuries."
- Cummings Otolaryngology Head and Neck Surgery
3. Temporal Bone and Otology
3a. Temporal Bone Fractures and Carotid Canal Injury
High-resolution CT (HRCT) is the primary tool for temporal bone fractures, but CTA plays a targeted role when vascular injury is suspected:
- A fracture through the carotid canal on HRCT carries an ~18% incidence of carotid artery injury (vs. ~5% when the canal is spared).
- In asymptomatic patients with carotid canal fractures, angiography yields little additional clinical utility.
- However, if transient or persistent neurologic deficits are present in basilar skull fractures, HRCT of the temporal bone plus CTA is indicated.
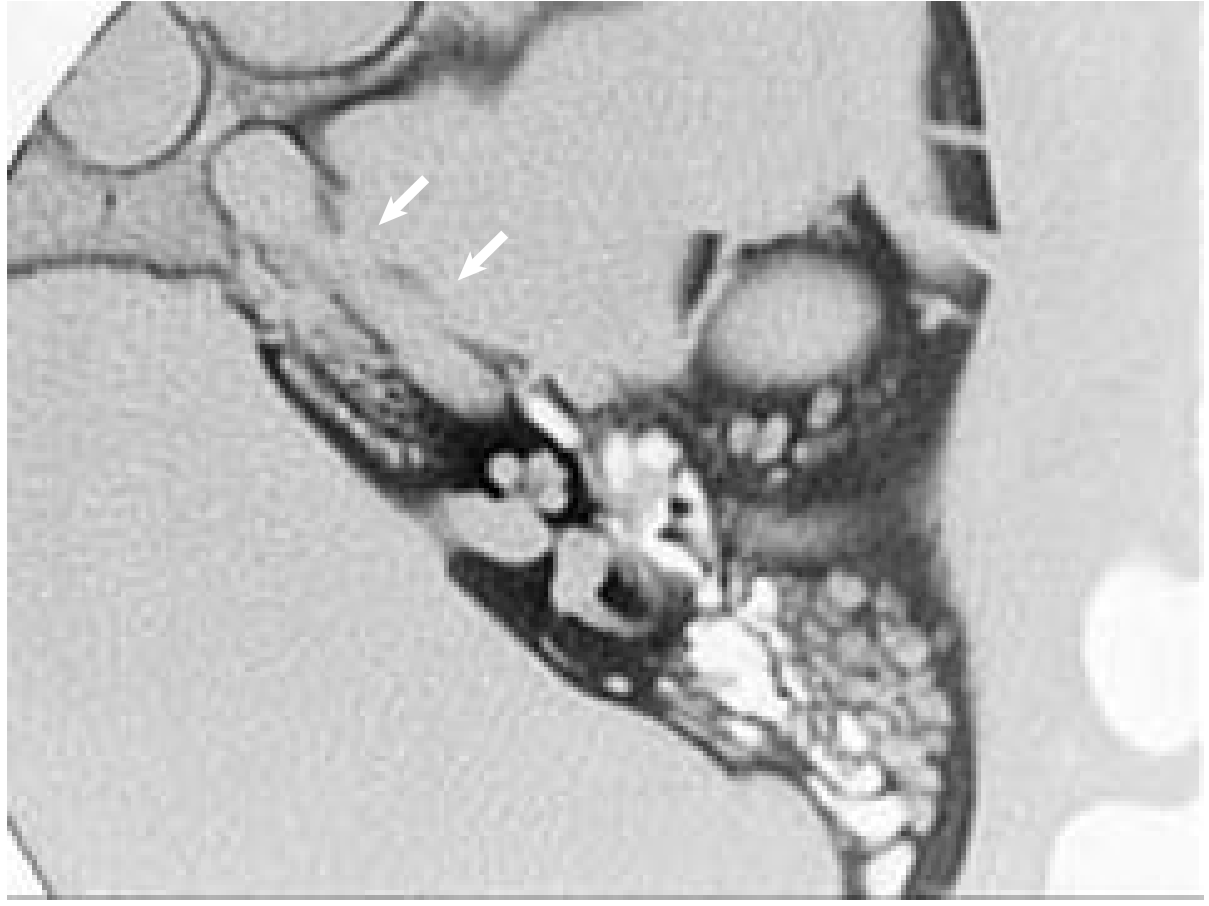
Axial HRCT demonstrating a fracture along the carotid canal (arrows). CTA is indicated if neurologic deficits accompany such fractures. (Cummings Otolaryngology)
3b. Pulsatile Tinnitus
CTA/CTV of the temporal bone is a key imaging modality in the algorithmic work-up of pulsatile tinnitus. The diagnostic algorithm from Cummings is shown below:
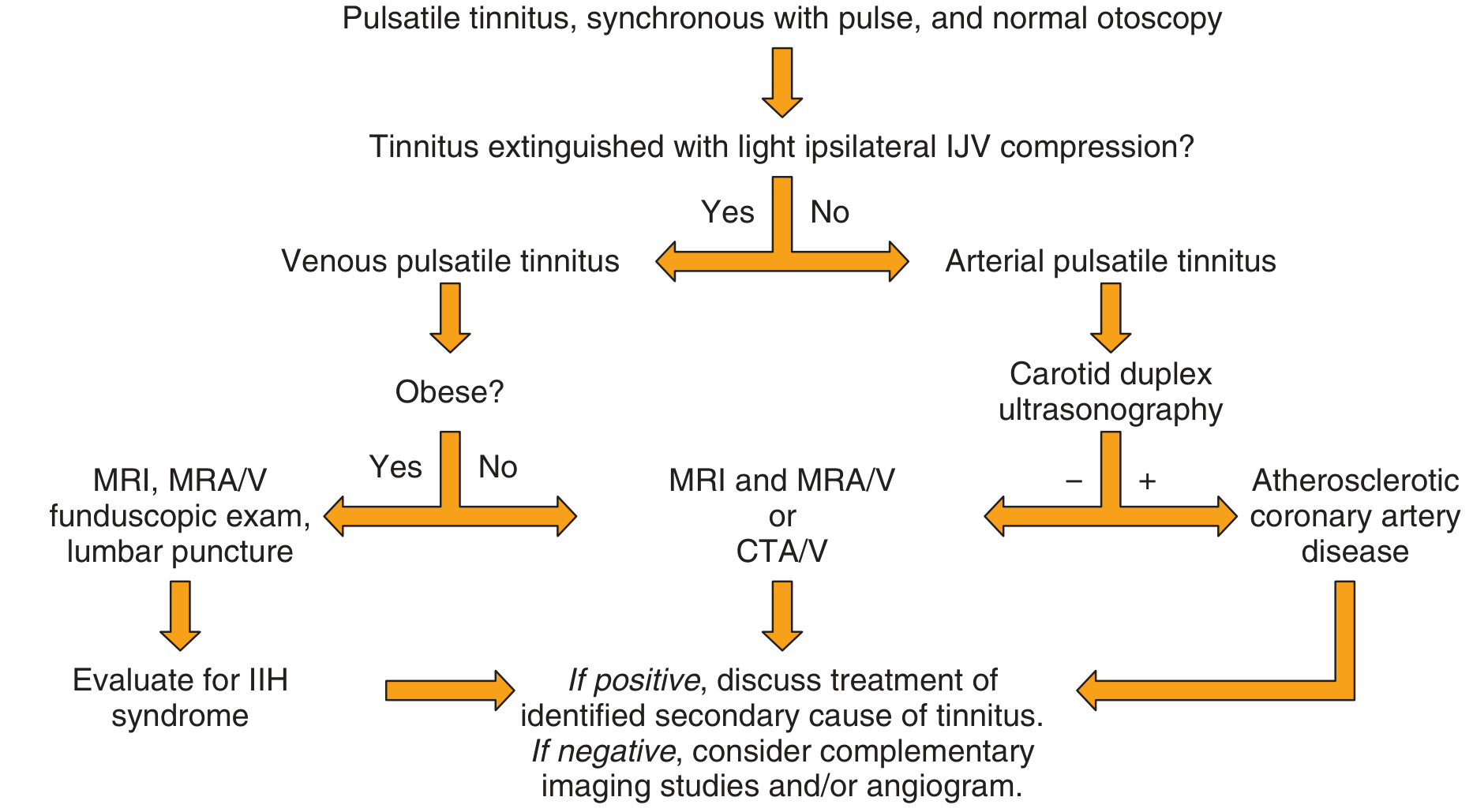
Diagnostic imaging algorithm for pulsatile tinnitus (Cummings Otolaryngology). CTA/V = CT angiography/venography; MRA/V = MR angiography/venography; IIH = idiopathic intracranial hypertension; IJV = internal jugular vein.
CTA-relevant causes of pulsatile tinnitus include:
| Category | Specific Pathology | Role of CTA |
|---|---|---|
| Venous | High-riding jugular bulb, jugular bulb diverticulum | CTA/V temporal bone - first-line imaging |
| Venous | Sigmoid sinus diverticulum | CTA/V - recommended initial study |
| Arterial | Carotid dissection, stenosis, aneurysm | CTA or MRA of head/neck |
| Arterial | Aberrant internal carotid artery | CTA temporal bone |
| AV | Dural AV malformation/fistula | CTA/V (small lesions may be missed - may need 4-vessel angiography) |
| Tumors | Paraganglioma, hemangioma | CT + MRI + angiography in combination |
- For jugular bulb and sigmoid sinus anomalies, CTA/V of the temporal bone is recommended as the initial imaging study.
- For dural arteriovenous malformations (dAVM/F), CTA/V is useful but small lesions can be missed - formal four-vessel angiography may then be required.
4. Paragangliomas (Glomus Tumors) of the Temporal Bone and Neck
CTA has a defined but supplementary role in paraganglioma management:
- CT (bone windows) remains the cornerstone - showing characteristic irregular destruction of the jugular foramen (vs. smooth enlargement in schwannomas).
- MRI provides complementary soft-tissue information (classic "salt-and-pepper" pattern, flow voids).
- Angiography (conventional or CTA) delineates the vascular pattern, which is characteristic for paragangliomas, and is a necessary step in preoperative embolization.
- Critically: CTA and MRA have NOT replaced direct intravascular angiography for glomus tumor management. Conventional angiography remains the gold standard for preoperative embolization planning.
- For skull base neoplasms requiring carotid artery manipulation: temporary balloon occlusion + xenon CT (or radioisotope imaging) is used to assess adequacy of collateral blood flow via the circle of Willis before carotid sacrifice is considered.
"Angiography is a necessary step in preoperative embolization of glomus tumors; in fact MRA, magnetic resonance angiography, and CT angiography (CTA) has not replaced direct intravascular angiography in glomus tumor management."
- Cummings Otolaryngology Head and Neck Surgery
5. Head and Neck Cancer - Preoperative Planning and Reconstruction
5a. Carotid Artery Involvement
In advanced head and neck malignancies, assessment of carotid artery involvement is critical:
- MRA, CTA, Doppler ultrasonography, or conventional angiography can be used preoperatively to assess:
- Carotid artery encasement or invasion (limits resectability)
- Adequacy of external carotid branches to support microvascular anastomosis
- Patency of the transverse cervical artery as a recipient vessel
- Status of jugular venous network (predicting need for sacrifice)
5b. Microvascular Free Flap Reconstruction
CTA is routinely used in preoperative planning for free tissue transfer:
- Fibular free flap: The most commonly used flap for mandibular reconstruction. Preoperative CTA (or MRA/Doppler) of the lower extremities confirms three-vessel runoff and ensures the foot is not dependent on the peroneal artery alone before harvesting the fibula.
- Anterolateral thigh (ALT) flap: CTA or Doppler used to locate and map perforating vessels pre-harvest.
- Other flaps (radial forearm, scapula, iliac crest): Angiographic studies including CTA help detect anatomic vascular anomalies, confirm adequate perforator supply, and document adequacy of distal collateral perfusion.
"CT angiography, angiography, and color Doppler studies can also be utilized, based on surgeon preference" for fibular free flap preoperative planning.
- Cummings Otolaryngology Head and Neck Surgery
6. Vertebral Artery Dissection and Stroke Syndromes
In ENT patients presenting with vertigo, posterior neck pain, or sudden-onset neurologic symptoms, CTA of the head and neck is indicated to evaluate:
- Vertebral artery dissection - especially in the setting of significant ongoing neck pain after trauma
- Carotid artery dissection - associated with Horner syndrome (ptosis, miosis, anhidrosis)
- These presentations may present to ENT/audiovestibular clinics before a neurologic diagnosis is established
7. Comparison with Other Imaging Modalities in ENT
| Modality | Strengths in ENT | Limitations |
|---|---|---|
| CTA | Fast, noninvasive, simultaneous bony/vascular/soft tissue detail, 3D reconstruction, widely available | Radiation, iodinated contrast (renal risk), limited soft-tissue contrast vs. MRI |
| MRA | No ionizing radiation, superior soft-tissue contrast | Slower, motion artifact, less bone detail, may overestimate stenosis |
| Conventional angiography | Gold standard for vessel detail, therapeutic (embolization) | Invasive, risk of stroke (~0.5-1%), requires IR suite |
| Doppler ultrasound | Bedside, no radiation, real-time flow assessment | Operator-dependent, limited for deep structures |
| CT (non-angio) | Best bony detail (HRCT temporal bone) | No vascular flow information |
8. Specific Clinical Indications Summary
| ENT Clinical Scenario | Role of CTA |
|---|---|
| Penetrating neck injury (Zones I, III; stable Zone II) | Screening for vascular injury - noninvasive alternative to conventional angiography |
| Blunt neck trauma with neurologic deficit | Detection of carotid/vertebral dissection |
| Temporal bone fracture with neurologic deficit | Evaluate carotid canal injury, carotid artery status |
| Pulsatile tinnitus | CTA/CTV temporal bone - first-line for jugular bulb/sigmoid anomalies and dAVF |
| Paraganglioma (glomus tumor) | Supplementary to CT+MRI; necessary before embolization (but DSA preferred) |
| Head and neck cancer - carotid involvement | Assess resectability, collateral flow |
| Fibular/ALT free flap planning | Confirm vascular anatomy of donor site |
| Carotid artery dissection (Horner syndrome, vertigo) | CTA head/neck - definitive noninvasive diagnosis |
| Oropharyngeal trauma (pediatric) | CTA to evaluate occult vascular injury - systematic review supports its use (PMID: 35561004) |
Recent Evidence
A 2023 systematic review in Laryngoscope (PMID: 35561004) confirmed that CTA guides management in pediatric oropharyngeal trauma, particularly in detecting occult vascular injuries not identified on clinical examination alone. A 2026 review in SA J Radiol examined multimodal imaging including CTA for conductive hearing loss workup (PMID: 41810166).
Key Takeaways
- CTA is the workhorse noninvasive vascular imaging tool in ENT - replacing conventional angiography for screening in most trauma and tumor settings.
- Conventional (DSA) angiography retains superiority where therapeutic intervention (embolization) is planned, especially for paragangliomas and dAVF.
- CTA/CTV of the temporal bone is the first-line study for jugular bulb and sigmoid sinus anomalies causing pulsatile tinnitus.
- In free flap reconstruction, CTA confirms donor-site vascular anatomy and prevents catastrophic harvest complications.
- Combined CT + MRI + CTA provides the most complete picture for skull base and parapharyngeal space lesions.
- The simultaneous extravascular detail (bone, airway, soft tissue) is a unique advantage of CTA in ENT - unavailable with conventional angiography.
Sources: Cummings Otolaryngology Head and Neck Surgery | KJ Lee's Essential Otolaryngology | Shambaugh Surgery of the Ear | Tintinalli's Emergency Medicine
Otitic hydrocephalus
Finding Sources
Finding Sources
Searching PubMed
"otitic hydrocephalus"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading Article
PMID: 39562726
I now have comprehensive, authoritative data from all major ENT textbooks plus recent evidence. Let me compile the full answer.
Otitic Hydrocephalus
Definition and Terminology
Otitic hydrocephalus is the term coined by Symonds (1931) to describe a syndrome associated with otitis media characterized by:
- Increased intracranial pressure (ICP)
- Normal CSF biochemistry and cell count
- No space-occupying lesion or obstruction to CSF flow
- No ventricular dilatation
- Spontaneous recovery tendency
The condition was first described by Quincke in 1897. Because there is no true ventricular dilatation, it is more correctly termed "benign raised intracranial tension" or pseudotumor cerebri - yet the term "otitic hydrocephalus" has persisted in the literature.
It is the rarest of all intracranial complications of ear disease - rarer than meningitis, extradural abscess, subdural empyema, brain abscess, and lateral sinus thrombosis.
"Otitic hydrocephalus is a rare complication of otitis media and stems from either AOM or COM... has a favorable prognosis and is very commonly associated with sigmoid sinus thrombophlebitis."
- Shambaugh Surgery of the Ear
Otologic Source
It may follow:
- Acute otitis media (AOM) - particularly in children
- Chronic otitis media (COM) - with or without cholesteatoma
- Rarely, otologic surgery
It is important to note that the condition is a misnomer in two respects: it can occasionally occur in the absence of active otitis, and there is no true (communicating or obstructive) hydrocephalus.
Pathophysiology
The precise mechanism is not fully established, but the dominant theory (Symonds) involves thrombophlebitis of the dural venous sinuses, as illustrated below:
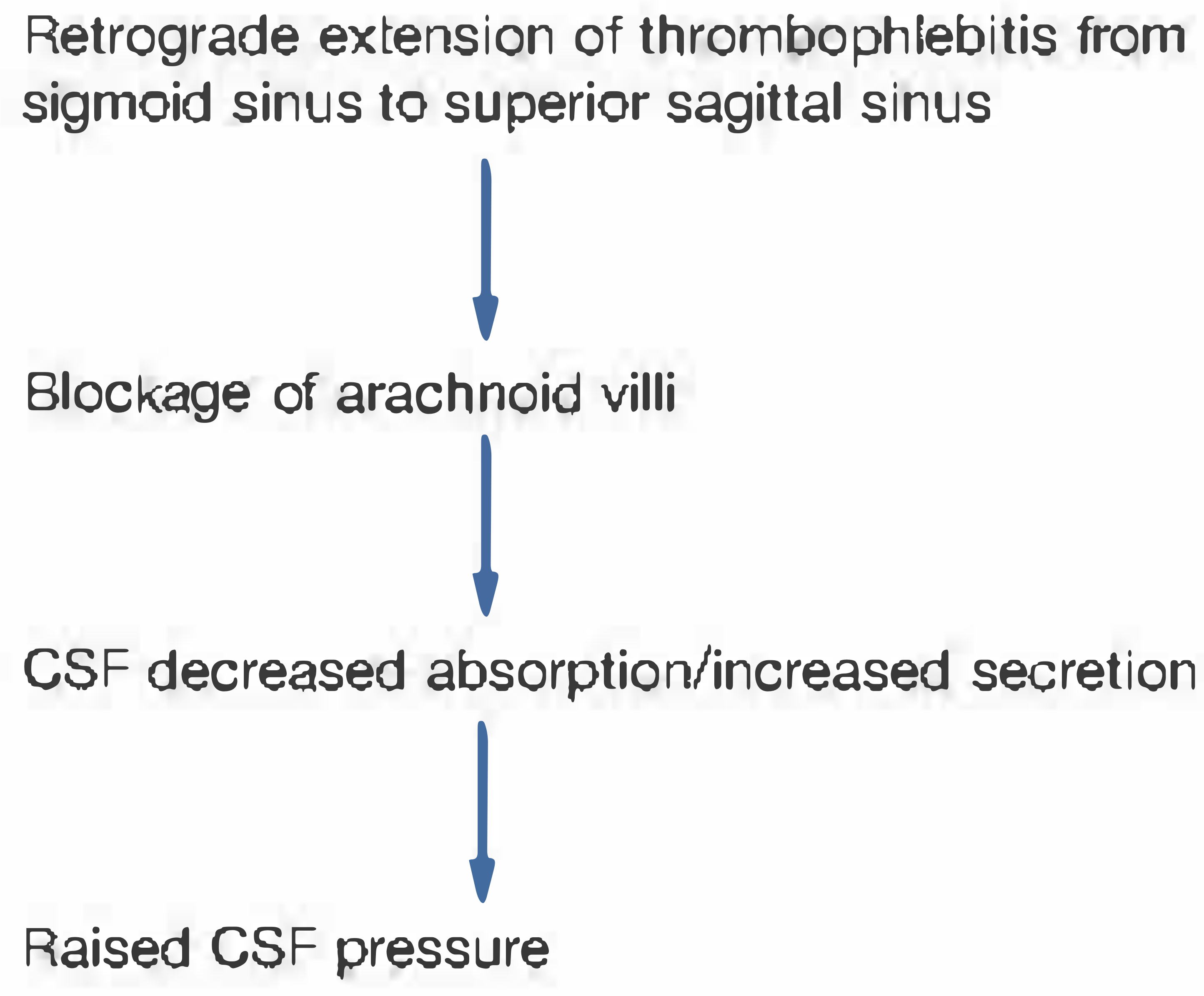
Pathophysiology of otitic hydrocephalus (Symonds' theory) - Shambaugh Surgery of the Ear
The Cascade:
- Otitis media / mastoiditis → septic thrombophlebitis of the sigmoid sinus
- Retrograde propagation to the transverse sinus, inferior petrosal sinus, cavernous sinus, and ultimately the superior sagittal sinus
- Thrombosis of the superior sagittal sinus → blockage of arachnoid granulations (villi)
- Impaired CSF reabsorption → raised intracranial pressure
- No obstruction to CSF circulation → ventricles remain normal in size
Alternative Theories:
- Sahs and Joynt: Brain edema from interstitial mechanisms (brain biopsies show interstitial edema, yet EEG and neurologic function remain normal)
- Weed and Flexner: Disruption of venous circulation causes direct rise in CSF pressure (CSF pressure is directly related to intracranial venous pressure)
- Increased CSF volume theory (separate from absorption impairment)
Determinants of Symptom Development After Lateral Sinus Occlusion (Cummings):
- Relative size of the involved lateral sinus vs. the contralateral side
- Adequacy of the collateral venous network (cavernous sinus, opposite inferior petrosal sinus)
- Likelihood of thrombosis propagating to additional venous outflow channels
Classification - Context Within Intracranial Complications of Otitis
Intracranial complications of otitis media are classified as:
Extradural:
- Extradural abscess
Intradural:
- Leptomeningitis / Meningitis
- Pachymeningitis / Subdural abscess
- Brain abscess
- Otitic hydrocephalus
Venous sinus:
- Lateral (sigmoid) sinus thrombophlebitis - most commonly associated with otitic hydrocephalus
Clinical Features
| Feature | Detail |
|---|---|
| Headache | Dominant symptom - diffuse, severe, persistent |
| Nausea and vomiting | Common |
| Visual disturbance | Blurring of vision, decreased visual acuity |
| Diplopia | Due to VI (abducens) nerve palsy - false localizing sign from raised ICP |
| Drowsiness / lethargy | With progressive elevation of ICP |
| Papilledema | Almost universal - found on fundoscopy; may progress to optic atrophy |
| Photo/phonophobia | May be present |
| Ear disease | Active AOM or COM signs present |
The Classic Triad:
Otitis media + Papilledema + VI nerve palsy (lateral rectus palsy causing horizontal diplopia)
Progression:
- In uncomplicated cases with medical management: headache ameliorates over 3-7 days
- If collateral venous drainage is inadequate: dulling of sensorium, decreased visual acuity from retinal vein occlusion
- Progression to coma and death is possible in severe untreated cases
- Optic atrophy can develop from chronic papilledema - representing a major cause of permanent morbidity
Investigations
1. CT Scan (with IV contrast)
- First investigation in practice - rules out brain abscess, subdural empyema, and other space-occupying lesions
- May show sigmoid/transverse sinus thrombosis as a filling defect ("empty delta sign" on post-contrast CT)
- Ventricles are normal or small - distinguishing it from true hydrocephalus
- CT of mastoids reveals the underlying otologic disease
2. MRI / MR Venography (MRV)
- Modality of choice for definitive assessment - superior evaluation of venous sinuses
- MRV confirms dural sinus thrombosis (sigmoid, transverse, superior sagittal sinus)
- Note: MRV confirms but is not required for the diagnosis of otitic hydrocephalus
- Important to rule out co-existing brain abscess, meningitis, subdural empyema
3. Lumbar Puncture (LP)
- Shows raised CSF opening pressure (often >25 cmH₂O)
- Normal CSF biochemistry: normal glucose, protein, and cell count
- This combination (raised pressure + normal CSF analysis) is the classic finding
- Caution: LP must be performed carefully given risk of cerebellar tonsillar herniation; a CT must be done first to confirm absence of mass lesion
Summary of Typical Findings:
| Investigation | Finding |
|---|---|
| CT head | Normal/small ventricles; may show sinus thrombosis |
| MRI/MRV | Dural sinus thrombosis; no abscess/mass |
| LP - Opening pressure | Raised (>25 cmH₂O) |
| LP - CSF analysis | Normal (protein, glucose, cells) |
| Fundoscopy | Papilledema (93% in recent pediatric series) |
Management
Management is directed at two goals: eradication of ear disease and reduction of raised ICP.
I. Treatment of Ear Disease
| Otologic Cause | Intervention |
|---|---|
| AOM | IV broad-spectrum antibiotics; myringotomy ± tympanostomy tube |
| COM / Cholesteatoma | Mastoidectomy (definitive) |
| No active infection (rare) | Medical treatment alone |
II. Reduction of Raised ICP (Medical)
| Agent | Role |
|---|---|
| Acetazolamide | First-line - carbonic anhydrase inhibitor, reduces CSF production |
| Mannitol | Osmotic diuretic - acute lowering of ICP |
| Corticosteroids | Reduce cerebral edema; important role in papilledema management |
| Diuretics (furosemide) | Adjunct to reduce ICP |
| Fluid restriction | Supportive measure |
III. Surgical / Procedural Options
| Procedure | Indication |
|---|---|
| Mastoidectomy | COM with/without cholesteatoma - source control |
| Sigmoid sinus decompression | Recommended by O'Connor and Moffat |
| Lumbar drainage / Lumbar peritoneal shunt | Recalcitrant/refractory raised ICP |
| Ventriculoperitoneal (VP) shunt | Occasionally required in persistent cases |
| Optic nerve sheath decompression | To prevent optic atrophy in worsening vision |
| Serial ophthalmologic follow-up | Mandatory - to monitor papilledema |
Role of Anticoagulation
- Consider anticoagulation in cases of superior sagittal sinus thrombosis
- Role in sigmoid sinus thrombosis is debated; more recent case series support mastoidectomy + antibiotics without mandatory sinus opening
Prognosis
- Overall favorable prognosis compared to other intracranial complications of otitis
- Most cases resolve with treatment of underlying ear disease and medical ICP management
- Primary morbidity is visual loss from progressive papilledema leading to optic atrophy
- A recent 2025 retrospective study (PMID: 39562726) at a quaternary children's hospital found:
- 93% of 15 patients developed papilledema
- 40% had CN VI palsy
- 73% had progressively worsening papilledema despite improving infection and clot burden
- Systemic corticosteroids significantly improved visual outcomes and helped avoid invasive neurosurgical procedures
- Two patients developed optic atrophy and visual loss before corticosteroids were started - both stabilized after initiation
Key Points to Remember
- Otitic hydrocephalus = raised ICP + normal CSF + no ventricular dilatation - in the setting of ear disease.
- Most commonly follows sigmoid sinus thrombophlebitis from AOM or COM.
- The pathophysiology is blockage of arachnoid villi from retrograde dural sinus thrombosis, impairing CSF reabsorption.
- Classic triad: otitis media + papilledema + VI nerve palsy.
- MRI/MRV is the imaging modality of choice; LP confirms raised pressure with normal CSF.
- Treatment = ear surgery (mastoidectomy) + medical ICP reduction (acetazolamide, mannitol, steroids).
- Optic atrophy is the main long-term morbidity - serial ophthalmologic examination is mandatory.
- Despite the name, it is not true hydrocephalus - ventricles are normal or small.
- It is more accurately called benign intracranial hypertension (pseudotumor cerebri) secondary to otologic disease.
Sources: Shambaugh Surgery of the Ear | Cummings Otolaryngology Head and Neck Surgery | Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2 | KJ Lee's Essential Otolaryngology | Tintinalli's Emergency Medicine | Chen et al., Eye 2025 (PMID: 39562726)
Steps of modified radical mastoidectomy
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have all the information needed to write a comprehensive, step-by-step account of modified radical mastoidectomy from the leading ENT surgical textbooks. Let me compile the full answer.
Steps of Modified Radical Mastoidectomy (MRM)
Definitions and Clarification of Terminology
The term "modified radical mastoidectomy" is used in two distinct ways in the literature:
| Term | Definition |
|---|---|
| Bondy MRM (classical/narrow) | Disease limited to the epitympanum; canal wall partially removed; intact tympanic membrane and ossicular chain preserved; middle ear not entered |
| MRM = canal wall-down (CWD) + tympanoplasty (modern/broad use) | Complete removal of posterior and superior canal walls, exteriorization of all temporal bone disease, with tympanoplasty to seal the middle ear - differs from radical mastoidectomy in that the TM and middle ear are reconstructed rather than abolished |
"Frequently the term modified radical mastoidectomy is used interchangeably with canal wall-down mastoidectomy, which is technically incorrect. Classically, modified radical mastoidectomy refers to the Bondy procedure... [however] modified radical mastoidectomy, also known as complete mastoidectomy and tympanoplasty, is an evolutionary surgical development that attempts to incorporate the major goal of cholesteatoma surgery (i.e., exteriorization of disease) with sealing of the middle ear space."
- Cummings Otolaryngology / Shambaugh Surgery of the Ear
The steps below describe the modern MRM (canal wall-down mastoidectomy + tympanoplasty) - the procedure most commonly taught and practiced.
Indications
Absolute Indications
- Cholesteatoma with extensive involvement of the attic, antrum, and mastoid
- Labyrinthine fistula
- Only hearing ear (single-stage clearance preferred)
- Failed previous canal wall-up procedure
- Patient unable or unwilling to attend for second-look surgery
- Occasional otologic surgeon (less experience with canal wall-up technique)
Relative / Intraoperative Indications
- Low-lying middle cranial fossa dura limiting access
- Anteriorly positioned sigmoid sinus creating a small mastoid cavity
- Extensive posterior canal wall destruction by cholesteatoma
- Poor Eustachian tube function (increases recurrence risk with canal wall-up)
- Age: elderly patients, poor anaesthetic risk
Instruments Required
- Operating microscope
- Continuous facial nerve monitor
- Electric drill with cutting burrs (large, medium) and diamond burrs (fine)
- Constant irrigation
- Suction
- Microforceps, right-angle hooks, whirlybird dissectors
- Micromirrors and/or surgical telescopes
- Rongeur
- Iris scissors (for meatoplasty)
STEP-BY-STEP PROCEDURE
STEP 1 - Preoperative Preparation
- Pre-op ear toilet: Active suppuration controlled with 1.5% acetic acid irrigations (1 part white vinegar: 2 parts boiled water) 2-4 times/day + antibiotic otic drops for several weeks
- Radiologic assessment: HRCT temporal bone - assesses scutum erosion, mastoid sclerosis, extent of cholesteatoma, proximity to facial canal, semicircular canals, sigmoid sinus, tegmen, and cochlea
- Audiogram: Pure tone audiogram mandatory before surgery
- Anaesthesia: General anaesthesia with endotracheal intubation; facial nerve monitor electrodes placed
STEP 2 - Patient Positioning and Skin Preparation
- Patient supine, head turned to opposite side, with affected ear uppermost
- Shave 1-2 cm of hair around the auricle
- Prep and drape in standard surgical fashion
STEP 3 - Local Anaesthetic Infiltration
- Inject 5-10 mL of 1% lidocaine with 1:100,000 epinephrine postauricularly and into the external ear canal
- Purpose: vasoconstriction (hemostasis) + postoperative analgesia
- Allow 10 minutes for full vasoconstriction
STEP 4 - Incision (Postauricular Approach)
- C-shaped postauricular incision placed approximately 1 cm behind the postauricular crease (placed more posteriorly than usual to facilitate subsequent saucerization and skin closure)
- Superiorly: incision carried down to the temporalis fascia (harvest site for graft)
- Temporalis fascia harvested at this stage (will be used for tympanoplasty graft)
- Inferiorly: extended to the anterolateral surface of the mastoid tip
"To facilitate closure, the C-shaped incision is placed about 1 cm behind the postauricular crease." - Cummings
STEP 5 - Periosteal Elevation and Exposure of the Mastoid Cortex
- Two periosteal incisions:
- Along the temporal line (superior)
- Perpendicular to the temporal line, extending to the mastoid tip
- Periosteum elevated using a broad periosteal elevator, retracted forward with the auricle
- Self-retaining retractor (Weitlaner or Shambaugh endaural retractor) inserted
- Full exposure of the mastoid cortex from the posterior root of the zygomatic process to 2-3 cm posterior to the suprameatal spine of Henle, and from the temporal line to the mastoid tip is essential
STEP 6 - External Auditory Canal Elevation (Tympanomeatal Flap)
- Under the operating microscope, tympanomeatal flap raised by making canal incisions:
- Posterior canal skin elevated from 6 o'clock to 12 o'clock position
- House #2 knife used to elevate the inferior flap to the fibrous annulus
- Tympanic membrane inspected; its relationship to disease assessed
- Annulus freed from the sulcus tympanicus; middle ear entered from below
STEP 7 - Cortical Mastoidectomy (Simple Mastoidectomy First)
- Begin with a large cutting burr along the temporal line (first burr cut), approximating the middle cranial fossa floor level
- Second burr cut perpendicular to the temporal line, tangential to the bony external canal, carried inferiorly to the mastoid tip
- Key principle: "Always leave the canal wall up" initially, except in the most contracted mastoid cavities
- Exenterate mastoid air cells systematically, exposing:
- Middle cranial fossa (tegmen) dural plate - superiorly
- Posterior fossa dural plate - posteriorly
- Sigmoid sinus - posteriorly
- Digastric ridge - inferiorly (marks the inferior extent of dissection and approximate level of the facial nerve)
- Bony posterior canal wall - anteriorly
- The mastoid antrum is identified by following the temporal line medially
- Identify the short process of the incus (fossa incudis) and the dome of the lateral semicircular canal (LSCC) - key landmarks
- Cholesteatoma and granulations filling the central mastoid tract can be removed at this stage

Modified radical mastoid cavity - Shambaugh Surgery of the Ear
STEP 8 - Identification of the Facial Nerve and Facial Recess
- Facial nerve identification is mandatory before taking down the canal wall
- Identify the vertical (mastoid) segment using two landmarks: digastric ridge below and LSCC above
- Diamond burr used (never cutting burr) to skeletonize the facial canal
- Open the facial recess (posterior tympanotomy): the triangular space bounded by:
- Medially: facial nerve
- Laterally: chorda tympani nerve
- Superiorly: incus buttress (fossa incudis)
- This gives access to the oval window, round window, and middle ear from behind
STEP 9 - Ossicular Management
- If the incus is involved with cholesteatoma: the incudostapedial joint is identified through the facial recess, divided with a joint knife, and the incus removed
- Removing the incus first reduces potential for trauma during subsequent canal wall takedown
- The malleus head may be retained (if free of disease) for later ossicular reconstruction, or removed by cutting the tensor tympani tendon at the cochleariform process
- Stapes is preserved whenever possible - it is the goal of the modified procedure to leave the stapes as the only remaining ossicle
- Chorda tympani nerve: sacrificed in the course of lowering the facial ridge (unavoidable in MRM)
STEP 10 - Canal Wall Takedown (Posterior and Superior)
This is the defining step of canal wall-down surgery:
Posterior canal wall:
- The posterior bony canal wall is taken down using a rongeur (or burr) after facial nerve identification
- Removal proceeds from superior to inferior, and from lateral to medial
- The facial ridge (posterior canal wall remnant above the facial nerve) is lowered to the level of the fallopian canal using a diamond burr
- Goal: the facial ridge should be as low as possible - only a thin layer of bone remains over the vertical facial nerve
Superior canal wall (anterior buttress and posterior buttress):
- The anterior buttress (where posterior bony canal wall meets the tegmen) is completely removed to achieve smooth continuity between the mastoid tegmen and tegmen tympani
- The posterior buttress (meeting of posterior canal wall and floor of EAC, lateral to facial nerve) is also removed
- The anterior epitympanum is drilled down to become continuous with the anterior canal wall
Inferior canal wall:
- The inferior canal wall must be drilled away until the inferior canal wall and mastoid tip are confluent with no bony overhang
"An important landmark is the anterior buttress, which is totally removed to achieve a smooth continuum between the mastoid tegmen and the tegmen tympani." - Shambaugh Surgery of the Ear
STEP 11 - Disease Clearance
- With the full cavity now exposed, all cholesteatoma matrix and sac systematically removed
- Particularly difficult areas: sinus tympani (behind the stapes), supratubal recess, anterior epitympanum, hypotympanum
- If disease extends into the sinus tympani: pyramidal eminence can be removed with a small diamond burr (only if stapes is absent)
- Tools to aid clearance in difficult areas: right-angle hooks, whirlybird dissectors, micromirrors, 30° and 70° surgical telescopes
- Labyrinthine fistula (if present): medial cholesteatoma matrix left on the fistula, not aggressively dissected
- Disease removed from the oval window region and horizontal segment of facial nerve
Caution: Tympanoplasty should not be performed if there is any question of residual cholesteatoma in the sinus tympani or hypotympanum.
STEP 12 - Saucerization and Cavity Refinement
- At completion of disease clearance, copious irrigation to lower bacterial count and aid hemostasis
- The cavity is saucerized to create a smooth-walled, ovoid/rectangular shape with:
- No overhanging ridges
- No ledges or concave bony irregularities
- A low facial ridge
- Smooth transition from mastoid to ear canal
- The cavity contour must allow free epithelial migration and self-cleaning postoperatively
- Particularly important: saucerization of the mastoid tip and posteroinferior cell tracts
"The cavity should approach an ovoid or rectangular shape with the facial ridge low... This attention to detail helps ensure soft tissue obliteration of much of the cavity space." - Shambaugh Surgery of the Ear
Scott-Brown emphasizes: cavity problems result from:
- High facial ridge
- Sump below floor of EAC
- Tympanic membrane perforation
- Small external meatus - all preventable with good technique
STEP 13 - Meatoplasty
- 1% lidocaine with 1:100,000 epinephrine infiltrated into the conchal bowl
- Posterior conchal cartilage excised: using iris scissors through fibrous periosteum and soft tissue, a semilunar (crescent-shaped) incision made into the cartilage posteriorly until the knife tip is felt through anterior skin
- Crescent-shaped cartilage measures approximately 1.5 × 2 cm
- This enlarges the external meatus to a size proportionate to the mastoid cavity
- The excised conchal cartilage can be used to partially obliterate the cavity
- A widely patent meatus is essential for postoperative cleaning and cavity maintenance
"The meatus should be an adequate size relative to the size of the cavity, so a meatoplasty is almost always required." - Scott-Brown's Otorhinolaryngology
STEP 14 - Körner's Flap (Meatal Skin Flap)
- Körner's flap developed from the external auditory canal skin:
- Inferior incision: begins in the inferior canal at 6 o'clock, carried into the conchal bowl, and curved around the inferior margin
- Superior incision: made at 12 o'clock and carried between tragus and anterior helix
- These incisions create a long posterosuperiorly based vascular strip flap
- This flap will form the back wall (posterior lining) of the mastoid cavity
- The auricle and flap are retracted anteriorly to expose the mastoid and middle ear
STEP 15 - Tympanoplasty (Grafting)
- Middle ear and Eustachian tube packed with saline-moistened absorbable gelatin sponge (Gelfoam) to the level of the anterior annulus - supports the graft and prevents graft medialization
- Temporalis fascia graft (harvested at Step 4) placed:
- Medial to the anterior annulus and drum remnant
- Extending over the stapes (if present) to the facial ridge into the mastoid
- Graft must lie flat - no folds
- If the stapes is present: graft placed directly atop the stapes superstructure
- Ossicular reconstruction (if feasible):
- With intact stapes capitulum: a malleus head goblet prosthesis can be placed atop the capitulum
- Without stapes: total ossicular replacement prosthesis (TORP) using autologous tissue preferred over alloplastic material
- Graft surface covered with antibiotic ophthalmic ointment (polymixin B + bacitracin)
STEP 16 - Securing the Körner's Flap and Closure
- Körner's flap sutured to the musculoperiosteum at the edge of the mastoid cavity using 3.0 polyglactin (Vicryl) sutures subdermally at both edges
- Tension adjusted until the meatus has the desired circular shape
- Overtightening the superior suture must be avoided - causes protruding auricle
- Postauricular wound closed in layers with subcuticular absorbable suture
- Mastoid bowl filled with antibiotic ointment or packed with bismuth iodoform paraffin paste (BIPP) gauze
- Mastoid pressure dressing applied
Summary of the Ten Key Principles
| Principle | Rationale |
|---|---|
| Complete air cell exenteration | Eliminates residual mucosa that would cause drainage |
| Low facial ridge | Allows epithelial migration and cavity self-cleaning |
| Removal of anterior + posterior buttress | Smooth cavity continuum, no overhanging bone |
| Adequate saucerization | No ledges, no sumps, no retentive areas |
| Adequate meatoplasty | Size of meatus must match cavity size |
| Tympanoplasty (sealing middle ear) | Prevents discharge from exposed middle ear mucosa |
| Körner's flap | Lines the mastoid cavity, promotes epithelialization |
| Facial nerve identification first | Prevents catastrophic injury during canal wall takedown |
| Cholesteatoma matrix removed in full | Prevents residual/recurrent disease |
| Stapes preservation | Enables hearing reconstruction |
MRM vs. Radical Mastoidectomy - Key Differences
| Feature | Radical Mastoidectomy | Modified Radical Mastoidectomy |
|---|---|---|
| Canal wall | Removed | Removed |
| TM | Sacrificed | Reconstructed (tympanoplasty) |
| Ossicles | Removed (except stapes footplate) | Stapes preserved; reconstruction attempted |
| Eustachian tube | Obliterated | Preserved/functional |
| Middle ear | Exteriorized into cavity | Sealed from mastoid cavity |
| Hearing | Not addressed | Preserved / reconstructed |
| Cavity discharge | Chronic from exposed mucosa | Reduced (mucosa sealed off) |
Postoperative Care
- Mastoid dressing removed on day 1; postauricular dressing on day 2
- Cotton in meatus changed frequently for first week (significant drainage expected)
- Ear kept dry; nose blowing avoided
- First postoperative visit at 2-3 weeks
- Granulation tissue debrided and treated with silver nitrate (not near exposed facial nerve)
- Serial audiogram at 6 weeks
- Long-term: regular cavity cleaning in clinic (every 6-12 months); cavity requires 1-3 months for complete epithelialization
Complications
| Complication | Notes |
|---|---|
| Facial nerve palsy | Most feared; prevented by identification before canal wall takedown |
| Sensorineural hearing loss | From drill trauma or labyrinthine injury |
| Labyrinthine fistula | Lateral semicircular canal most common |
| Persistent/recurrent cholesteatoma | Especially in sinus tympani (5-15% CWD rate) |
| Chronic discharging cavity | 20-25% long-term; reduced with good technique |
| Caloric vertigo | From water/wind exposure over bare LSCC |
| Meatal stenosis | Inadequate meatoplasty |
| Graft failure | Tympanoplasty breakdown |
| Chorda tympani injury | Taste disturbance (unavoidable in MRM) |
Sources: Shambaugh Surgery of the Ear | Cummings Otolaryngology Head and Neck Surgery | Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2
Stereotactic radio surgery
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Pan endoscopy
Finding Sources
Finding Sources
Searching PubMed
"panendoscopy" AND "head and neck"
Reading File
Reading File
Reading File
Reading Article
PMID: 39957633
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from all the key sources. Let me compile the full, detailed answer.
Panendoscopy
Definition
Panendoscopy (also called triple endoscopy or quadruple endoscopy) is the combined endoscopic examination of the entire upper aerodigestive tract - including the larynx, trachea, bronchi, hypopharynx, esophagus, and nasopharynx - performed as a single procedure, classically under general anaesthesia.
"Panendoscopy, sometimes known as triple endoscopy, involves three diagnostic components: laryngoscopy, bronchoscopy, and esophagoscopy."
- Miller's Anesthesia
Components
| Component | Structures Examined |
|---|---|
| Direct laryngoscopy (microlaryngoscopy) | Larynx, supraglottis, glottis, subglottis, hypopharynx, base of tongue, vallecula, piriform fossae |
| Rigid bronchoscopy (or flexible) | Trachea, carina, main bronchi, lobar orifices |
| Rigid oesophagoscopy (or flexible) | Cricopharynx, cervical and thoracic oesophagus to the gastro-oesophageal junction |
| + Nasopharyngoscopy (when added = "quadruple endoscopy") | Post-nasal space, Eustachian tube orifices, adenoid pad |
Indications
1. Head and Neck Cancer - Staging and Disease Extent
The primary indication for panendoscopy in ENT practice:
- Staging of known head and neck squamous cell carcinoma (HNSCC) - to define the full extent of disease before treatment planning
- Biopsy of suspected or confirmed primary lesions for histopathologic diagnosis
- Assessment of lesions not accessible under office conditions (tongue base, inferior tonsil, posterior oropharyngeal wall, subglottis, pyriform sinus apex, post-cricoid region)
- Assess resectability - involvement of larynx, trachea, oesophagus, and hypopharynx
"Panendoscopy under general anesthesia is an important tool not only to detect lesions, define their extent, and biopsy them but also to rule out any secondary malignancy."
- Cummings Otolaryngology
2. Detection of Synchronous Second Primary Tumours (SSPCA)
A major justification for panendoscopy historically:
- Patients with HNSCC have a field cancerization effect - chronic mucosal exposure to carcinogens (tobacco, alcohol) predisposes the entire aerodigestive tract mucosa to malignant transformation
- Second primary tumours may occur synchronously in the oesophagus, bronchus, or another head and neck site
- A large meta-analysis found a small but significant advantage to panendoscopy in detection of second primary tumours in prospective studies
However, this indication is now contested (see Evidence section below):
- Panendoscopy is currently only recommended for symptomatic patients or patients with primary tumours known to have a significant risk of a synchronous primary - not as a routine for all HNSCC
- Appropriate symptom-directed investigations + routine chest imaging achieve similar detection rates and avoid unnecessary risk/expense in asymptomatic patients
3. Unknown Primary of the Head and Neck (Carcinoma of Unknown Primary - CUP)
One of the most important current indications:
- When a patient presents with cervical lymph node metastasis from SCC with no identifiable primary on clinical examination or imaging
- Panendoscopy with directed biopsies, ipsilateral tonsillectomy, and examination of the tongue base and nasopharynx
- The oropharynx (tongue base, palatine tonsil) is the most common site of occult primary in CUP of the head and neck
- PET-CT should be performed before panendoscopy and biopsies (post-biopsy inflammatory response increases FDG uptake and confounds interpretation)
- Traditional panendoscopy with directed biopsies identified primary in ~25% of CUP cases; newer techniques (TLM, TORS with lingual tonsillectomy) achieve detection rates of 89-94%
- HPV/p16 status of FNA material should be tested pre-procedure: p16-positive SCC in cervical nodes reliably predicts oropharyngeal origin and guides targeted biopsy/tonsillectomy
4. Monitoring and Surveillance
- Assessment for recurrence after treatment of head and neck cancer
- Monitoring vocal cord lesions, papillomatosis
- Evaluating treatment response
5. Therapeutic Procedures
- Microlaryngoscopy with laser treatment (papilloma, early glottic carcinoma, stenosis)
- Oesophageal foreign body removal
- Balloon dilatation of stenoses
- Injection procedures (vocal cord augmentation, Botulinum toxin)
- Tracheo-oesophageal puncture (voice prosthesis)
6. Other ENT Indications
- Dysphagia of unknown cause (hypopharyngeal/oesophageal assessment)
- Globus sensation
- Laryngopharyngeal reflux assessment and monitoring
- Airway assessment prior to major head and neck surgery
- Suspected subglottic or tracheal stenosis
Contraindications
| Absolute | Relative |
|---|---|
| Unstable cervical spine | Poor general anaesthetic risk |
| Severe ankylosing spondylitis preventing neck extension | Severe coagulopathy (correct before procedure) |
| Acute severe respiratory failure | Active myocardial ischaemia |
| Known thoracic aortic aneurysm (rigid oesophagoscopy) | Recent oesophageal surgery |
Preoperative Assessment
- Clinical history and examination: full head and neck examination including flexible nasopharyngoscopy in clinic
- Imaging first: CT neck and chest (or PET-CT) - must be performed before panendoscopy and biopsy; imaging upstaging from biopsy oedema is a real concern
- Audiogram and voice assessment where indicated
- Dental review: to protect dentition during laryngoscopy (use dental guard)
- Anaesthetic assessment: airway review is critical - disease may compromise intubation
- Informed consent: explaining specific risks including dental injury, lip laceration, voice change, oesophageal/tracheal injury, and (rarely) death
Anaesthesia
Panendoscopy requires specific anaesthetic planning and surgeon-anaesthetist communication. The key questions are:
- How does the pathology affect intubation/ventilation?
- What airway management plan will allow the surgeon adequate access?
- What co-existing disease (COPD, IHD, GORD, OSA) needs optimisation?
Patient Position
- Supine, neck flexed, head extended ("Jackson position" = "sniffing position")
- Shoulder roll beneath the shoulders
- Head ring to support the extended head
Five Airway Options for Panendoscopy (Miller's Anesthesia):
| Option | Details | Best For |
|---|---|---|
| 1. MLT endotracheal tube | Narrow-bore microlaryngeal tube (5.0 mm ID) - most common | Standard cases; provides airway protection and ETCO₂ monitoring |
| 2. Jet ventilation (+ rigid laryngoscope) | No ETT; requires TIVA (propofol + remifentanil infusion) | Optimal laryngeal access; anterior commissure pathology |
| 3. Hybrid methods | Intermittent SGA, MLT + jet ventilation, or intermittent apnoea | Selected complex cases |
| 4. Tracheostomy under local anaesthesia | Prior to GA induction | Anticipated severely difficult airway; significant airway compromise |
| 5. Transtracheal jet cannula (Ravussin catheter) | Placed before induction | Selected anticipated difficult airway |
- When laser surgery is combined with panendoscopy: a laser-safe ETT is mandatory
- When jet ventilation is used: TIVA is required (no volatile anaesthetic delivery possible without an ETT)
- Most common standard technique: GA + muscle relaxation + MLT tube - familiar, provides airway protection, allows volatile anaesthetics and reliable ETCO₂
Procedure - Step by Step
Step 1 - Direct Laryngoscopy (Microlaryngoscopy)
- Anterior commissure laryngoscope (Kleinsasser) or Dedo laryngoscope introduced
- Suspended in position using a chest support - frees both surgeon hands
- Operating microscope brought into position
- Systematic examination:
- Epiglottis, aryepiglottic folds
- False cords, laryngeal ventricles
- True vocal cords - anterior commissure, posterior commissure
- Subglottis
- Piriform fossae (posterior retraction of the scope)
- Post-cricoid region
- Vallecula, base of tongue
- Biopsies taken from suspicious lesions with microlaryngeal cup forceps
- Cold steel or laser excision/ablation performed as required
- Photographic documentation of all findings
Step 2 - Rigid Bronchoscopy (if indicated)
- Laryngoscope replaced by ventilating rigid bronchoscope
- Inserted through the larynx under direct vision
- Examination of: trachea, carina, right and left main bronchi, lobar bronchial orifices
- Biopsy of any endobronchial lesions
- In modern practice, often replaced by flexible bronchoscopy or CT chest alone in asymptomatic patients
Step 3 - Rigid Oesophagoscopy
- Patient's head repositioned: neck flexed (chin down) to align the cricopharyngeal inlet
- Rigid oesophagoscope introduced carefully through the right side of the mouth, passed behind the larynx under direct vision
- Advance through the cricopharyngeal sphincter (Killian's dehiscence area is a point of risk)
- Systematic examination:
- Cricopharynx, upper oesophagus
- Mid-oesophagus
- Lower oesophagus to the gastro-oesophageal junction
- Biopsy of mucosal abnormalities
- Note: right-angle scope illumination allows examination of mucosal walls
Step 4 - Nasopharyngoscopy (if performing quadruple endoscopy)
- Rigid 0° or 30° nasal endoscope
- Examination of: nasopharynx, post-nasal space, Eustachian tube orifices, adenoid pad
- Biopsy of any suspicious post-nasal space lesions
Biopsies and Documentation
- Diagrammatic representation of all lesions is mandatory (with photographs/videos)
- Multiple directed biopsies from suspicious sites, including apparently normal mucosa in high-risk areas (tongue base, tonsillar fossa in CUP)
- In CUP: ipsilateral tonsillectomy performed at same sitting to maximise detection rate
- Frozen sections may be used intraoperatively to confirm malignancy or assess margins
Office-Based (Awake Unsedated) Panendoscopy
Modern practice has introduced transnasal oesophagoscopy (TNO) and awake flexible panendoscopy in the office setting:
- Performed with distal-chip flexible endoscopes (outer diameter 3.1-5.3 mm) with working channel (2 mm) for suction, biopsy forceps, or laser fibre
- Topical anaesthesia only (no sedation or GA)
- Nil by mouth 3 hours pre-procedure
- Advantages: avoids hospital admission, avoids GA, immediate results, biopsy still possible
- Limitations: no rigid laryngoscopy; bronchoscopic evaluation generally not performed (replaced by high-resolution CT)
- Diagnostic accuracy equivalent to conventional endoscopy in skilled hands for oesophageal assessment
- Suitable for: small vocal fold tumours, laryngopharyngeal reflux, Barrett's oesophagus surveillance, head and neck cancer surveillance
Complications
| Complication | Notes |
|---|---|
| Dental injury | Most common; dental guard protects dentition |
| Lip/gum laceration | Poor positioning or instrument technique |
| Tongue numbness | Hypoglossal nerve compression by laryngoscope |
| Oesophageal perforation | Most serious of oesophagoscopy; ~0.1-0.3%; cervical oesophagus at greatest risk |
| Tracheal/bronchial injury | Rare; usually from rigid bronchoscope |
| Laryngeal/vocal cord trauma | Voice change, granuloma formation |
| Aspiration | Especially in patients with swallowing dysfunction |
| Haemorrhage | From biopsy sites; usually self-limiting |
| Jaw/TMJ injury | In rigid laryngoscopy with limited mouth opening |
| Hypoxia/respiratory compromise | From airway instrumentation in compromised airways |
| Death | Extremely rare; ~0.7% major complication rate overall |
Current Evidence on Routine Panendoscopy
The most recent systematic review (Bellavance et al., J Otolaryngol Head Neck Surg, 2025 - PMID: 39957633) analysed 51 studies (n = 19,914 patients):
| Finding | Data |
|---|---|
| Overall SSPCA detection rate | 6.4% of all panendoscopies (467/7262) |
| Change in management if prior CT neck + chest | Only 1.1% of cases (3/268) |
| Change in management if prior PET-CT | 0% (0/544) |
| Major complication rate | 0.7% (58/8386) |
| Cost (private US healthcare) | $3,802 - $17,296 USD per procedure |
Conclusion: Routine panendoscopy adds minimal value when CT neck + chest or PET-CT has already been performed. It should be reserved for confirming suspicious findings from initial imaging - not performed systematically in all HNSCC patients.
Panendoscopy vs. Modern Alternatives - Summary
| Approach | Advantage | Limitation |
|---|---|---|
| Routine panendoscopy | Comprehensive single-session evaluation; biopsy capability | GA risk; cost; low yield if modern imaging done |
| CT neck + chest | Non-invasive; detects SSPCA and distant mets | Cannot biopsy; misses mucosal lesions |
| PET-CT | Highest sensitivity for SSPCA and distant metastasis; guides panendoscopy | Cost; false positives in tonsils (15-39%) |
| Transnasal office endoscopy (TNO) | No GA; immediate; low risk | Limited to flexible; no rigid bronchoscopy |
| TORS/TLM for CUP | 89-94% detection rate for occult primary | Requires expertise; theatre-based |
Key Points to Remember
- Panendoscopy = laryngoscopy + bronchoscopy + oesophagoscopy ± nasopharyngoscopy, under GA.
- Primary indications: staging HNSCC, biopsy, CUP workup, surveillance.
- Not routinely recommended for SSPCA detection if CT chest/neck or PET-CT already performed.
- For CUP: always perform PET-CT first (before biopsies); panendoscopy with ipsilateral tonsillectomy + directed biopsies; newer TORS/TLM achieves much higher detection.
- Anaesthesia requires careful surgeon-anaesthetist planning - 5 airway options available; MLT tube most common; jet ventilation for anterior commissure access; laser-safe ETT for laser cases.
- Jackson position (neck flexed, head extended) used for rigid instruments.
- TIVA required when jet ventilation is used (no volatile anaesthetic delivery).
- Major complication rate of panendoscopy is low (0.7%) but cost burden is significant.
- Office-based TNO is an increasingly viable alternative for selected patients.
- Imaging must precede biopsy - post-biopsy oedema confounds CT/MRI staging and FDG uptake on PET.
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery | Cummings Otolaryngology Head and Neck Surgery | Miller's Anesthesia 10th ed | Bellavance et al., J Otolaryngol Head Neck Surg 2025 (PMID: 39957633)
Rhinolith
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.