AWARENESS UNDER ANESTHESIA. DEPTH OF ANESTHESIA MONITORING
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Now I have comprehensive information from multiple authoritative anesthesia textbooks. Let me compile the complete answer.
Awareness Under Anesthesia & Depth of Anesthesia Monitoring
1. Definition and Scope
Intraoperative awareness occurs when a patient under general anesthesia regains consciousness and retains recall of intraoperative events. It ranges from mild anxiety to full explicit memory of surgical events, pain, and paralysis, with sequelae that can include posttraumatic stress disorder (PTSD), sleep disturbances, nightmares, and social difficulties.
The problem is deeply feared by patients: a continuing series of media reports has imprinted the fear of awareness in the general population, and it has become a primary patient concern before surgery. — Morgan and Mikhail's Clinical Anesthesiology, 7e
2. Incidence
| Population | Incidence of Awareness |
|---|---|
| General elective surgery (adults) | ~0.1–0.2% |
| Children undergoing elective surgery | 0.0025–0.1% |
| Major trauma surgery (early studies) | Up to 43% |
| Cardiac surgery | ~1.5% |
| Cesarean section | ~0.4% |
| ASA Closed Claims database | ~2% of all claims |
| NHS Litigation Authority (1995–2007) | 19/93 relevant claims = "awake paralysis" |
— Morgan and Mikhail's Clinical Anesthesiology, 7e; Barash Clinical Anesthesia, 9e
3. High-Risk Situations
Several clinical scenarios predispose to awareness:
- Major trauma surgery — reduced anesthetic doses may be required hemodynamically
- Cardiac surgery and cardiopulmonary bypass (CPB)
- Cesarean section under general anesthesia
- Total intravenous anesthesia (TIVA) — dose-response curve is less consistent than inhaled agents; unrecognized IV access loss can result in awareness
- Neuromuscular blockade (NMB) — abolishes movement as a clinical sign; NMB agents have been implicated in contributing to accidental awareness
- Long-term substance abuse — increased anesthetic requirements may go unmet
- Equipment malfunction — vaporizer failure, medication errors, mislabeling
"Lack of cortical arousal cannot be ensured by hemodynamic monitoring, as there can be a discordance between sympathetic response to stimulus and awareness of that stimulus." — Sabiston Textbook of Surgery, 11e
4. Clinical Signs of Inadequate Anesthetic Depth
Traditional indicators of inadequate depth (used when no processed EEG monitoring is available):
- Movement in non-paralyzed patients (most reliable clinical sign)
- Tachycardia, hypertension (sympathetic activation)
- Sweating, lacrimation, pupillary dilation
- Increased respiratory rate in spontaneously breathing patients
Limitations: Hemodynamic monitoring alone is unreliable. Movement can represent spinal reflexes without cortical consciousness, and is absent in paralyzed patients.
5. Depth of Anesthesia Monitoring
a. Minimum Alveolar Concentration (MAC)
For volatile anesthetics, maintaining an age-adjusted end-tidal MAC ≥ 0.7 reduces awareness risk. MAC monitoring is practical, well-validated, and broadly accessible. It is used as the comparator standard in awareness trials.
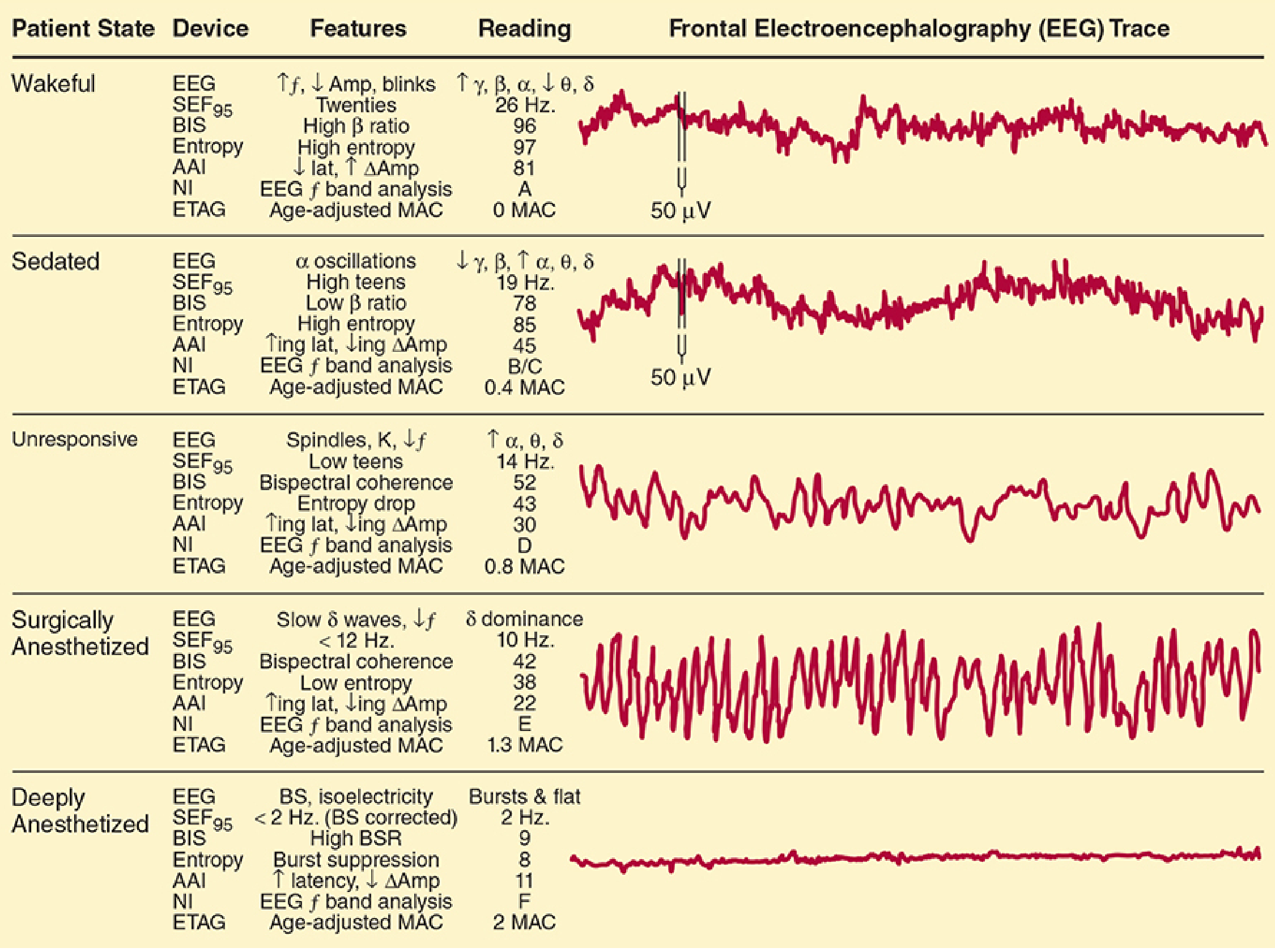
b. Electroencephalography (EEG)
The EEG records surface cortical activity. As anesthesia deepens:
- Beta activation (fast waves) → light anesthesia
- Slowing (delta/theta waves) → deep anesthesia
- Burst suppression → very deep
- Isoelectricity → maximal suppression
Raw multichannel EEG is cumbersome in the OR and is typically processed into a dimensionless index (0–100 scale):
| Monitor | Manufacturer | Signal | Anesthesia Target Range |
|---|---|---|---|
| BIS (Bispectral Index) | Aspect Medical Systems | Single-channel EEG | 40–60 |
| PSI (Patient State Index) | Physiometric / PSA 4000 | 4-channel EEG | 25–50 |
| Narcotrend | Monitor-Techniks | 1–2 channel EEG | D₂–C (index ~40–60) |
| Entropy (SE/RE) | Datex-Ohmeda / GE | Single-channel EEG + EMG | 40–60 |
| AAI (A-Line ARX Index) | Danmeter | Auditory evoked potentials | 15–25 |
| SedLine | Masimo | Processed EEG spectrogram | — |
— Morgan and Mikhail's Clinical Anesthesiology, 7e, Table 6–1
Below is the referenced EEG figure from Morgan & Mikhail showing EEG traces across patient states and corresponding monitoring values:
c. Bispectral Index (BIS) — The Most Studied Monitor
BIS analyzes four EEG components:
- Low-frequency activity (deep anesthesia)
- High-frequency beta activation (light anesthesia)
- Suppressed EEG waves
- Burst suppression ratio
BIS score:
- 100 = fully awake
- 60–80 = sedation
- 40–60 = general anesthesia (target range)
- <40 = deep hypnosis / approaching burst suppression
- 0 = flat/isoelectric EEG
Clinical evidence for BIS:
- Three randomized trials showed BIS helps prevent awareness in high-risk populations (cardiac surgery, TIVA)
- For volatile anesthetic-based anesthesia, BIS has not been shown superior to end-tidal MAC protocols in preventing awareness
- For TIVA, processed EEG (including BIS) is particularly beneficial as there is no gas monitoring equivalent
- BIS may also prevent anesthetic overdose by signaling complete cortical suppression
— Sabiston Textbook of Surgery, 11e; Miller's Anesthesia, 10e; Morgan & Mikhail, 7e
d. EEG Limitations
- Hypothermia reduces EEG activity independently of anesthetic depth
- Certain IV agents (e.g., ketamine, nitrous oxide) produce atypical EEG patterns
- EEG measures only cortical activity — subcortical or embolic injury can go undetected
- Pediatric patients: processed EEG monitors are less reliable at certain developmental stages; SedLine spectrograms may offer some advantage
- The ASA has not adopted awareness monitors as a universal standard of care
6. Prevention Strategies
- Maintain end-tidal MAC ≥ 0.7 (age-adjusted) with volatile agents
- Use processed EEG monitoring (BIS/SedLine) — mandatory for TIVA, beneficial for high-risk cases
- Avoid sole reliance on hemodynamic signs for depth assessment
- Administer benzodiazepines or scopolamine when volatile agents cannot be used at amnestic concentrations
- Check equipment (vaporizer function, IV line patency during TIVA)
- NMB monitoring — always use when neuromuscular blockers are given; residual paralysis masks awareness
- Document end-tidal anesthetic concentrations and amnesic drug doses
7. Management of Suspected or Confirmed Awareness
If intraoperative awareness is detected or suspected:
- Immediately deepen anesthesia (bolus propofol 1–2 mg/kg is practical)
- Add a benzodiazepine for amnesia if not contraindicated
- Postoperatively: obtain a detailed account, answer patient questions empathetically, refer for psychological counseling if appropriate
- Most patients who report awareness are dissatisfied with how their concerns are addressed — communication is critical
"Most patients reporting awareness are dissatisfied with the manner in which their concerns are addressed." — North American Anaesthesia Awareness Registry, cited in Morgan and Mikhail's Clinical Anesthesiology, 7e
8. Informed Consent Considerations
- Routinely discussing the possibility of intraoperative recall and mitigation steps is advisable as part of informed consent for general anesthesia
- This is particularly important for trauma, cardiac, and obstetric surgery where the risk is higher
- Patients undergoing regional or monitored anesthesia care with sedation should be counseled that awareness is expected (and desired) in those settings
Key References:
- Morgan and Mikhail's Clinical Anesthesiology, 7e, pp. 2347–2348
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e (Depth of Anesthetic Monitoring section)
- Miller's Anesthesia, 10e (Electroencephalography and BIS Monitoring section)
- Sabiston Textbook of Surgery, 11e, p. (CNS Monitoring section)
- Mulholland and Greenfield's Surgery, 7e (Awareness and Level of Consciousness Monitors)
BIS
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, deep content from Miller's Anesthesia on BIS. Here is the complete synthesis:
Bispectral Index (BIS) — In Depth
1. Background and Rationale
Standard clinical signs of anesthetic depth (hemodynamics, movement) are unreliable:
- Tachycardia/hypertension can arise from many non-awareness causes
- Movement is abolished by neuromuscular blockade
- There is no direct correlation between sympathetic response and cortical awareness
The BIS was developed to give clinicians an objective, real-time measure of cortical activity and consciousness depth. It is the most clinically studied processed EEG monitor available.
— Miller's Anesthesia, 10e
2. How BIS Works
Signal Acquisition
- A single-channel (single frontal region) adhesive sensor is placed on the patient's forehead
- The raw EEG from cortical surface activity is captured and processed
The EEG Signal During Anesthesia
During the awake state: small-amplitude, high-frequency (gamma/beta) activity (~5–10 μV)
As anesthesia deepens with GABA-ergic agents (propofol, volatile ethers):
| Stage | EEG Finding |
|---|---|
| Mild sedation | Beta buzz (12–30 Hz oscillations) |
| Loss of responsiveness | Anteriorization — frontal alpha oscillations (8–12 Hz) replace posterior alpha |
| Surgical anesthesia | Alpha-delta pattern (slow, high-amplitude waves) |
| Deep anesthesia | Burst suppression |
| Maximal suppression | Isoelectricity |
BIS Algorithm — Four Components
BIS uses a proprietary weighted algorithm based on four EEG parameters:
- Relative α/β ratio — low frequency power vs. high frequency power
- Bicoherence (bispectral analysis) — phase coupling between EEG waves; decreases with anesthesia depth
- Suppressed EEG waves — amplitude suppression detected
- Burst suppression ratio (BSR) — fraction of time the EEG is isoelectric
These are combined into a dimensionless number from 0 to 100:
| BIS Value | Clinical State |
|---|---|
| 100 | Fully awake |
| 80–100 | Sedation/light hypnosis |
| 40–60 | General anesthesia (target range) |
| <40 | Deep hypnosis / burst suppression |
| 0 | Isoelectric (flat) EEG |
— Morgan and Mikhail's Clinical Anesthesiology, 7e, Table 6–1
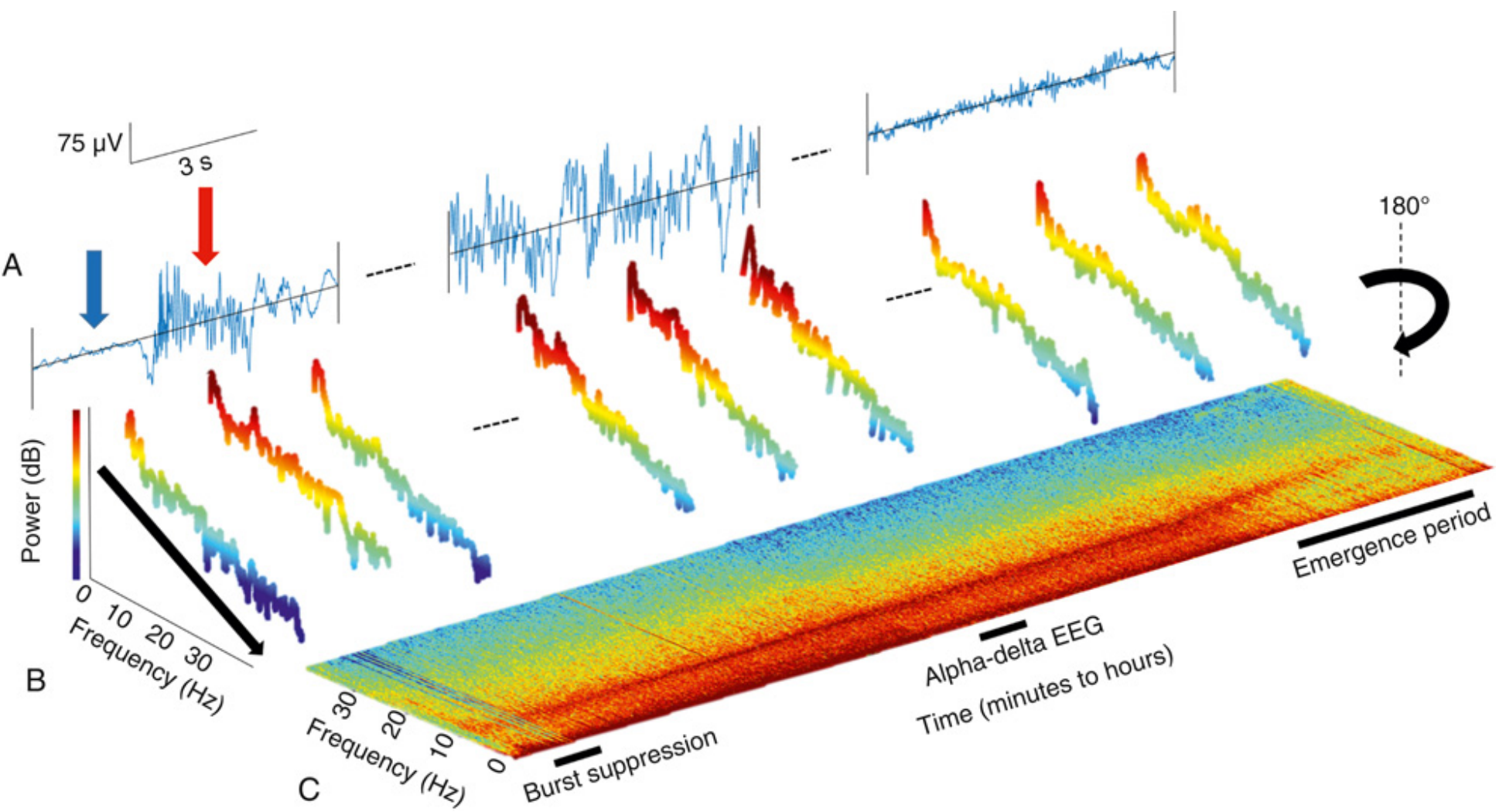
3. Burst Suppression Detection
Burst suppression is a state of deep cortical depression in which periods of near-isoelectric EEG alternate with bursts of electrical activity. In the BIS monitor, this is detected using the QUAZI suppression subalgorithm, which contributes to the final BIS index. On a spectrogram, burst suppression appears as alternating bands of power and silence.
Clinical significance: Burst suppression under anesthesia correlates with postoperative delirium, though whether actively avoiding it prevents delirium and POCD remains unclear.
— Miller's Anesthesia, 10e
4. EEG Artifacts Affecting BIS
The BIS signal is susceptible to several noise sources that can produce false readings:
| Artifact | EEG Appearance | Spectrogram Pattern |
|---|---|---|
| Eye blinks | Large amplitude frontal shifts | Thin vertical lines |
| Electrocautery | High amplitude bursts | Broad red blocks across all frequencies |
| ECG artifact | Sharp spikes at heart rate frequency | Horizontal stripes (especially during burst suppression) |
| EMG (muscle activity) | High-frequency, fuzzy waveforms | Vertical broadband red bands |
EMG artifact is particularly important: EMG during anesthesia is not noise — it signals the patient is likely grimacing and may need increased analgesia or hypnosis.
Electrode impedance must be kept below 5–8 kΩ for reliable signals.
5. Clinical Evidence
Major Randomized Trials
| Trial | n | Design | Outcome |
|---|---|---|---|
| B-Aware (Myles et al.) | ~2000 | BIS vs. standard care (high-risk) | BIS reduced AWR (landmark trial; criticized for low fragility index) |
| B-Unaware | ~2000 | BIS vs. end-tidal MAC ≥0.7 (high-risk) | No difference |
| BAG-RECALL | ~6000 | BIS vs. end-tidal MAC ≥0.7 (high-risk) | No difference |
| Mashour et al. (MACS) | ~18,836 | BIS vs. end-tidal agent | No significant difference; terminated for futility |
Meta-analysis (52 studies, 41,331 patients):
- BIS monitoring more than halved AWR vs. clinical monitoring alone (OR = 0.36, 95% CI 0.21–0.60)
- AWR rate: 3/1000 with BIS vs. 9/1000 with clinical monitoring
- No significant difference vs. end-tidal anesthetic agent monitoring
- Evidence graded as low certainty due to rarity of events
— Miller's Anesthesia, 10e
Schwartz's Summary
"A multicenter trial of over 6000 patients showed that titrating anesthetic concentration to the BIS monitor was not superior to titrating anesthetic depth to end-tidal anesthetic concentration with goal MAC > 0.7." — Schwartz's Principles of Surgery, 11e
Current Consensus
- BIS is beneficial for TIVA (no gas equivalent; IV line loss may go undetected)
- BIS is NOT superior to end-tidal MAC monitoring when volatile agents are used
- BIS can prevent anesthetic overdose (burst suppression avoidance)
- The ASA has not adopted BIS monitoring as a universal standard of care
6. Limitations of BIS
| Limitation | Explanation |
|---|---|
| Agent specificity | Ketamine and nitrous oxide produce atypical EEG patterns not well-represented in BIS algorithm |
| Pediatrics | Unreliable at certain developmental stages |
| Individual variability | A BIS of 50 in one patient ≠ BIS of 50 in another; awareness has been reported with BIS 40–90 |
| Proprietary algorithm | Black-box — exact weightings unknown |
| Trained on healthy volunteers | Performance may differ in elderly, critically ill, or neurologically abnormal patients |
| Hypothermia | Reduces EEG activity independently of anesthetic depth |
| EMG contamination | Can falsely elevate BIS, suggesting lighter anesthesia than present |
| Rare event problem | AWR incidence (~1:1000) makes monitoring performance statistically limited; 111 false alarms per true case detected with a "90% sensitive" monitor |
| Neural inertia | BIS values at emergence differ from those at equivalent induction concentrations |
7. Validated Screening Tool: The Modified Brice Interview
Postoperative screening for AWR uses the Modified Brice Questionnaire:
- What is the last thing you remembered before going to sleep?
- What is the first thing you remembered when you woke up?
- Can you remember anything between these two periods?
- Did you dream during your operation?
- What was the worst thing about your operation?
Classification into "aware" or "not aware" requires adjudication with intraoperative records, as some experiences reflect emergence rather than true intraoperative awareness.
8. Practical Summary
- Target BIS 40–60 for general anesthesia
- Target BIS ~30 in specific contexts (e.g., severe TBI with fentanyl infusion titration)
- Use alongside end-tidal MAC monitoring, not as a replacement
- Essential for TIVA — provides the only continuous depth signal when no volatile agents are used
- Check electrode impedance; recognize and account for EMG, ECG, and cautery artifacts
- Do not dismiss clinical signs (movement, hemodynamics) in favor of the BIS value alone
Sources: Miller's Anesthesia, 10e (Chapter 36 — Intraoperative Awareness and EEG Monitoring); Morgan and Mikhail's Clinical Anesthesiology, 7e (Table 6–1); Schwartz's Principles of Surgery, 11e; Sabiston Textbook of Surgery, 11e
This is a shared conversation. Sign in to Orris to start your own chat.