Migraine management
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
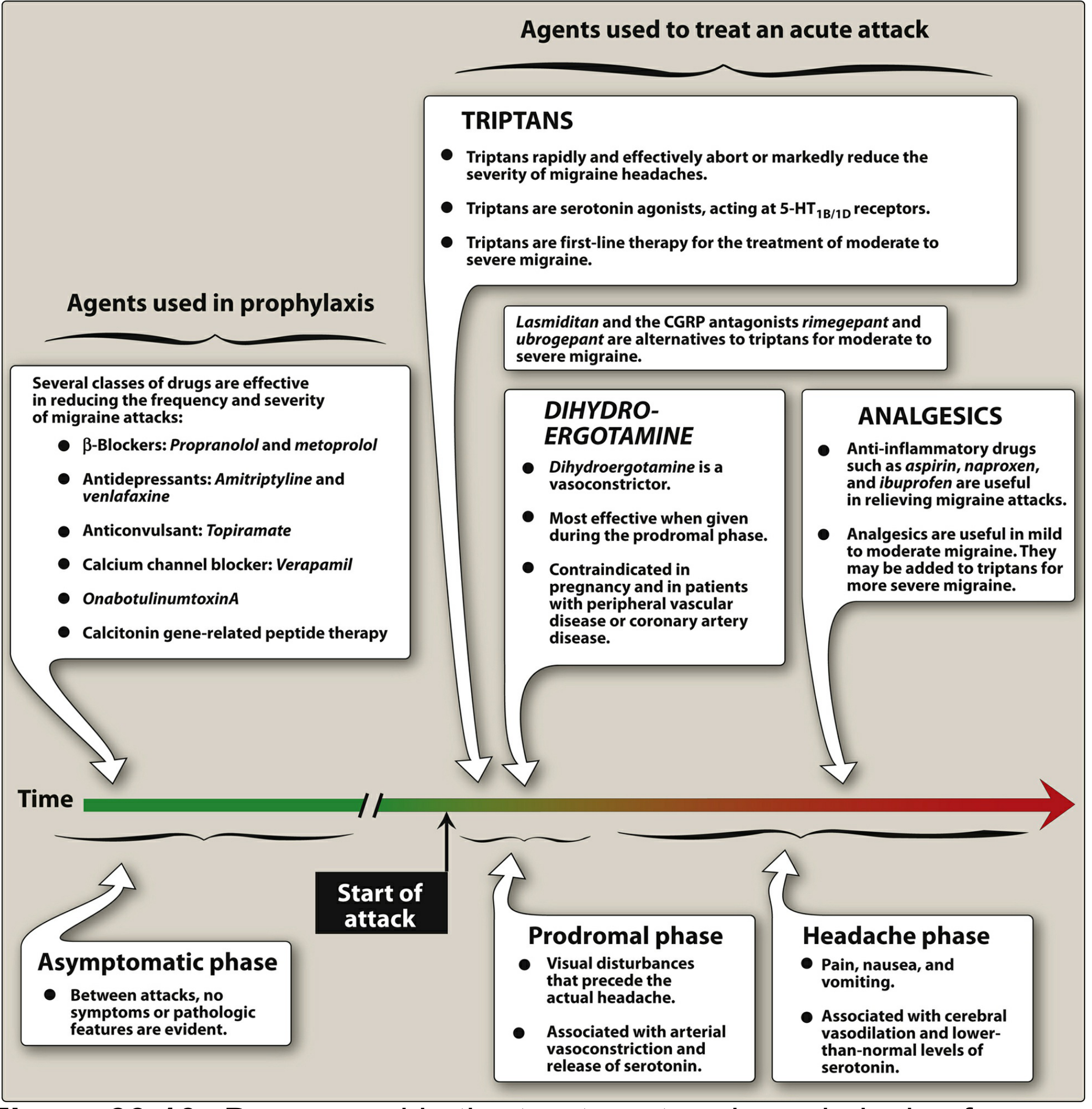
Here is a comprehensive overview of migraine management, drawn from multiple authoritative sources including Goldman-Cecil Medicine, Bradley & Daroff's Neurology, and Lippincott Pharmacology.
Migraine Management
Pathophysiology (Brief)
Migraine pain arises from activation of the trigeminocervical system, which innervates pain-sensitive intracranial structures (dura mater, meningeal and cerebral vessels). This triggers release of vasoactive neuropeptides — CGRP, substance P, PACAP, VIP — causing vasodilation, neurogenic inflammation, and central sensitization. The migraine brain is characteristically hyperexcitable, with exaggerated responses to sensory stimuli and impaired pain inhibition during attacks.
Acute (Abortive) Treatment
Stratified Care Principle
Treatment should be stratified by attack severity, not stepped. Matching drug potency to headache severity results in less disability and fewer medication days. Prompt treatment improves outcomes.
Important: Once an attack is fully developed, oral agents are less effective due to reduced GI motility. Non-oral routes (intranasal, subcutaneous, suppository) are preferred when nausea or vomiting is prominent.
Mild Attacks — Non-Specific Analgesics
| Drug | Dose |
|---|---|
| Acetaminophen | 650–1000 mg |
| Aspirin | 250–1000 mg |
| Ibuprofen | 400–600 mg |
| Naproxen | 500–825 mg |
| Diclofenac | 50 mg |
| Ketoprofen | 75 mg |
Antiemetics (prochlorperazine, metoclopramide) are useful adjuncts when nausea is present.
Moderate–Severe Attacks — Migraine-Specific Therapy
1. Triptans (First-line)
Mechanism: 5-HT1B/1D receptor agonists → cranial vasoconstriction + inhibition of trigeminal neuropeptide release. May also act centrally on the trigeminal nucleus caudalis.
Available agents: sumatriptan, zolmitriptan, rizatriptan, eletriptan, almotriptan, naratriptan, frovatriptan
- Abort or markedly reduce headache in ~70% of patients
- Sumatriptan routes: oral, subcutaneous (fastest onset, ~20 min), intranasal
- Zolmitriptan: oral or nasal spray
- Combination of sumatriptan + naproxen has superior efficacy
Contraindications: uncontrolled hypertension, ischemic heart disease, Prinzmetal angina, significant cardiovascular risk factors
2. Ergotamine / Dihydroergotamine (DHE)
- DHE 1–2 mg intranasally or subcutaneously; ergotamine tartrate 2 mg sublingually
- Most effective early in the attack (prodromal phase)
- Requires antiemetic pretreatment if given IV
- Contraindicated in pregnancy, peripheral vascular disease, coronary artery disease
3. Lasmiditan (Ditan)
- Selective 5-HT1F agonist — no vasoconstriction
- Safe in patients with cardiovascular contraindications to triptans
- Dose: 50–200 mg orally
- Side effect: sedation — driving contraindicated for ≥90 min (possibly up to 8 hours)
4. CGRP Receptor Antagonists (Gepants)
- Rimegepant 75 mg orally; ubrogepant 50–100 mg orally
- ~10% absolute increase in pain freedom at 2 hours vs. placebo
- Useful when triptans fail or are contraindicated
- Few side effects; no vasoconstriction
5. Combination / Rationale Polytherapy
Combining agents with different mechanisms is more effective than monotherapy:
NSAID + Triptan (or ergot) + Dopamine antagonist antiemetic (prochlorperazine or metoclopramide)
Very Severe Attacks
| Option | Dose/Route |
|---|---|
| DHE | 1 mg SC or 0.5–1 mg IV (with antiemetic) |
| Ketorolac | 60 mg IM or 30 mg IV |
| Prochlorperazine | 10–25 mg IM or 10 mg IV (over 5 min) |
| Metoclopramide | 10 mg IV |
| Celecoxib solution | 120 mg orally |
Opioids: last resort only. Meperidine is ineffective. Oral opiates should not be used for chronic recurrent primary headache — risk of medication overuse headache (MOH).
Neuromodulation (Newer Non-Pharmacologic Options)
FDA-cleared devices for acute migraine:
- Non-invasive vagus nerve stimulation (nVNS)
- Trigeminal nerve stimulation
- Occipital nerve stimulation
- Transcranial magnetic stimulation (TMS)
- Remote electrical neuromodulation (smartphone-controlled)
Caution: avoid in patients with cardiac pacemakers.
Special Population: Pregnancy
- Mild–moderate: acetaminophen ± isometheptene mucate + dichloralphenazone
- Antiemetics: prochlorperazine 10–25 mg, metoclopramide
- Triptans and ergotamines are generally avoided
Prophylactic (Preventive) Treatment
Indications: ≥2 attacks/month with significant disability or neurologic signs; inadequate response to acute therapy; medication overuse.
First-Line Agents (supported by all major guidelines)
| Class | Drug | Typical Daily Dose |
|---|---|---|
| β-Blockers | Propranolol | 80–240 mg |
| Metoprolol | variable | |
| Timolol, nadolol, atenolol | variable | |
| Anticonvulsants | Topiramate | titrated |
| Divalproex sodium | titrated |
Second-Line / Alternative Agents
| Class | Drug | Notes |
|---|---|---|
| Tricyclic antidepressants | Amitriptyline 10–150 mg at night | independent of antidepressant effect |
| Nortriptyline, imipramine | similar; try for ≥3 months | |
| SNRIs | Venlafaxine | |
| Calcium channel blockers | Verapamil 80–160 mg TID | better for migraine with aura |
| Botulinum toxin | OnabotulinumtoxinA | chronic migraine (≥15 days/month) |
CGRP-Based Preventive Therapy (newer)
| Type | Agents |
|---|---|
| Oral gepants (CGRP antagonists) | Rimegepant, atogepant |
| Injectable anti-CGRP monoclonal antibodies | Erenumab, galcanezumab, fremanezumab, eptinezumab |
These have demonstrated efficacy in episodic and chronic migraine with favorable side effect profiles.
Key Principles Summary
- Treat early — delayed treatment is less effective
- Match drug potency to attack severity (stratified care > step care)
- Avoid opiates as a routine strategy — risk of MOH
- Avoid analgesic overuse (especially >10–15 days/month) — can transform episodic to chronic daily headache
- Combination therapy targeting multiple mechanisms outperforms monotherapy for severe attacks
- Prophylaxis takes 2–3 months to evaluate fully; use shared decision-making
Sources: Goldman-Cecil Medicine (25th ed.), Bradley & Daroff's Neurology in Clinical Practice, Lippincott Illustrated Reviews: Pharmacology, Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.