acuts appendicitis complications, Treatment,cause, symptom,Pecularities in children. under 3 years
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I have very comprehensive content. The Schwartz content was fully within the 250-line block and the Rosen's EM content covered the full pediatric section including under-5 and under-3 peculiarities. I now have enough to give a comprehensive, well-cited answer. Let me compile the full response.
Acute Appendicitis — Comprehensive Overview
Etiology (Causes)
The fundamental mechanism is luminal obstruction of the appendix, leading to a cascade of edema → vascular congestion → ischemia → bacterial invasion → necrosis → perforation.
Common causes of obstruction:
- Fecaliths (hardened stool — most common in adults) — also the most important predictor of perforation
- Lymphoid hyperplasia — the predominant cause in children, triggered by enteric infections (viral/bacterial gastroenteritis, respiratory infections)
- Vegetable/fruit seeds, barium, parasites (e.g., Enterobius vermicularis, Ascaris)
- Tumours (carcinoid, mucocele) — rare, more relevant in adults
The appendix wall becomes distended; luminal pressure rises above venous pressure, causing mucosal ischemia. Gut bacteria (E. coli, Bacteroides, Pseudomonas, Streptococcus) then invade the wall.
— Schwartz's Principles of Surgery, 11th ed.
Symptoms
Classic Presentation (Adults & Older Children)
| Symptom | Details |
|---|---|
| Abdominal pain | Begins as vague, crampy, periumbilical pain (visceral phase) → migrates to right lower quadrant (RLQ), constant & sharp (somatic phase) — "Migratory pain" |
| Anorexia | Almost universal; precedes pain onset |
| Nausea & Vomiting | Follow pain onset |
| Low-grade fever | Usually 38–38.5°C; high fever suggests perforation |
| Constipation or diarrhoea | Variable |
Classic Physical Signs
- McBurney's point tenderness — 2/3 of way from umbilicus to ASIS
- Rovsing's sign — LLQ pressure causes RLQ pain (peritoneal irritation)
- Psoas sign — RLQ pain on right hip extension (retrocaecal appendix)
- Obturator sign — RLQ pain on internal rotation of right flexed hip (pelvic appendix)
- Rebound tenderness (Blumberg sign) — suggests peritoneal irritation
- Guarding and rigidity — muscular defense
— Rosen's Emergency Medicine, Schwartz's Surgery
Complications
| Complication | Details |
|---|---|
| Perforation | Most feared; rate increases with duration; >24–36 h markedly elevated risk |
| Peritonitis | Localised → generalised; chemical then bacterial |
| Appendiceal abscess/phlegmon | Walled-off perforation; palpable RLQ mass; fever persisting >5 days |
| Pelvic abscess | After perforation in pelvic appendix |
| Pylephlebitis | Septic thrombophlebitis of the portal venous system — rare but life-threatening |
| Sepsis & septic shock | From gram-negative bacteraemia post-perforation |
| Adhesions/intestinal obstruction | Post-inflammatory or post-operative |
| Wound infection | Common post-operatively in complicated appendicitis |
| Stump appendicitis | Inflammation of residual appendiceal stump after appendectomy |
| Enterocutaneous fistula | Rare, post-drain or post-op complication |
Morbidity and mortality increase significantly if the appendix ruptures prior to operative management.
— Rosen's Emergency Medicine, Schwartz's Surgery 11th ed.
Treatment
1. Non-Operative Management (Antibiotics Alone)
- Viable option for uncomplicated appendicitis (no fecalith, no perforation, no abscess)
- Broad-spectrum IV antibiotics (e.g., piperacillin-tazobactam, or ceftriaxone + metronidazole)
- Resolution in 80–90% of cases within 24–48 hours
- Drawback: recurrence rate up to 40% at medium-term follow-up → many surgeons use it as a bridge to elective interval appendectomy
- Patients with fecaliths are excluded from non-operative management
2. Operative Management (Standard of Care)
- Laparoscopic appendectomy — gold standard; preferred in adults and children alike
- Performed within 12–24 hours of diagnosis
- Open appendectomy reserved for laparoscopic conversion situations
- Preoperative: IV fluids, analgesia, IV antibiotics
- Same-day discharge possible in early uncomplicated disease
3. Complicated Appendicitis (Perforated/Abscess)
- Peritonitis + haemodynamic instability → emergency surgery
- Localised abscess/phlegmon present >5 days → non-operative approach first:
- IV antibiotics
- Interventional radiology (IR) drain if accessible abscess present
- Followed by interval appendectomy at 6–8 weeks
- Antibiotic duration guided by: fever, leukocytosis, source control status, ileus
— Schwartz's Principles of Surgery, Current Surgical Therapy 14th ed., Rosen's Emergency Medicine
Peculiarities in Children — General
Children differ from adults in several critical ways:
| Feature | Children vs. Adults |
|---|---|
| Omentum | Underdeveloped → cannot wall off infection → diffuse peritonitis more common |
| Appendiceal wall | Thinner → ruptures earlier in the disease course |
| Peak age | 9–12 years; uncommon <5 years |
| Perforation rate | Higher overall in children; inversely related to age |
| Classic symptoms | Often absent or atypical in young children — cannot reliably localise pain |
| Rovsing, Psoas, Obturator signs | Poor sensitivity/specificity in young children; unreliable |
| Differential | Mesenteric adenitis (often post-viral URTI) frequently mimics appendicitis in children |
| Imaging | Ultrasound and MRI preferred over CT in children (avoids ionising radiation) |
| Scoring | Pediatric Appendicitis Score (PAS) and Alvarado score used; labs alone insufficient |
⚠️ Peculiarities in Children UNDER 3 Years — Special Emphasis
This age group carries the highest risk and worst outcomes of any paediatric subgroup:
1. Rarity but High Lethality
- Appendicitis is uncommon under age 5 and rare under age 3, but when it occurs it is a diagnostic emergency
- The smaller, thinner-walled appendix and immature immune/omental response mean the progression from inflammation to perforation is extremely rapid
2. Perforation Rates >50%
"Perforation is highest among children younger than 5 years, among whom more than 50% are ruptured at the time of surgery." — Rosen's Emergency Medicine
In children under 3, this rate is even higher. The anatomical absence of a mature omentum means perforation leads directly to diffuse peritonitis rather than a localised abscess.
3. Atypical and Non-Specific Presentation
- Cannot describe or localise pain — they present with irritability, crying, restlessness
- Parents report refusal to eat, unusual posturing (lying still, flexing legs), lethargy
- Vomiting and diarrhoea are prominent → frequently misdiagnosed as gastroenteritis
- Fever may be the dominant or only finding early on
- The classic periumbilical → RLQ migration of pain is rarely elicitable or described
4. Diagnostic Difficulty
- Clinical signs (McBurney's, Rovsing's, Psoas, Obturator) are not assessable or reliable
- Examination is difficult due to lack of cooperation → tenderness often only detected as crying/guarding on palpation of RLQ
- WBC and CRP are helpful but non-specific
- Paediatric scoring systems (PAS, Alvarado) are not validated in this age group
- Ultrasound is first-line imaging — but visualisation is operator-dependent and may be limited
5. High Misdiagnosis Rate
- Most common misdiagnoses: gastroenteritis, viral illness, intussusception, Meckel's diverticulitis
- Significant delays in seeking care by parents (child "too young to have appendicitis") compound the problem
- By the time diagnosis is made, the disease is often already perforated with generalised peritonitis
6. Clinical Course After Perforation
- Diffuse bacterial peritonitis rather than localised abscess (due to absent omental walling)
- Systemic sepsis develops rapidly
- Toxic appearance: high fever, abdominal distension, lethargy, dehydration
- Ileus and abdominal rigidity ("board-like abdomen") in severe cases
7. Management
- Urgent surgical intervention once diagnosis suspected — do not delay for diagnostic certainty
- Pre-operative IV fluid resuscitation, broad-spectrum antibiotics (covering gram-negatives and anaerobes)
- Laparoscopic appendectomy — standard even in small children; conversion to open is rarely necessary
- Post-operative antibiotics continued based on degree of contamination and clinical response
- Non-operative management with antibiotics generally not favoured in this age group given perforation rate
Ultrasound Image — Acute Appendicitis in a Child
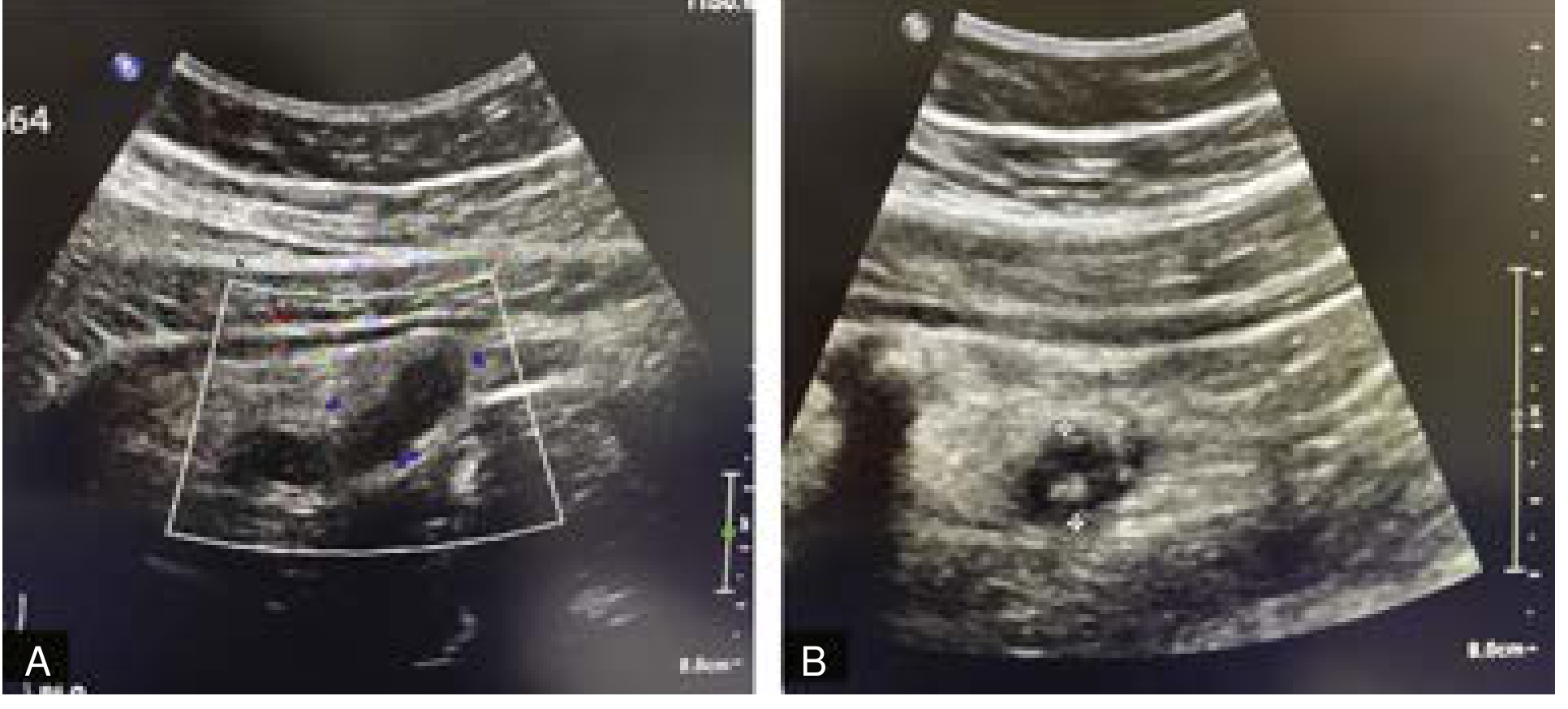
RLQ ultrasound in a 10-year-old with abdominal pain: (A) dilated fluid-filled tubular structure with increased vascularity; (B) echogenic focus = appendicolith. Both findings consistent with acute appendicitis.
— Current Surgical Therapy, 14th ed.
Summary Table — Under 3 Years vs. Older Children
| Feature | Older children (5–12 yr) | Under 3 years |
|---|---|---|
| Incidence | Common (peak 9–12 yr) | Rare |
| Pain localisation | Usually RLQ | Cannot describe; diffuse/none |
| Perforation rate at presentation | ~20–30% | >50–80% |
| Omental containment | Present | Absent |
| Peritonitis pattern | Localised abscess possible | Diffuse peritonitis |
| Clinical signs | Rovsing's, Psoas assessable | Unreliable / unassessable |
| Misdiagnosis rate | Moderate | Very high |
| Urgency | High | Extreme |
Key references:
- Schwartz's Principles of Surgery, 11th ed. — Chapter: The Appendix
- Rosen's Emergency Medicine: Concepts and Clinical Practice — Appendicitis (Paediatric)
- Current Surgical Therapy, 14th ed. — Paediatric Appendicitis
This is a shared conversation. Sign in to Orris to start your own chat.