Give me detailed information about dourine,it's etiology, transmission, pathogenesis, clinical signs, treatment and prevention from standard Veterinary reference books,and pathogenesis in flow chart form
dourine Trypanosoma equiperdum etiology transmission pathogenesis clinical signs treatment prevention veterinary
https://www.cfsph.iastate.edu/Factsheets/pdfs/dourine.pdf
Trypanosoma equiperdum dourine equids
https://www.cfsph.iastate.edu/Factsheets/pdfs/dourine.pdf
Trypanosoma equiperdum dourine pathogenesis treatment
A detailed vertical flowchart diagram showing the pathogenesis of Dourine (Trypanosoma equiperdum infection in horses). The flowchart should include the following steps with arrows connecting them: 1. Venereal Transmission - T. equiperdum in genital secretions transferred during coitus. 2. Local Tissue Invasion - Parasites penetrate mucous membranes of genitalia; Local inflammatory response (orchitis/vulvitis/vaginitis). 3. Genital Stage - Mucopurulent discharge; Edema of prepuce/glans penis or vulva; Genital vesicles and ulcers; Leukodermic (depigmented) scars. 4. Parasitemia - Trypanosomes enter bloodstream; Antigenic variation evades immune response; Intermittent parasitemia. 5. Systemic Dissemination - Hematogenous spread to skin, CNS, and lymphatics; Progressive hypoproteinemia and anemia. 6. Cutaneous Stage - Characteristic urticarial plaques (2-10 cm) on skin, especially neck/flanks; Plaques appear and disappear (pathognomonic). 7. Neurological Stage - CNS and peripheral nerve invasion; Facial paralysis (unilateral); Ptosis of lower lip; Hindlimb weakness, stiffness, incoordination; Progressive paralysis. 8. Terminal Stage - Severe emaciation; Cachexia; Recumbency; Death (50-70% mortality untreated). Clean professional medical/veterinary diagram style with blue color scheme.
DOURINE
Synonyms
1. ETIOLOGY
| Feature | Detail |
|---|---|
| Taxonomic position | Subgenus Trypanozoon, Salivarian section |
| Related organisms | Very closely related to T. brucei (nagana) and T. evansi (surra) |
| Morphology | Morphologically identical to T. evansi and T. brucei - cannot be distinguished by light microscopy |
| Unique characteristic | Primarily a tissue parasite - rarely invades blood (unlike other trypanosomes) |
| Size | 14-28 μm long; slender, spindle-shaped with a free flagellum and undulating membrane |
| Pathogenicity | Strains differ in virulence - some cause acute, fatal disease; others cause mild chronic illness |
| Genomic classification | Some researchers consider T. equiperdum a subspecies of T. brucei rather than a separate species (subject of ongoing debate) |
2. TRANSMISSION
Primary Route
- Venereal (coital) transmission - the organism's near-exclusive mode of spread
- Present in genital secretions (seminal fluid, vaginal secretions, urethral discharge) of infected animals
- Stallion to mare is more common, but mare to stallion transmission also occurs
- Can be present in semen before clinical signs appear (important epidemiologically)
- The parasite is shed in the mucous membranes and genital secretions at coitus and directly inoculated into the partner's mucous membranes
Other Routes (Rare)
- Conjunctival mucous membranes - occasional non-venereal infection
- Vertical transmission (mare to foal) - documented but uncommon; may occur transplacentally or during parturition
- Iatrogenic - contaminated equipment at artificial insemination could theoretically spread infection
Carrier State
- Donkeys and mules are commonly asymptomatic carriers and serve as a silent reservoir
- Periodically, the organism disappears from the genital tract for weeks to months - animals are non-infectious during these periods
- Parasitemia is intermittent and often undetectable in chronic stages
Incubation Period
- Ranges from a few weeks to several years (typically 1-4 weeks in experimental infections)
Geographic Distribution
- Endemic in Africa (Mediterranean coast, southern Africa, Ethiopia, Namibia)
- Middle East, Asia (Mongolia, Russia, Central Asia)
- South America (Argentina, Bolivia)
- Eastern and Southern Europe (outbreaks reported in Italy in 2011)
- OIE/WOAH-listed disease - notifiable internationally
3. PATHOGENESIS
Pathogenesis Flowchart
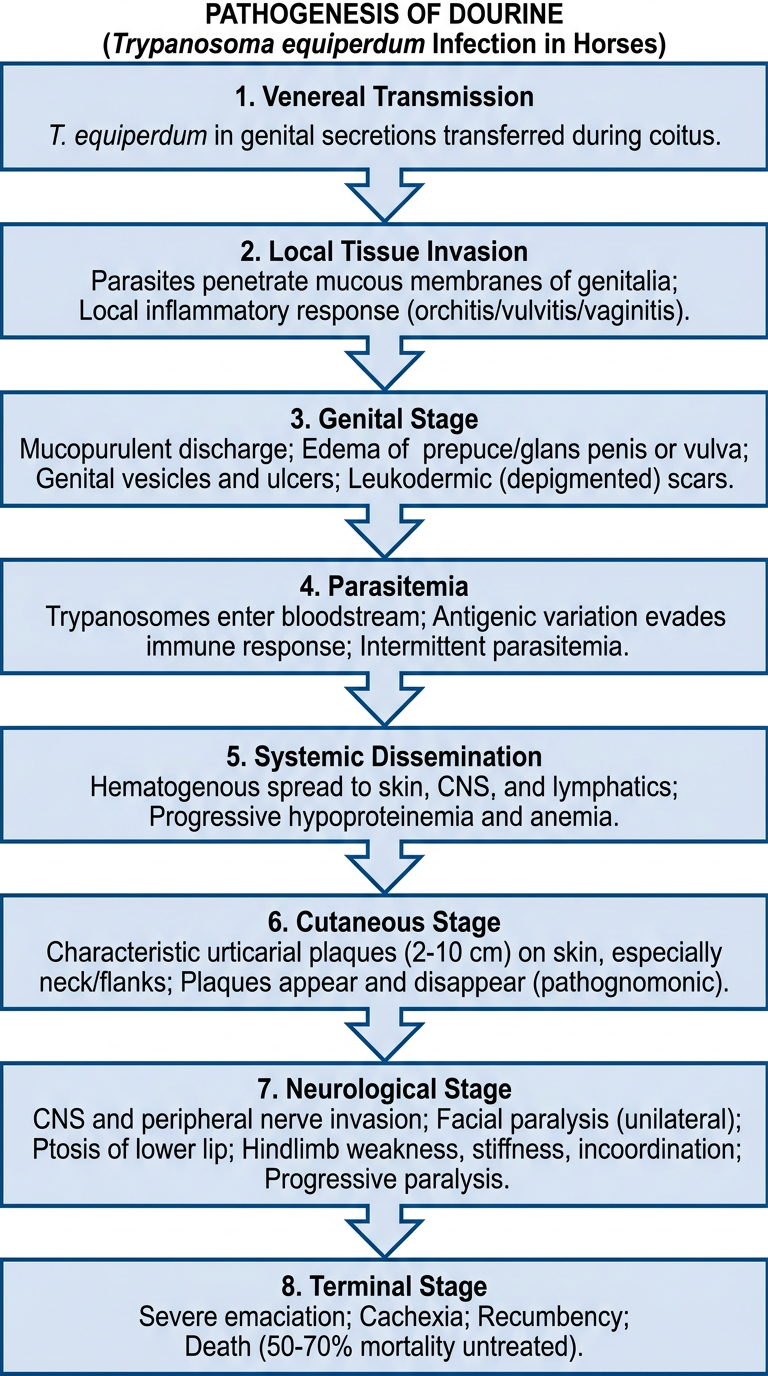
Step-by-Step Pathogenesis
- T. equiperdum enters via genital mucous membranes during coitus
- Parasites establish in the subepithelial connective tissue of the genitalia
- Triggers a local inflammatory response: vasodilation, increased vascular permeability, perivascular infiltration of mononuclear cells
- Results in edema and tissue thickening of genital structures
- Local inflammatory mediators cause mucopurulent discharge, orchitis (stallions), vulvitis/vaginitis (mares)
- Ulcers and vesicles develop on genital mucosa; heal leaving leukodermic (depigmented) patches - white scars
- Edema can wax and wane; genitalia become progressively indurated
- Parasites breach local defenses and enter the bloodstream
- T. equiperdum undergoes antigenic variation of its variable surface glycoproteins (VSG), allowing it to periodically evade host antibody responses
- This leads to waves of parasitemia alternating with antibody-mediated clearance
- The host mounts antibody, complement, and cellular immune responses, but cannot clear the organism completely
- Hematogenous spread to skin, lymph nodes, peripheral nerves, and CNS
- Hypoalbuminemia develops from chronic inflammation and protein loss
- Anemia results from immune-mediated erythrocyte destruction and bone marrow suppression
- Protein-poor edema extends beyond genitalia (ventral edema, limb edema)
- Characteristic urticarial (trypanosomal) plaques appear on skin, particularly on neck, flanks, and thighs
- Plaques are 2-10 cm diameter, raised, depigmented, appear and disappear transiently
- These "dollar plaques" are considered pathognomonic for dourine
- Result from localized perivascular infiltration and immune complex deposition in the dermis
- CNS invasion causes meningoencephalitis and myelitis
- Peripheral neuritis contributes to motor deficits
- Demyelination in the lumbar/sacral spinal cord causes hindlimb ataxia and paresis
- Facial nerve palsy (unilateral), ptosis of lower lip
- Progressive weakness - hindlimbs > forelimbs
- Severe cachexia and progressive emaciation
- Profound hypoproteinemia with effusions (pleural, peritoneal, synovial)
- Recumbency, complete paralysis, death
- Untreated mortality: 50-70% (MSD Veterinary Manual)
4. CLINICAL SIGNS
Stage I - Genital Stage
- Mucopurulent urethral discharge
- Edema and swelling of prepuce, glans penis, scrotum
- Orchitis and epididymitis
- Genital vesicles and ulcers → heal as white leukodermic scars
- Decreased libido or reluctance to breed
- Mucopurulent vaginal discharge
- Edema of vulva and mammary gland
- Vulvitis, vaginitis
- Thickened semi-transparent patches on vaginal mucosa
- Polyuria, signs of discomfort
- Abortion (with virulent strains)
Stage II - Cutaneous Stage
- Urticarial/trypanosomal plaques (2-10 cm diameter) - raised, circular, edematous
- Found on neck, flanks, back, thighs
- Appear and disappear within hours to days - pathognomonic
- Skin may show depigmented patches
Stage III - Neurological Stage
- Facial nerve palsy - usually unilateral
- Ptosis of the lower lip (very characteristic)
- Progressive hindlimb weakness, stiffness, and lameness
- Gait abnormalities: ataxia, stumbling, dragging of hind feet
- Inability to mount (detected only at mating in mild cases)
- Muscle atrophy and wasting
- Progressive paralysis leading to recumbency
Systemic Signs (Throughout)
- Progressive emaciation and weight loss
- Intermittent fever (corresponds with waves of parasitemia)
- Anemia (pale mucous membranes)
- Generalized lymphadenopathy
- Ventral edema
- General weakness and lethargy
Clinical Course Summary
| Presentation | Duration | Outcome |
|---|---|---|
| Peracute | Days to 1 week | Death |
| Acute | 1-2 months | Death or progression to chronic |
| Chronic | Months to years | Wasting, death or rare recovery |
| Subclinical | Indefinite | Carrier state (common in donkeys) |
5. POST-MORTEM / PATHOLOGICAL LESIONS
- Edema and inflammation of genitalia; white leukodermic scars
- Perivascular mononuclear infiltration in skin, genitalia, nerves
- Demyelination in lumbar/sacral spinal cord
- Minimal internal organ lesions (inconsistent): pinpoint white hepatic foci, splenic congestion
- Increased synovial fluid in joints
- Yellowish fluid in thoracic and abdominal cavities (hypoproteinemia)
- Severe muscle atrophy and subcutaneous fat depletion
6. DIAGNOSIS
| Test | Details |
|---|---|
| Serology (primary) | Complement fixation test (CFT) - OIE prescribed; ELISA; IFAT |
| Direct parasitology | Wet smear of genital secretions; buffy coat smear - low sensitivity (parasitemia is transient) |
| Histopathology | Perivascular infiltration in skin/genitalia; demyelination in spinal cord |
| PCR | Identifies Trypanozoon subgenus but cannot distinguish T. equiperdum from T. evansi |
| Clinical signs | Trypanosomal plaques are pathognomonic; combination with serology is most reliable |
7. TREATMENT
Important note: It is uncertain whether any treatment can completely eliminate T. equiperdum. Long-term efficacy is unproven. Treatment may suppress clinical signs and parasitemia without achieving sterile cure, and relapse is well documented.
Drugs Used
| Drug | Dose / Route | Notes |
|---|---|---|
| Diminazene aceturate (Berenil) | 3.5-7 mg/kg IM | Most commonly used in endemic regions; may suppress but not cure |
| Quinapyramine sulfate | 3-5 mg/kg SC | Used as single agent or in combination |
| Combination therapy | Diminazene + quinapyramine | May be more effective than monotherapy (Sugimoto et al., 2020 - J Equine Vet Sci) |
| Suramin | 10 mg/kg IV | Used historically; nephrotoxic |
| Cymelarsan (melarsomine) | Experimental | Arsenical compound; limited availability |
Current Evidence (2025-2026)
- A 2025 study (PMID 39827514) identified 3'-deoxytubercidin as a potent candidate for treating surra and dourine
- A 2026 systematic review (PMID 41429593) - Raftery et al., Equine Vet J - reviewed equine trypanosomiasis disease management
Regulatory Consideration
- In many disease-free countries (e.g. USA, Western Europe), treatment is not permitted - infected animals are culled to protect disease-free status
- Treatment is only practiced in endemic regions as a control measure
8. PREVENTION AND CONTROL
Individual Animal Level
- Quarantine and testing of all new equids before introduction into a herd
- Serological screening (CFT or ELISA) of breeding animals before use
- Good hygiene at assisted matings and artificial insemination to prevent fomite-mediated spread
- Avoid breeding animals with clinical signs
Herd and Regional Level
- Prohibition on breeding in affected areas during outbreaks
- Quarantine zones around infected premises
- Serological surveillance to identify infected animals
- Culling of positive animals - standard approach in disease-free countries
- Identification and management of asymptomatic carriers (especially donkeys)
National/International Level
- Movement controls - restrict movement of equids from endemic to disease-free areas
- Import regulations - require negative CFT on imported equids
- OIE/WOAH notification - dourine is a listed disease requiring immediate reporting
- In the USA: notify state or federal veterinary authorities immediately upon suspicion
Vaccine
- No vaccine is available. Antigenic variation by T. equiperdum makes vaccine development extremely difficult.
Environmental Decontamination
- T. equiperdum is fragile in the environment and does not survive long outside a host
- Standard disinfectants effective against the closely related T. brucei include: 0.05% sodium hypochlorite, 70% ethanol, 2% formaldehyde, 2% TriGene, 0.05% glutaraldehyde
- Heat (50°C) kills 100% of T. brucei trypomastigotes
Summary Table
| Parameter | Details |
|---|---|
| Causative agent | Trypanosoma equiperdum (subgenus Trypanozoon) |
| Host species | Horses, donkeys, mules (equids); donkeys often asymptomatic carriers |
| Transmission | Primarily venereal (coitus); rarely vertical or conjunctival |
| Vector | None - unique among trypanosomes |
| Incubation | Weeks to years (typically 1-4 weeks) |
| Key clinical signs | Genital edema/discharge → trypanosomal skin plaques → neurological signs → emaciation |
| Pathognomonic sign | Transient urticarial plaques ("dollar plaques") on skin |
| Untreated mortality | 50-70% |
| Treatment | Diminazene aceturate ± quinapyramine sulfate (uncertain long-term efficacy) |
| Vaccine | None available |
| Reporting status | OIE/WOAH-listed notifiable disease |
- CFSPH Iowa State Dourine Factsheet (Updated September 2024)
- MSD Veterinary Manual - Trypanosomiasis in Animals (Updated March 2026)
- Gizaw Y, Megersa M, Fayera T. Dourine: a neglected disease of equids. Trop Anim Health Prod. 2017;49(5):887-97. (Springer)
- Raftery AG, Gummery L, Garcia K. Equine trypanosomiasis, a systematic review: Disease management. Equine Vet J. 2026 Mar. PMID 41429593
- Gilbert RO. Dourine. In: Foreign Animal Diseases, 7th ed. USAHA; 2008. p. 231-6.