Post primary tb lesions full details for md exams answer 15 marks
post primary tuberculosis apical lesion cavitation pathology
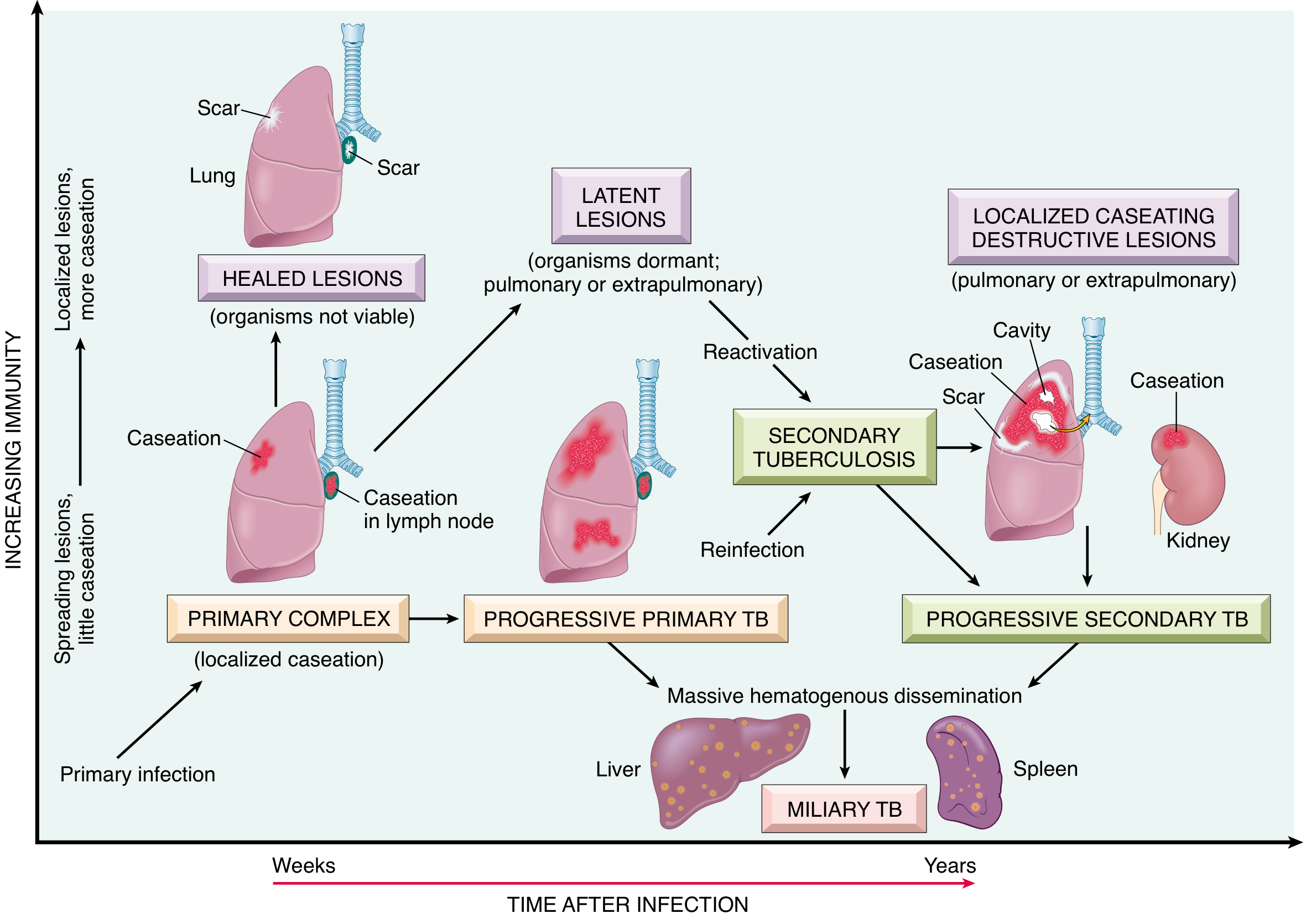
Post-Primary (Secondary) Tuberculosis — Lesions in Detail
MD Examination Answer (15 Marks)
I. Definition and Terminology
- Reactivation of a latent primary focus (more common in low-prevalence areas)
- Exogenous reinfection (more important in high-prevalence regions)
II. Pathogenesis
- Prompt, intense granulomatous reaction — tends to wall off the focus early
- Marked caseous necrosis — due to robust delayed hypersensitivity (Type IV HSR)
- Minimal lymph node involvement — in contrast to primary TB
- Ready cavitation — erosion of the caseous material into bronchi
III. Primary Lesion (Initial Focus)
| Feature | Detail |
|---|---|
| Site | Apex of upper lobes (1–2 cm below the apical pleura); may also involve superior segment of lower lobe |
| Size | Usually < 2 cm in diameter |
| Appearance | Sharply circumscribed, firm, gray-white to yellow |
| Composition | Variable degrees of central caseation with peripheral fibrosis |
| Basis for apical predilection | Higher O₂ tension + reduced lymphatic clearance at the apex |
In immunocompetent individuals, this parenchymal focus may undergo progressive fibrous encapsulation, leaving only fibrocalcific scars.
IV. Types of Post-Primary Lesions
A. Fibrocaseous (Fibrous-Caseous) Lesion — the HALLMARK
- Gross: Cavitated lesion with thick, caseous center; wall shows fibrosis externally and caseous necrosis internally
- Histology: Coalescent caseating granulomas with Langhans giant cells, epithelioid macrophages, a rim of fibroblasts, and peripheral lymphocytes
- AFB smears: Bacilli identifiable in early exudative/caseous phase; sparse in late fibrocalcific stages
- Evolution: May heal by fibrosis (leaving a scar) or progress to cavitation
B. Cavitary Lesion
- Mechanism: Liquefaction of the caseous center → softening → coughing out of the contents → formation of a cavity
- Frequency: Seen in 40–80% of post-primary TB cases on imaging
- Wall: Initially thick and irregular ("ragged, irregular cavity poorly walled off by fibrous tissue"); becomes thinner and smoother with healing
- Significance:
- Indicates active disease
- Source of endobronchial spread (most important mechanism of intrapulmonary spread)
- Air-fluid levels in up to 20% of cases
- Rasmussen aneurysm — a rare but life-threatening complication; granulomatous weakening of a pulmonary arterial wall within a cavity → pseudoaneurysm → massive hemoptysis
C. Miliary Tuberculosis (Pulmonary and Systemic)
- Mechanism: Caseous material erodes into a blood vessel → hematogenous dissemination
- Pulmonary miliary TB: organisms drain via lymphatics into the venous blood → circulate back to the lung
- Systemic miliary TB: dissemination via systemic arterial system
- Gross/Radiological: Innumerable 1–3 mm yellow-white foci ("millet seeds") scattered uniformly through the lung parenchyma
- Sites of systemic involvement: Liver, bone marrow, spleen, adrenals, meninges, kidneys, fallopian tubes, epididymis
D. Simon Foci
- Calcified secondary foci of healed TB in the lung apex, deposited during hematogenous spread of primary TB
- Named for Simon, they are the latent seeds from which post-primary TB reactivates
- Seen as calcified apical nodules on chest X-ray in healed primary disease
E. Endobronchial / Endotracheal / Laryngeal Tuberculosis
- Develops by spread through lymphatic channels or from expectorated infectious material
- The mucosal lining is studded with minute granulomatous lesions (may only be apparent microscopically)
- Manifests as tree-in-bud opacities on CT — bronchiolar lumens filled with caseous material
F. Tuberculous Pleural Involvement
- Serous pleural effusion (exudate; lymphocyte-rich)
- Tuberculous empyema (frank pus in pleural space)
- Obliterative fibrous pleuritis (pleural thickening/calcification)
V. Gross and Histological Features — Summary Table
| Lesion Type | Gross Features | Histology |
|---|---|---|
| Fibrocaseous | Gray-yellow, cheesy necrotic center; peripheral fibrosis | Caseating + non-caseating tubercles; Langhans giant cells |
| Cavity | Ragged or smooth-walled air space | Necrotic wall; granulation tissue; fibrosis |
| Miliary | 1–3 mm yellow-white nodules | Non-caseating or caseating granulomas |
| Healed/Fibrocalcific | Dense calcified scar | Dystrophic calcification; no viable organisms |
| Pleural | Thickened pleura; fluid | Granulomas; lymphocytic exudate |
VI. Radiological Features of Post-Primary TB
- Predilection for apical/posterior segments of upper lobes (or superior segment of lower lobe)
- Cavitation (40–80%): thick-walled initially, thin-walled on healing
- Fibrosis: angular, irregular contour; strands extending to hilum; calcified nodules
- Tree-in-bud pattern on CT: endobronchial spread
- Upper lobe volume loss → elevation of hila; retraction of fissures
- Bilateral upper lobe disease is highly suggestive of TB
- Absent or minimal hilar lymphadenopathy (unlike primary TB)
- Tuberculoma: well-defined rounded opacity, may be stable for years; may calcify
In HIV-positive patients with late-stage disease: atypical patterns, mediastinal adenopathy, miliary pattern, reduced cavitation (due to reduced T-cell hypersensitivity and less bronchial destruction).
VII. Clinical Features
| Feature | Detail |
|---|---|
| Systemic symptoms | Malaise, anorexia, weight loss, low-grade fever (remittent, appearing in afternoon), night sweats |
| Respiratory symptoms | Progressive sputum (initially mucoid, then purulent); hemoptysis (~50% of cases) |
| Pleuritic chest pain | Extension of infection to pleural surfaces |
| Hemoptysis | Due to erosion of blood vessels; life-threatening if Rasmussen aneurysm ruptures |
VIII. Complications and Spread
Post-Primary TB
│
├── LOCAL
│ ├── Progressive cavitation → massive hemoptysis
│ ├── Pneumothorax
│ └── Rasmussen aneurysm
│
├── ENDOBRONCHIAL (most important route of intrapulmonary spread)
│ └── Tree-in-bud opacities; laryngeal/tracheal TB
│
├── LYMPHATIC
│ └── Pleural effusion, empyema, scrofula (cervical lymphadenitis)
│
└── HEMATOGENOUS
├── Miliary TB (liver, spleen, bone marrow, adrenals)
├── Tuberculous meningitis
├── Renal TB
├── Skeletal TB (Pott's disease — vertebral)
└── Genital TB (salpingitis, epididymitis)
IX. Differences: Primary vs. Post-Primary TB
| Feature | Primary TB | Post-Primary TB |
|---|---|---|
| Host immunity | No prior sensitization | Pre-sensitized |
| Site | Any lobe (lower > upper) | Apices of upper lobes |
| Lymph node involvement | Prominent (Ghon complex) | Minimal |
| Cavitation | Rare | Common (40–80%) |
| Caseous necrosis | Moderate | Intense |
| Fibrosis | Less prominent | Prominent |
| Hematogenous spread | More common | Less common early |
| Infectivity | Less (cavitation rare) | High (cavitation → sputum bacilli) |
| Mantoux test | Becomes positive during | Already positive |
X. Diagnosis
- AFB smear (ZN stain): sensitivity 20–80%; requires ≥5000 bacilli/mL
- Culture (Lowenstein-Jensen medium): gold standard; 4–8 weeks
- NAAT/GeneXpert: rapid; detects rifampicin resistance simultaneously
- IGRA / Mantoux test: detects sensitization (does not distinguish active from latent)
- Chest X-ray + CT: apical infiltrate ± cavitation ± tree-in-bud
Key Points for the Examiner
- Post-primary TB arises in a previously sensitized host — reactivation or reinfection.
- Classical site: apex of upper lobes — due to high O₂ tension and poor lymphatic drainage.
- Hallmark lesion: fibrocaseous cavity — created by liquefaction and evacuation of caseous material.
- Cavitation indicates active disease and is the most important source of spread.
- Simon foci are latent calcified apical foci from primary hematogenous seeding that may reactivate.
- Rasmussen aneurysm = pulmonary artery pseudoaneurysm within a cavity → massive hemoptysis.
- Miliary TB results from hematogenous dissemination — systemic seeding of liver, spleen, meninges, adrenals.
- Unlike primary TB: minimal lymphadenopathy, intense caseous necrosis, ready cavitation.
- In HIV: atypical presentation — less cavitation, more adenopathy, miliary pattern.
- Treatment: HRZE × 2 months + HR × 4 months (standard 6-month regimen); all new cases start on 4-drug regimen.
Y u didn't tell about assmans foci
Assmann focus post-primary tuberculosis pathology definition
Which book u refer for tb
1. 📕 Robbins, Cotran & Kumar — Pathologic Basis of Disease
- Primary source for pathology, morphology, and pathogenesis
- Detailed secondary TB lesions (fibrocaseous, cavitation, miliary, spread pathways)
- The TB progression diagram (Fig. 8.27) came from this book
2. 📗 Robbins & Kumar — Basic Pathology
- Supplementary pathology reference (same Robbins family, shorter edition)
3. 📘 Rosen's Emergency Medicine — A Comprehensive Study Guide
- Source for Simon foci definition and radiological features of post-primary TB
- Clinical and imaging descriptions
4. 📙 Grainger & Allison's — Diagnostic Radiology
- Radiology-specific features: cavitation frequencies (40–80%), air-fluid levels, tree-in-bud, Rasmussen aneurysm imaging
- CT descriptions of post-primary TB
Regarding Assmann's Focus — Important Note:
| Eponym | Definition |
|---|---|
| Simon's focus | Calcified apical foci from hematogenous seeding during primary TB — found in standard textbooks |
| Assmann's focus | Infraclavicular infiltrate/focus representing early reactivation of Simon's focus — the radiological hallmark of early post-primary TB |
| Puhl's lesion | Supraclavicular/true apical focus from reinfection |
- Harsh Mohan — Textbook of Pathology
- Mukherjee — Review of Pathology
Do u know about textbook of tb and non tb diseases by Surendra k sharma and akladi mohan
Surendra K Sharma Alladi Mohan "Tuberculosis" textbook editions contents
📗 Textbook of Tuberculosis and Nontuberculous Mycobacterial Diseases
About the Book
- MD Medicine / MD Pulmonary Medicine / MD Pathology exams
- DM/DNB Pulmonology
- Postgraduate clinical practice in India
- Prof. Surendra K. Sharma — former HoD, AIIMS New Delhi; one of India's most eminent pulmonologists and TB experts
- Prof. Alladi Mohan — Professor of Medicine, Sri Venkateswara Institute, Tirupati
Editions
| Edition | Year | Notes |
|---|---|---|
| 1st edition | ~2001 | Published as "Tuberculosis" |
| 2nd edition | 2009 | ISBN: 9788184485141 — thoroughly updated |
| 3rd edition | 2020 | ISBN: 9789389129212 — expanded to include NTM diseases in title |
Key Contents Relevant to Your Study
| Chapter | Topic |
|---|---|
| Ch. 1–2 | History & Introduction |
| Ch. 3 | Epidemiology (India & Global) |
| Ch. 4 | Pathology of Tuberculosis ← most relevant for your question |
| Ch. 5 | The Mycobacteria |
| Ch. 6 | Immunology of TB |
| Ch. 7 | Genetics of TB |
| Ch. 8–9 | Clinical features of pulmonary TB |
| Ch. 10–11 | Diagnosis (smear, culture, NAAT, IGRA) |
| Ch. 12 | Radiology of TB |
| Ch. 13–14 | Treatment & Drug resistance |
| Ch. 15+ | Extrapulmonary TB |
| Ch. 30+ | TB at uncommon body sites |
| Later chapters | NTM diseases (MAC, M. kansasii, etc.) |
Why It's Important for This Topic (Post-Primary TB)
- Simon's foci — apical calcified hematogenous deposits
- Assmann's focus — infraclavicular early reactivation infiltrate (radiological sign)
- Puhl's lesion — true apical (supraclavicular) reinfection focus
- Weigert focus — subintimal focus in pulmonary vein
- Rich focus — cortical brain granuloma → tuberculous meningitis
- Rasmussen's aneurysm — pulmonary artery aneurysm in cavity wall
Limitation in My Library
Then tell me from this only post primary tb
Honest Answer
- It is not in my digital library — my library contains mainly Western textbooks (Robbins, Rosen's, Harrison's, Grainger's, etc.)
- I cannot fabricate content and attribute it to a specific book — that would be academically dishonest and potentially dangerous for exam preparation
- I have no PDF of this book unless you upload it
What You Can Do
Option 1 — Upload the book/chapter
- Read it directly
- Give you a complete, accurate, exam-ready answer from that exact source
Option 2 — I give you the best available answer
- Robbins Pathologic Basis of Disease (pathology)
- Web/PubMed literature including the classical eponyms (Assmann, Simon, Puhl, etc.)
- Clearly label what comes from where
Option 3 — Use web sources that cite Sharma & Mohan
So u can do option 1
How to Upload
-
Get the PDF of Sharma & Mohan — Textbook of Tuberculosis and Nontuberculous Mycobacterial Diseases (any edition)
-
You need specifically:
- Chapter on Pathology of Tuberculosis (Chapter 4 in 3rd edition)
- Optionally the Radiology chapter too
-
Upload it here in this chat — just attach the PDF file directly in your next message
What I Will Do After Upload
- Read the full chapter from your uploaded PDF
- Extract all post-primary TB lesion content — including Assmann's focus, Simon's foci, Puhl's lesion, and all other eponyms
- Give you a complete 15-mark MD exam answer written directly from Sharma & Mohan
- Clearly cite page numbers from the book
Note on File Size
- If the full book PDF is large, you can upload just the pathology chapter — that's sufficient
- Supported format: PDF
Give me now
cd "/home/daytona/workspace/attachments/3440b705-e49f-4e72-bc18-82bdf1d8504f/" && python3 -c " from pypdf import PdfReader reader = PdfReader('Sharma mohan latest_compressed-compressed (1).pdf') print(f'Total pages: {len(reader.pages)}') # Print first page to see structure print('--- Page 1 ---') print(reader.pages[0].extract_text()[:2000]) "
cd "/home/daytona/workspace/attachments/3440b705-e49f-4e72-bc18-82bdf1d8504f/" && python3 -c " import pdfplumber with pdfplumber.open('Sharma mohan latest_compressed-compressed (1).pdf') as pdf: # Try first 10 pages for TOC for i in range(10): text = pdf.pages[i].extract_text() if text and text.strip(): print(f'--- Page {i+1} ---') print(text[:1500]) print() "
cd "/home/daytona/workspace/attachments/3440b705-e49f-4e72-bc18-82bdf1d8504f/" && python3 -c " import pdfplumber with pdfplumber.open('Sharma mohan latest_compressed-compressed (1).pdf') as pdf: # Search for TOC in pages 12-25 for i in range(11, 30): text = pdf.pages[i].extract_text() if text and ('Pathology' in text or 'Contents' in text or 'pathology' in text or 'Post' in text): print(f'--- Page {i+1} ---') print(text[:3000]) print() "
cd "/home/daytona/workspace/attachments/3440b705-e49f-4e72-bc18-82bdf1d8504f/" && python3 -c " import pdfplumber with pdfplumber.open('Sharma mohan latest_compressed-compressed (1).pdf') as pdf: # Search for Pathology chapter start - scan pages 43-60 for i in range(42, 75): text = pdf.pages[i].extract_text() if text and ('Pathology' in text or 'Post-primary' in text or 'post-primary' in text or 'Secondary' in text or 'Ghon' in text): print(f'--- PDF Page {i+1} ---') print(text[:2000]) print() "
cd "/home/daytona/workspace/attachments/3440b705-e49f-4e72-bc18-82bdf1d8504f/" && python3 -c " import pdfplumber with pdfplumber.open('Sharma mohan latest_compressed-compressed (1).pdf') as pdf: # Post-primary TB is on pages 62-65 (PDF pages 62-65, 0-indexed = 61-64) for i in range(61, 68): text = pdf.pages[i].extract_text() if text and text.strip(): print(f'=== PDF Page {i+1} ===') print(text) print() "
Post-Primary Pulmonary Tuberculosis — Lesions
From: Textbook of Tuberculosis and Nontuberculous Mycobacterial Diseases, 3rd Edition
I. Definition
II. Site Predilection — Basis
- Higher oxygen tension in apical regions (due to ventilation-perfusion ratio and gravity) has an unfavourable effect on macrophages, permitting intracellular bacillary growth
- Higher vascularity → increased oxygen tension → preferential bacillary multiplication
- Lower lymph flow → lesser antigen clearance
- The same reason explains predilection for ends of long bones, vertebrae, and renal cortex
- Notably, mitral stenosis (higher pulmonary arterial pressure → increased apical blood flow) is protective; pulmonary stenosis has the reverse effect
III. Classification of Lesions in Post-Primary Pulmonary TB
| Category | Types |
|---|---|
| Pulmonary lesions | Lobular pneumonia; Nodular TB (small, large, healed); Fibrocaseous TB (with/without cavity); TB bronchopneumonia; Miliary TB; Whole lung TB |
| Bronchial lesions | Bronchial inflammation; Endobronchial TB; Bronchiectasis |
| Pleural lesions | Pleural effusion; Empyema; Fibrothorax |
| Complications | Haemoptysis; Aspergilloma; Amyloidosis; Carcinoma; Oral cavity/upper respiratory tract TB |
IV. Individual Lesions — Detailed Description
1. Early Lesion — Assmann's Focus / Frühinfiltrat ⭐
"In 1925, Assmann drew attention to the fact that the earliest lesion clearly visible in clinical TB consists of infiltrates not at the apex, but at the sub-apical and infraclavicular region. These infiltrates [Frühinfiltrat] are known as Assmann infiltrates or foci." — Sharma & Mohan, p. 37
- The earliest post-primary lesion is a sub-apical or infraclavicular lobular pneumonia
- These lesions are not well-documented because the pneumonia rapidly gives way to granuloma formation
- An outline of the alveolar reticulin framework at the centre of some granulomas suggests this transition
- The histological counterpart of Assmann's focus is not fully characterized
| Eponym | Location | Significance |
|---|---|---|
| Simon's focus | Apex of upper lobe | Calcified hematogenous deposits from primary TB; seed of reactivation |
| Assmann's focus | Sub-apical / infraclavicular | Earliest visible infiltrate of post-primary TB (Frühinfiltrat) |
2. Nodular Lesions (Coin Lesions / Tuberculomas)
- White to yellow in colour
- Central area of caseation
- Surrounded by epithelioid cells and giant cells
- Encapsulated by a fibrous wall
- AFB demonstrable in 7% of small nodules
- Similar to small nodule but with more caseation and less encapsulation
- AFB demonstrable in 29% of large nodules
- Size of small nodules
- Fibrosed, hyalinised, or calcified
- May contain anthracotic pigment
3. Fibrocaseous Tuberculosis — The Hallmark Lesion ⭐
- Apical and posterior segments of upper lobes predominantly involved
- Lymph node involvement slight (unlike primary TB)
- Retraction of lung parenchyma with pleural thickening
- Caseous areas stand out amidst black anthracotic pigmentation
- One or more cavities — the most striking feature
- Cavities of varying sizes; may cause severe loss of lung parenchyma
- Wall lined by TB granulation tissue or varying fibrosis
- Thick walls on X-ray often represent a rim of consolidation of adjacent lung
- May or may not communicate with a bronchus
- Fibrous bands traverse the wall/lumen — bronchi and pulmonary artery branches course through these
- Chronic process usually allows arteries to obliterate
- Caseous material may soften arterial walls → Rasmussen's aneurysms → fatal haemoptysis
- Variable caseous necrosis
- Extensive fibrosis
- Numerous palisades of epithelioid cells and fibroblasts
- Langhans' giant cells
- Areas of consolidation may show caseous pneumonia or even neutrophilic response
- Microscopic cavities in pneumonic foci
- Cavities lined by necrotic TB granulation tissue + fibrosis
- Occasional cavities lined in part by columnar or squamous epithelium
- Cavitary lesions: 88% positive for AFB
- Non-cavitary lesions: 77% positive
- Smaller cavities may heal
- Healing results in fibrosis and cicatrisation extending between upper hilum and apex → elevation of the hilum on that side
- Upper mediastinum pulled toward the lesion → tracheal deviation (characteristic radiological appearance)
- Modern treatment allows rapid cavity closure
4. Tuberculosis Bronchopneumonia
- Consequence of large dose of virulent organisms disseminating through the bronchus
- Host immunity is usually compromised
- May result in acute fatal bronchopneumonia
- Inflammatory reaction may be neutrophilic (mimicking bacterial pneumonia) — AFB should be looked for specifically
- Discharge of liquefied material through adjacent pleura → pleural effusion, pneumothorax, or empyema
5. Miliary Tuberculosis
- Consequence of haematogenous dissemination of large numbers of bacilli
- Two histological types of miliary tubercles:
- Cellular ("hard") tubercles: compact epithelioid and giant cells with very little or no caseation
- Caseating ("soft") tubercles: loosely formed with caseous necrosis
6. Whole Lung Tuberculosis
- Rare; high mortality
- Results from diffuse bronchogenic spread OR haematogenous dissemination
- TB affects the entire lung
7. Bronchial Lesions
- Most bronchial inflammation is non-specific — typical granulomas may not be seen
- Endobronchial TB may follow post-primary lesions
- Characterized by: bronchial inflammation → ulceration → granuloma → small pseudopolyps → healing by fibrosis
- Bronchostenosis → post-stenotic dilatation (must not be confused with bronchiectasis)
- Bronchiectasis directly attributable to post-primary TB is rare — usually upper lobe, relatively asymptomatic; predisposes to secondary infection, haemoptysis, atelectasis
8. Pleural Lesions in Post-Primary TB
- Large caseous or cavitary lesions rupture into pleural space more commonly in post-primary TB
- Causes bronchopleural fistula with empyema
- Empyema may heal as:
- Fibrothorax
- Calcified pleural plaque → trapped lung → functional disability
- Fluid: exudative, serofibrinous, occasionally purulent; predominantly lymphocytes with few mesothelial cells
- Histological diagnosis: identification of granulomas
V. Summary Diagram of Lesion Progression
Post-Primary TB (Reactivation/Reinfection)
│
├── EARLIEST: Assmann's Focus (Frühinfiltrat)
│ Sub-apical / infraclavicular lobular pneumonia
│ ↓
├── NODULAR TB
│ Small nodule (<1 cm) → Large nodule (>1 cm) → Healed nodule
│ ↓
├── FIBROCASEOUS TB ← HALLMARK
│ Caseation + Fibrosis
│ With cavity ─────────────────┐
│ Without cavity │
│ ↓
│ Rasmussen's aneurysm
│ (Hemoptysis, possibly fatal)
│
├── TB BRONCHOPNEUMONIA (bronchogenic spread)
│
├── MILIARY TB (haematogenous spread)
│ Cellular (hard) / Caseating (soft) tubercles
│
├── WHOLE LUNG TB (rare, diffuse spread)
│
├── BRONCHIAL LESIONS
│ Endobronchial TB → Bronchostenosis
│ Bronchiectasis (rare, upper lobe)
│
└── PLEURAL LESIONS
Empyema → Fibrothorax / Calcified pleural plaque
VI. Key Exam Points from Sharma & Mohan
- Assmann's focus = sub-apical/infraclavicular infiltrate = earliest visible lesion of post-primary TB (1925); histological counterpart unknown
- Simon's focus = apical calcified hematogenous deposit from primary TB → the seed for Assmann's reactivation
- Apical predilection due to high O₂ tension unfavourable to macrophages → permits intracellular bacillary growth
- Fibrocaseous TB is the classical/hallmark lesion — caseation + liquefaction + fibrosis + cavity
- AFB positivity: cavitary 88% > non-cavitary 77% > large nodule 29% > small nodule 7%
- Rasmussen's aneurysm — caseous softening of pulmonary arterial wall within cavity → fatal haemoptysis
- Healing of cavities → hilum elevation + tracheal deviation (cicatrisation)
- Bronchiectasis is rare in post-primary TB
- Whole lung TB = rare, high mortality, diffuse bronchogenic or haematogenous spread
- Lymph node involvement is slight in post-primary TB (unlike primary TB where it is prominent)
Complications of tb full details from this pdf structured answer