Define analyst micro and microwave complications of diabetes mellitus
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have rich, comprehensive content from multiple authoritative sources. Here is the complete, well-organized answer:
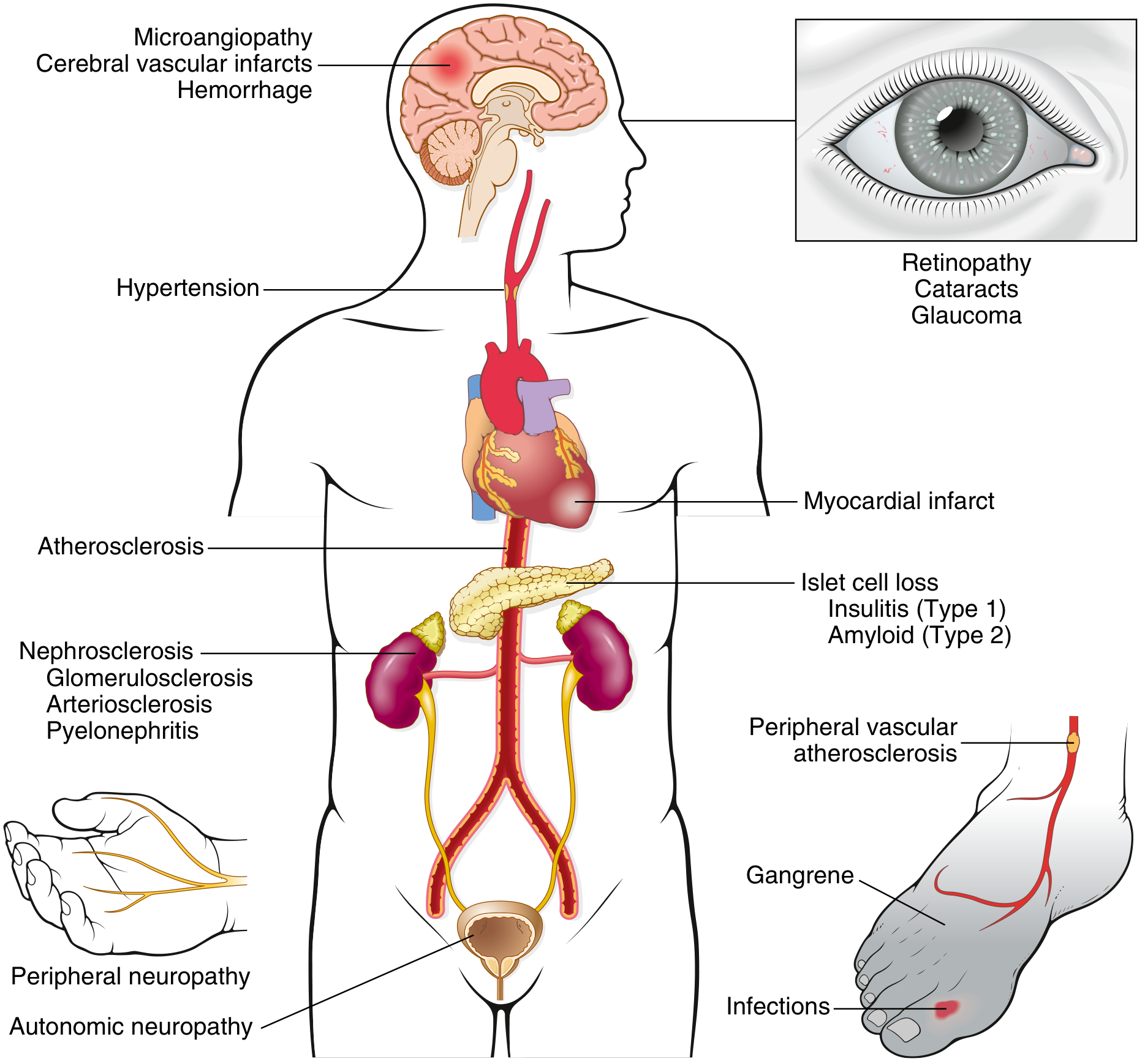
Micro and Macrovascular Complications of Diabetes Mellitus
(Note: The question title likely refers to "micro and macrovascular" complications - the terms "analyst" and "microwave" appear to be voice-to-text errors.)
Overview
The vascular complications of DM are subdivided into:
- Microvascular (diabetes-specific): retinopathy, nephropathy, neuropathy
- Macrovascular (shared with general population): ASCVD, peripheral arterial disease (PAD), cerebrovascular disease, heart failure
Nonvascular complications also occur: infections, skin changes, cheiroarthropathy, hearing loss, fractures, and cognitive impairment.
Pathogenesis of Complications
Chronic hyperglycemia is the central etiologic factor. Four major mechanisms operate:
1. Advanced Glycation End Products (AGEs)
Nonenzymatic reactions between intracellular glucose-derived precursors and amino groups of proteins form AGEs at an accelerated rate under hyperglycemia. AGEs bind to their receptor (RAGE) on macrophages, T cells, endothelium, and vascular smooth muscle, causing:
- Release of cytokines including TGF-β (promotes excess basement membrane deposition) and VEGF (implicated in retinopathy)
- Generation of reactive oxygen species (ROS) in endothelial cells
- Increased procoagulant activity
- Enhanced proliferation of vascular smooth muscle and extracellular matrix synthesis
- Cross-linking of extracellular proteins trapping LDL in vessel walls (accelerating atherosclerosis) and albumin in capillary walls (causing basement membrane thickening)
2. Protein Kinase C (PKC) Activation
Intracellular hyperglycemia stimulates de novo synthesis of diacylglycerol (DAG) from glycolytic intermediates, activating PKC. This leads to:
- Production of proangiogenic VEGF (neovascularization in retinopathy)
- Production of profibrogenic TGF-β (excess extracellular matrix deposition)
3. Polyol Pathway / Aldose Reductase
In insulin-independent tissues (nerves, lens, kidney, blood vessels), excess glucose is metabolized by aldose reductase to sorbitol and then fructose, consuming NADPH. Depletion of NADPH reduces regeneration of glutathione (an antioxidant) and increases oxidative stress. Sorbitol accumulation causes osmotic injury.
4. Hexosamine Pathway
Excess glucose flux through the hexosamine pathway leads to O-linked glycosylation of proteins and altered gene expression.
A possible unifying mechanism: hyperglycemia → increased mitochondrial production of ROS/superoxide → activation of all four pathways above, and potentially epigenetic changes that sustain gene expression changes long after glucose is controlled (the "metabolic memory" or legacy effect).
- Harrison's Principles of Internal Medicine 22E (2025), p. 3266-3267
- Robbins Basic Pathology, p. 749
MICROVASCULAR COMPLICATIONS
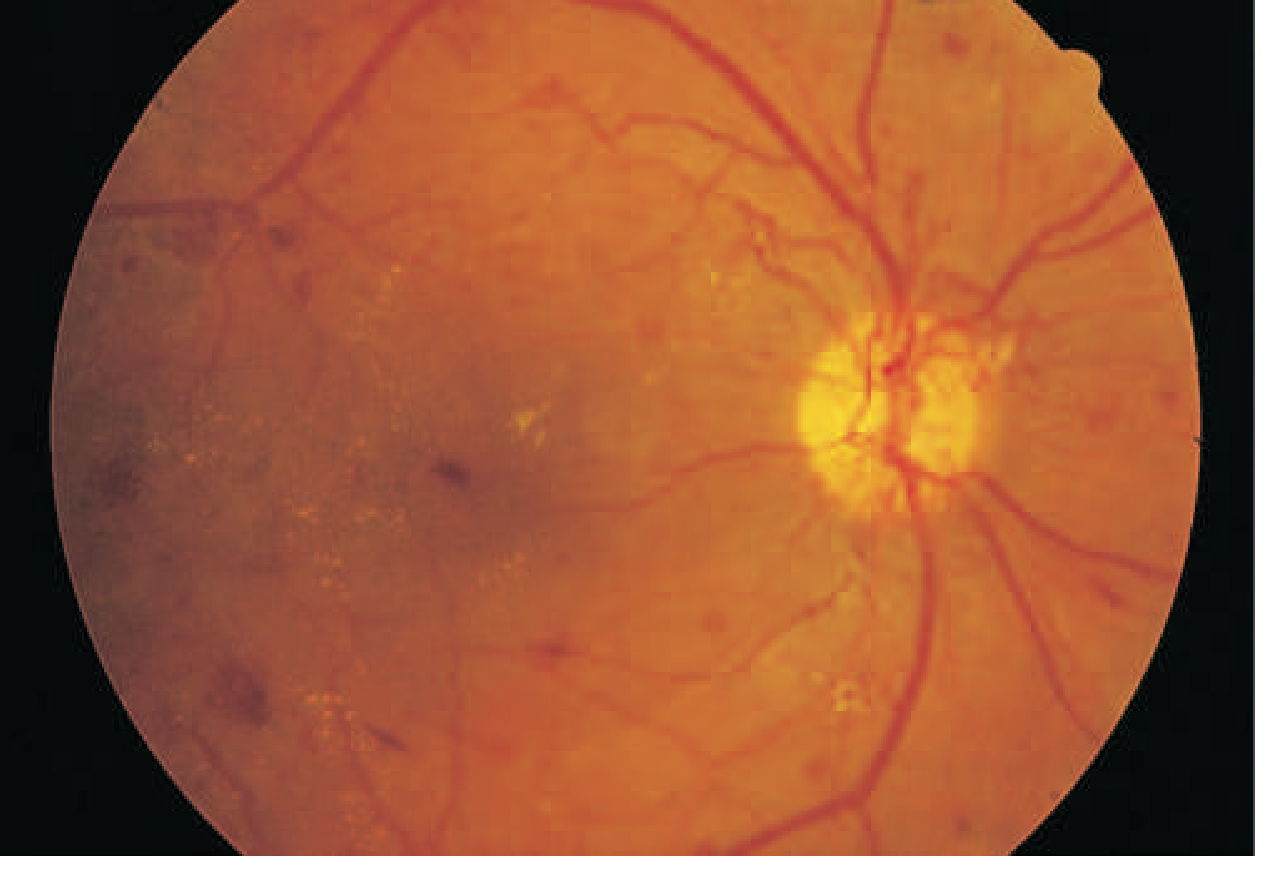
1. Diabetic Retinopathy
DM is the leading cause of new blindness in adults aged 20-74 in the United States. Glaucoma and cataracts also occur earlier and more frequently in diabetics.
Stages:
| Stage | Features |
|---|---|
| Nonproliferative (NPDR) | Retinal vascular microaneurysms, blot hemorrhages, cotton-wool spots, venous caliber changes, intraretinal microvascular abnormalities |
| Proliferative (PDR) | Neovascularization near optic nerve/macula; rupture leads to vitreous hemorrhage, fibrosis, and retinal detachment |
Pathophysiology of NPDR: Loss of retinal pericytes, increased retinal vascular permeability, altered retinal blood flow, and abnormal retinal microvasculature all lead to retinal ischemia.
Hallmark of PDR: Neovascularization in response to retinal hypoxia, driven by VEGF-A (which is the target of intravitreal anti-VEGF therapy).
Clinically significant macular edema can occur in either stage and is detected by fluorescein angiography and optical coherence tomography (OCT). It is associated with a markedly increased risk of moderate visual loss at 3 years.
Risk factors: Duration of DM and degree of glycemic control (best predictors); also hypertension, nephropathy, dyslipidemia.
- Harrison's, p. 3267-3268
2. Diabetic Nephropathy
Diabetic nephropathy is the leading cause of chronic kidney disease (CKD) and end-stage renal disease (ESRD) requiring renal replacement therapy. Approximately 20-40% of patients with diabetes develop it. It is more common in Black, Native American, and Hispanic individuals.
Natural History (initially defined in Type 1 DM):
- Early (first years): Glomerular hyperperfusion and renal hypertrophy → increased eGFR (hyperfiltration)
- First 5 years: Glomerular basement membrane (GBM) thickening, glomerular hypertrophy, mesangial expansion as GFR normalizes
- Later: Marked albuminuria with declining GFR (largely irreversible)
Pathological Lesions (Robbins):
- Diffuse basement membrane thickening - earliest change; detectable by EM before clinical renal dysfunction
- Diffuse mesangial sclerosis - mesangial matrix increase + mesangial cell proliferation; present in most with >10 years DM
- Nodular glomerulosclerosis (Kimmelstiel-Wilson lesion) - ball-like laminated matrix deposits in the glomerular periphery; present in 15-30% of long-term diabetics; virtually pathognomonic of diabetes
- Hyaline arteriolosclerosis - both afferent and efferent arterioles affected; amorphous thickening of arteriolar walls narrowing the lumen
- Pyelonephritis and necrotizing papillitis - more severe in diabetics
Pathogenic mechanisms include:
Soluble factors (angiotensin II, endothelin, growth factors, AGEs), hemodynamic alterations (glomerular hyperfiltration/hyperperfusion), structural changes (basement membrane thickening, mesangial expansion, fibrosis), and tubular dysfunction.
Screening:
-
Begin 5 years after Type 1 DM onset; at the time of Type 2 DM diagnosis; annually thereafter
-
Use urine albumin-to-creatinine ratio (UACR) on spot specimen + estimated GFR (eGFR)
-
Albuminuria defined as UACR >30 mg/g; moderate 30-299 mg/g; severe >300 mg/g
-
Harrison's, p. 3268-3270; Robbins Basic Pathology, p. 750-751
3. Diabetic Neuropathy
Diabetic neuropathy is the most common complication of diabetes and the most prevalent cause of neuropathy in the developed world.
Classification:
A. Diabetic Symmetric Peripheral Neuropathy (DSPN)
- Most common form
- Affects distal lower extremities more than upper
- Predominantly sensory loss (numbness, tingling, pain) with distal motor involvement
- Loss of protective sensation (LOPS) increases risk of plantar ulcers and Charcot arthropathy
- "Glove and stocking" distribution
- Chronic painful DSPN is difficult to treat; agents with some efficacy: gabapentinoids (pregabalin, gabapentin), SNRIs (duloxetine, venlafaxine), tricyclic antidepressants, capsaicin patch
B. Autonomic Neuropathy
- Cardiovascular: resting tachycardia, orthostatic hypotension (parasympathetic denervation)
- GI: gastroparesis (delayed gastric emptying - anorexia, nausea, vomiting, early satiety), altered bowel motility (constipation or diarrhea)
- Genitourinary: erectile dysfunction, neurogenic bladder, retrograde ejaculation
- Sudomotor: anhidrosis
C. Other forms: Mononeuropathy, cranial neuropathy (CN III most common), diabetic amyotrophy (lumbosacral plexopathy)
Pathophysiology: Microangiopathy and increased permeability of capillaries supplying the nerves (vasa nervorum), plus direct axonal damage from polyol pathway activity.
- Harrison's, p. 3270; Robbins Basic Pathology, p. 752
MACROVASCULAR COMPLICATIONS
Macrovascular disease reflects accelerated atherosclerosis of large and medium-sized arteries. The hallmark is identical to atherosclerosis in nondiabetics - just earlier onset and greater severity.
1. Coronary Artery Disease / Myocardial Infarction
- Most common cause of death in patients with diabetes
- MI is nearly as common in diabetic women as in men (unlike the general population where premenopausal women are relatively protected)
- ASCVD events and mortality are 2-4x greater in type 2 DM
2. Cerebrovascular Disease / Stroke
- Increased risk of ischemic stroke
- Diabetic microangiopathy can also cause cerebral vascular infarcts and hemorrhage
3. Peripheral Arterial Disease (PAD)
- Lower extremity ischemia from atherosclerosis of peripheral vessels
- Gangrene of the lower extremities is ~100 times more common in diabetics than the general population
- Interacts with peripheral neuropathy to cause the "diabetic foot"
4. Heart Failure
- Both HFpEF and HFrEF are increased; "diabetic cardiomyopathy" is a recognized entity (distinct from ischemic or hypertensive causes)
Key Difference from Microvascular Complications:
Microvascular complications are driven almost exclusively by chronic hyperglycemia. Macrovascular complications are also strongly driven by dyslipidemia, hypertension, insulin resistance, and inflammation (traditional cardiovascular risk factors), which is why tight glycemic control alone does not reduce macrovascular events as dramatically as it reduces microvascular events.
- Harrison's, p. 3267, 3269; Robbins Basic Pathology, p. 750
Evidence from Major Clinical Trials
| Trial | Population | Key Finding |
|---|---|---|
| DCCT | Type 1 DM | Intensive glycemic control (HbA1c 7.3% vs 9.1%) reduced microvascular complications by ~50-70% |
| UKPDS | Type 2 DM | Each 1% reduction in HbA1c = 35% reduction in microvascular complications; strict BP control reduced macro + microvascular events |
| DCCT/EDIC follow-up | Type 1 DM | "Metabolic memory" - benefit of prior intensive control persisted for ≥10 years even after glycemic control was equalized |
Summary Table
| Complication | Category | Key Feature |
|---|---|---|
| Retinopathy | Microvascular | Leading cause of blindness 20-74 yrs; NPDR → PDR with neovascularization |
| Nephropathy | Microvascular | Leading cause of ESRD; Kimmelstiel-Wilson nodule is pathognomonic |
| Peripheral neuropathy | Microvascular | Most common complication; distal symmetric sensory > motor |
| Autonomic neuropathy | Microvascular | Gastroparesis, orthostatic hypotension, erectile dysfunction |
| Coronary artery disease | Macrovascular | Most common cause of death in DM |
| Stroke | Macrovascular | Ischemic > hemorrhagic |
| PAD / Gangrene | Macrovascular | 100x more common than general population |
| Heart failure | Macrovascular | Both HFpEF and HFrEF |
Sources: Harrison's Principles of Internal Medicine 22E (2025) - p. 3265-3272; Robbins Basic Pathology - p. 749-752; Goldman-Cecil Medicine - Ch. 210
This is a shared conversation. Sign in to Orris to start your own chat.