Jaundice
Reading File
Finding Sources
Searching PubMed
"jaundice" AND "bilirubin"
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full response.
Jaundice
Jaundice (icterus) is the yellowish discoloration of the skin, sclera, and mucous membranes caused by accumulation of bilirubin. It becomes clinically visible when serum bilirubin rises above 2.5-3 mg/dL (normal <1 mg/dL). - Schwartz's Principles of Surgery, 11th Ed.
Bilirubin Metabolism - The Foundation
Bilirubin is produced primarily from breakdown of heme in red blood cells (and smaller amounts from myoglobin and cytochromes). Its metabolism has three phases:
| Phase | What Happens |
|---|---|
| Prehepatic | Heme converted to insoluble unconjugated (indirect) bilirubin; transported bound to albumin |
| Intrahepatic | Unconjugated bilirubin taken up by hepatocytes and conjugated with glucuronic acid (via UGT1A1) to form water-soluble conjugated (direct) bilirubin |
| Posthepatic | Conjugated bilirubin excreted via bile ducts into duodenum; gut bacteria convert it to urobilinogen |
Dysfunction at any phase causes jaundice. - Schwartz's Principles of Surgery
Classification by Phase (with Causes)
1. Prehepatic (Unconjugated Hyperbilirubinemia)
The conjugation system is overwhelmed by excess heme breakdown:
- Hemolytic anemias (inherited: spherocytosis, G6PD deficiency, sickle cell; acquired)
- Direct Coombs positive = immune-mediated (autoimmune, drug-induced)
- Direct Coombs negative = non-immune (mechanical, microangiopathy, infections)
- Ineffective erythropoiesis - thalassemia major, megaloblastic anemia (B12/folate deficiency), sideroblastic anemia, lead poisoning
- Large hematoma resorption, massive tissue infarction
- Albumin loss (burns, poor nutrition) - impairs unconjugated bilirubin transport to liver
Note: Hemolysis alone in a healthy liver cannot sustain bilirubin >4 mg/dL. Higher levels suggest concurrent hepatic dysfunction. - Harrison's Principles of Internal Medicine 22E
2. Intrahepatic (Hepatocellular or Cholestatic)
Unconjugated hyperbilirubinemia - conjugation defects:
| Condition | Mechanism | Notes |
|---|---|---|
| Gilbert Syndrome | UGT1A1 activity reduced to 10-35% of normal; also impaired uptake | Common (up to 8% prevalence); bilirubin usually <3 mg/dL; exacerbated by fasting, stress, illness, alcohol; benign |
| Crigler-Najjar Type I | Complete absence of UGT1A1 | Severe; kernicterus risk in neonates |
| Crigler-Najjar Type II | Markedly reduced UGT1A1 (>100 UGT1 mutations identified) | Less severe; residual enzyme activity |
| Physiologic neonatal jaundice | Immature UGT1A1 + enterohepatic recirculation | Self-limited; most neonates affected |
| Drug-induced | Rifampin, probenecid, novobiocin inhibit hepatic uptake | Resolves with drug cessation |
| Hypothyroidism | Impaired conjugation |
Conjugated hyperbilirubinemia - excretion defects:
| Condition | Mechanism |
|---|---|
| Dubin-Johnson syndrome | Impaired secretion of conjugated bilirubin from hepatocyte into canaliculi (MRP2 defect) |
| Rotor syndrome | OATP1B1/1B3 deficiency; interrupts conjugated bilirubin reuptake |
| Viral hepatitis | Hepatocellular injury disrupts secretion |
| Alcoholic hepatitis | Hepatocellular injury; can mimic obstruction |
| Drug-induced hepatitis | Many drugs - OTC agents, herbal supplements included |
| Primary biliary cholangitis (PBC) | Immune destruction of intrahepatic bile ducts |
| Primary sclerosing cholangitis (PSC) | Inflammatory stricturing of bile ducts |
| Ischemic hepatitis | Impaired hepatic blood flow |
| Sepsis | Endotoxin inhibits NTCP, MRP2, BSEP function |
| Cirrhosis | Combined liver insufficiency + portal hypertension |
| Intrahepatic cholestasis of pregnancy | Third trimester; BSEP/FIC1/MRP2/MDR3 gene polymorphisms; resolves postpartum |
| Acute fatty liver of pregnancy | Third trimester; microvesicular steatosis; can be fatal |
- Quick Compendium of Clinical Pathology, 5th Ed.; Sleisenger & Fordtran's GI & Liver Disease
3. Posthepatic (Obstructive/Extrahepatic - Conjugated)
Obstruction preventing bile flow into the duodenum:
Intrinsic obstruction:
- Choledocholithiasis (most common cause of extrahepatic obstruction)
- Benign biliary strictures (post-surgical: clips, ischemia, retained stones)
- Cholangiocarcinoma
- Cholangitis (bacterial infection - presents with Charcot's triad: fever, RUQ pain, jaundice)
- Papilla of Vater disorders
Extrinsic compression:
-
Pancreatic carcinoma (classic painless progressive jaundice in elderly)
-
Pancreatitis / pancreatic pseudocysts
-
Lymph node compression
-
Schwartz's Principles of Surgery 11th Ed.
Key Lab Differentiation
| Lab Finding | Suggests |
|---|---|
| ALP >3x ULN + transaminases <3x ULN | Cholestatic (obstructive) |
| Transaminases >3x ULN + ALP <3x ULN | Hepatocellular |
| Isolated unconjugated hyperbilirubinemia, all other LFTs normal | Gilbert's, hemolysis, Crigler-Najjar |
| Conjugated bilirubin >30% of total | Excretory defect (intrahepatic or posthepatic) |
| Leukocytosis + elevated amylase/lipase | Biliary obstruction / pancreatitis |
| Prothrombin time corrects with vitamin K | Cholestatic (fat-soluble vitamin malabsorption) |
| Prothrombin time does NOT correct | Hepatocellular synthetic failure |
| Thrombocytopenia | Cirrhosis (portal hypertension, reduced thrombopoietin) |
| Hemolytic anemia (positive Coombs, abnormal smear) | Prehepatic |
- Quick Compendium of Clinical Pathology 5th Ed.; Sleisenger & Fordtran's
Clinical Diagnostic Approach
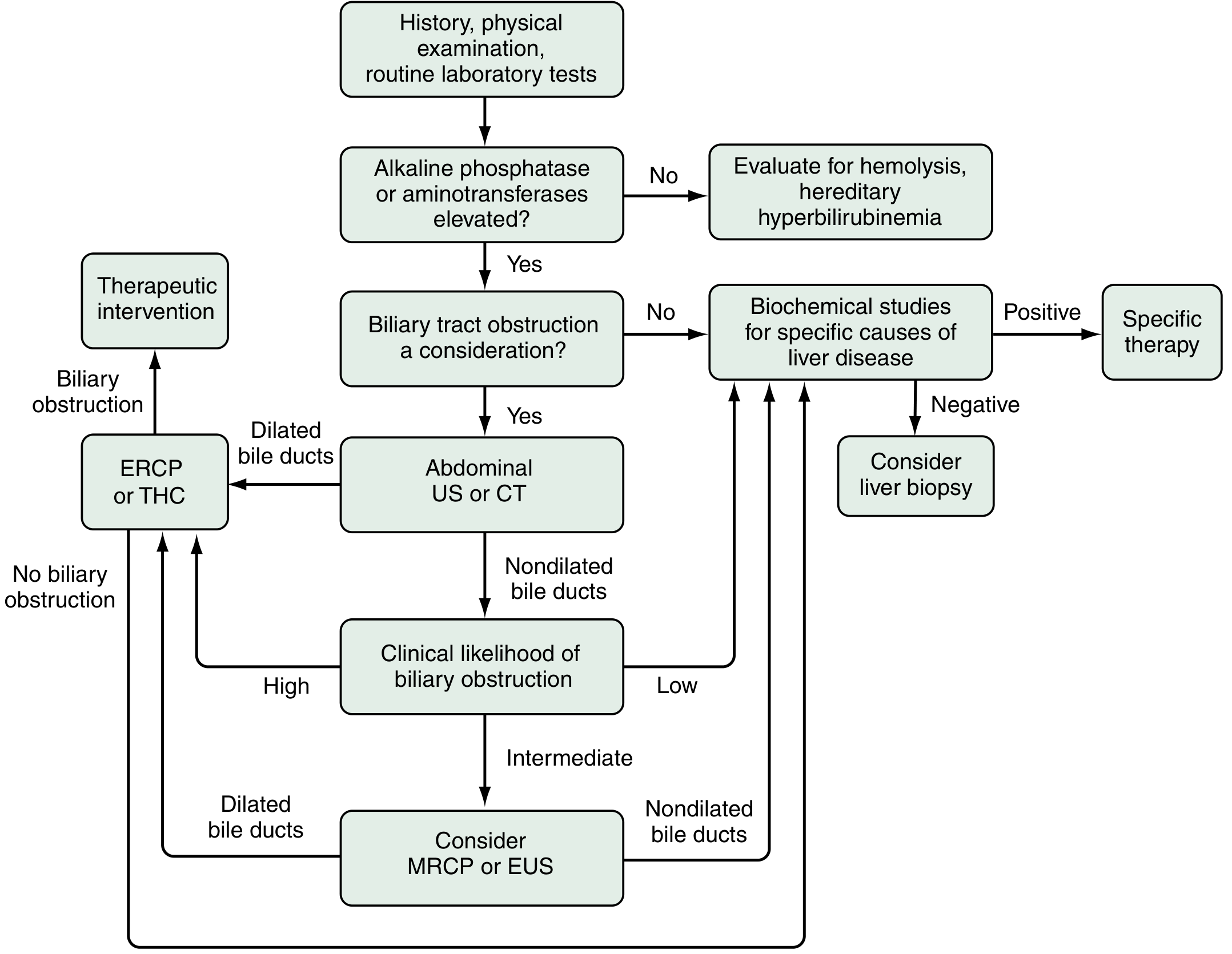
Four-step logical approach (Sleisenger & Fordtran's GI & Liver Disease):
- History, physical exam, and baseline labs
- Formulate working differential
- Select specialized tests to narrow possibilities
- Develop treatment/further testing strategy
History Clues
| Suggests Obstruction | Suggests Liver Disease |
|---|---|
| RUQ pain, fever, rigors | Viral prodrome (anorexia, myalgias, malaise) |
| Prior biliary surgery | Known hepatotoxin exposure |
| Older age | Blood products / injection drug use |
| Palpable abdominal mass | Family history of liver disease |
Physical Exam Clues
- Cholangitis: fever, RUQ tenderness
- Malignancy: painless jaundice, palpable gallbladder (Courvoisier's sign), weight loss
- Cirrhosis: ascites, splenomegaly, spider telangiectasias, gynecomastia, caput medusae, asterixis
- Wilson's disease: Kayser-Fleischer rings (pathognomonic)
History + physical + routine labs correctly classify jaundice as obstructive vs. non-obstructive in ~75% of cases. - Sleisenger & Fordtran's
Imaging Strategy
- Abdominal ultrasound - first line if obstruction is suspected (checks for dilated bile ducts, stones, masses)
- CT abdomen - better for extrahepatic masses, pancreatic pathology
- MRCP - non-invasive biliary tree imaging; preferred when intermediate clinical suspicion
- EUS - for distal biliary lesions, pancreatic assessment
- ERCP - diagnostic AND therapeutic (stent placement, stone removal); used when obstruction confirmed
Special Contexts
Jaundice in Pregnancy
- Hyperemesis gravidarum (1st trimester) - mild, self-limited
- Intrahepatic cholestasis of pregnancy (3rd trimester) - pruritus + jaundice; resolves postpartum; gene polymorphisms in BSEP, FIC1, MRP2, MDR3
- Acute fatty liver of pregnancy (3rd trimester) - microvesicular steatosis; can be fatal; requires urgent delivery
- HELLP syndrome - hemolysis, elevated liver enzymes, low platelets; preeclampsia variant
Jaundice in Cirrhosis
Results from liver insufficiency (inability to excrete bilirubin). In cholestatic diseases (PBC, PSC) driving cirrhosis, biliary damage contributes additionally. Jaundice appearing in compensated cirrhosis signals the transition to decompensated cirrhosis (median survival drops from >12 years to ~1.6 years). - Goldman-Cecil Medicine
Jaundice in the Critically Ill
Broad differential: hepatic ischemia, blood transfusions, hepatotoxic drugs, parenteral nutrition, occult sepsis, renal injury. Even when clinical status improves, jaundice may lag in resolving - important not to over-investigate. - Sleisenger & Fordtran's
Neonatal Jaundice
- Physiologic: UGT1A1 immaturity + enterohepatic recirculation of unconjugated bilirubin - peaks days 3-5, resolves by day 10-14
- Pathologic: hemolytic disease, infection, Crigler-Najjar, metabolic disease
- Phototherapy converts unconjugated bilirubin to water-soluble photoisomers for excretion without conjugation
Associated Symptoms
- Pruritus - from bile salt accumulation; more prominent in cholestatic jaundice. Treated with cholestyramine, antihistamines, rifampin, opioid antagonists, gabapentin
- Dark urine - conjugated bilirubin (water-soluble) spills into urine (bilirubinuria)
- Pale/clay-colored stools - absent urobilinogen due to bile duct obstruction
- Steatorrhea - fat malabsorption from absent bile in gut
Recent Evidence
Three recent reviews may be relevant:
- Evaluation of Jaundice in Adults - Nelson M et al., Am Fam Physician 2025 (PMID 39823630) - practical clinical approach update
- Managing neonatal hyperbilirubinemia: updated guideline - Chastain AP et al., JAAPA 2024 (PMID 39259272)
- Neonatal Hyperbilirubinemia - Wickremasinghe AC et al., Pediatr Clin North Am 2025 (PMID 40619190)
Sources: Schwartz's Principles of Surgery 11th Ed. | Sleisenger & Fordtran's GI & Liver Disease | Harrison's Principles of Internal Medicine 22E | Goldman-Cecil Medicine | Quick Compendium of Clinical Pathology 5th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.