Can you give me detial study about central line
Reading File
Finding Sources
Finding Sources
Searching PubMed
"central venous catheter" AND complications
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
I now have extensive, comprehensive information from multiple authoritative textbooks. Let me compile the full detailed study.
Central Line (Central Venous Catheter) - Detailed Study
1. Definition
A central line (central venous catheter, CVC) is a catheter inserted into a large central vein - typically the internal jugular (IJ), subclavian, or femoral vein - with the tip positioned in the superior vena cava (SVC) just above the right atrium, or in the inferior vena cava (IVC) for femoral lines. It provides direct access to the central circulation.
2. Anatomy
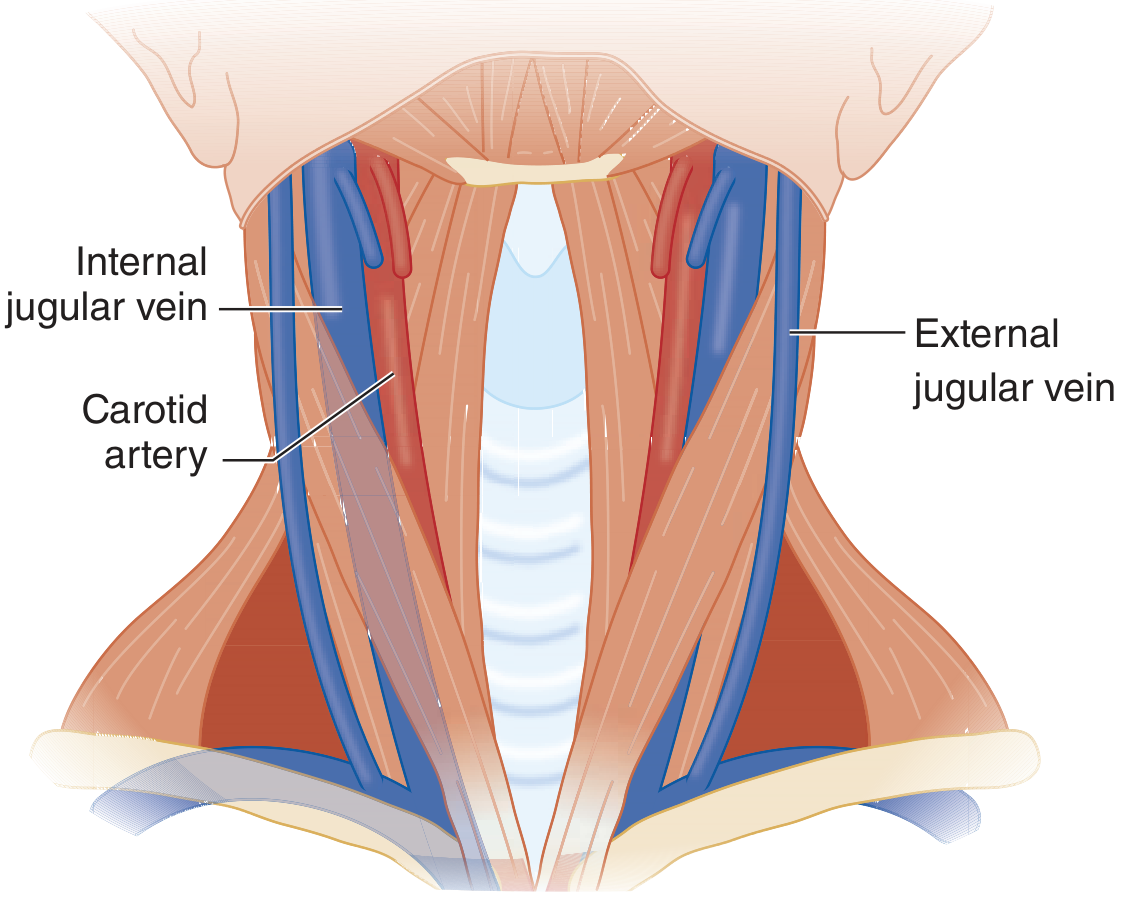
Vascular anatomy of the neck - Tintinalli's Emergency Medicine
Key Anatomical Points
Internal Jugular Vein (IJV)
- Lies lateral to the internal carotid artery inside the carotid sheath
- Overlies the carotid artery in more than 50% of patients (varies significantly)
- Joins the subclavian vein to form the brachiocephalic vein
- The right IJV offers a shorter, straighter course to the SVC and avoids the thoracic duct (which enters on the left side)
Subclavian Vein
- Crosses under the clavicle at the medial-to-proximal third of the clavicle
- The subclavian artery lies posterior and superior
- The thoracic duct joins the left subclavian vein at its junction with the left IJV
- Dome of the pleura lies posterior and inferior - risk of pneumothorax
Femoral Vein
- Travels in the femoral sheath deep to the medial third of the inguinal ligament
- Mnemonic for lateral-to-medial arrangement: NAVEL - Nerve, Artery, Vein, Empty space, Lymphatics
- Always cannulate below the inguinal ligament; injury above can cause retroperitoneal hemorrhage
3. Indications
From Tintinalli's Emergency Medicine (Table 31-4), indications include:
| Category | Specific Indication |
|---|---|
| Access | Inability to obtain peripheral venous access |
| Hemodynamic monitoring | CVP monitoring; pulmonary artery catheter placement |
| Drug administration | Vasoactive drugs (vasopressors, inotropes); vesicant chemotherapy |
| Nutrition | Total parenteral nutrition (TPN) - must be via a dedicated CVC |
| Fluid/blood | Rapid volume resuscitation; massive transfusion |
| Special procedures | Transvenous pacing; hemodialysis; plasmapheresis; Swan-Ganz catheter |
| Sampling | Mixed venous oxygen saturation monitoring |
4. Types of Central Lines
4a. Non-Tunnelled CVCs
- Standard triple-lumen or double-lumen catheters
- Inserted percutaneously at the bedside
- Short-term use (days to weeks)
- Single-, double-, or triple-lumen configurations available
4b. Tunnelled CVCs
- Hickman line: Most common; cuffed Silastic catheter, the Dacron cuff is placed halfway along the subcutaneous tunnel as a bacterial barrier; used for chemotherapy, prolonged TPN, bone marrow transplantation
- Groshong catheter: Has a pressure-sensitive valve at the tip (reduces backflow of blood into the catheter)
- Haemodialysis catheter: Large-bore, dual-lumen tunnelled line for dialysis access
Broviac (1973) first introduced the cuffed Silastic catheter for parenteral hyperalimentation; the Hickman catheter evolved from this and became the standard for bone marrow transplantation and prolonged IV feeding. Double- and triple-lumen versions superseded it when simultaneous chemotherapy and TPN were needed. - Pye's Surgical Handicraft, 22nd Edition
4c. Implantable Ports (Port-a-Cath)
- Totally subcutaneous reservoir connected to a central catheter
- Accessed via needle through the skin
- Lowest infection rate among long-term devices
- Preferred for intermittent long-term chemotherapy
4d. Peripherally Inserted Central Catheter (PICC)
- Inserted via basilic, brachial, or cephalic vein in the arm
- Tip advanced to SVC
- Lower immediate procedural risks (no pneumothorax)
- Higher DVT rates in long-term use
5. Technique - Seldinger (Guidewire) Method
The standard percutaneous technique is the Seldinger technique, as outlined in Tintinalli's Emergency Medicine (Table 31-8):
| Step | Action |
|---|---|
| 1 | Gown in sterile fashion; sterile gloves, gown, cap, mask |
| 2 | Prepare the site with chlorhexidine or povidone-iodine; allow to dry (30 s dry site; 2 min for femoral/moist site) |
| 3 | Drape patient from head to toe with large sterile drape |
| 4 | Identify anatomy/ultrasound; infiltrate with 1% lidocaine |
| 5 | Insert 18-gauge introducer needle at appropriate angle toward the vein |
| 6 | Confirm venous blood return in syringe (non-pulsatile, dark blood) |
| 7 | Advance guidewire through the needle (never let go of the wire!) |
| 8 | Remove the needle over the wire |
| 9 | Nick the skin with a #11 scalpel |
| 10 | Advance the venodilator over the wire |
| 11 | Remove the dilator; advance the catheter over the wire |
| 12 | Remove the guidewire; aspirate blood from each lumen and flush with normal saline |
| 13 | Secure the catheter with suture and apply sterile transparent dressing + Biopatch (chlorhexidine disc) |
| 14 | Confirm tip position with chest radiograph |
Pre-procedure Checklist (Table 31-7 - Tintinalli's)
- Time-out: correct patient, correct side/location
- Hand hygiene immediately prior
- Site sterilized and allowed to dry
- Head-to-toe sterile drape
- ALL staff in room wearing masks
- Door kept closed; traffic minimized
6. Site-Specific Techniques
Internal Jugular Vein
Three approaches: anterior, central (triangle), and posterior.
Preferred site: Right IJV - shorter, straighter course to the SVC; avoids the thoracic duct.
- Anterior approach: Identify carotid pulse medial to site; enter at midpoint of medial aspect of the sternal head of sternocleidomastoid (SCM) at 30-45 degrees, aim toward the ipsilateral nipple. Venous return typically at 3-5 cm depth.
- Central approach: Enter at the apex of the triangle formed by the two heads of the SCM.
- US guidance is strongly recommended: IJV overlies the carotid artery in >50% of patients.
Subclavian Vein
Infraclavicular approach:
- Patient head-down, neutral position, small towel under the thoracic spine
- Landmark: junction of middle and medial thirds of the clavicle
- Direct needle toward the suprasternal notch at a 10-degree angle, parallel to chest surface
- "Walk" the needle down the clavicle if bone is hit
- Venous return at 3-5 cm
Supraclavicular approach:
- Better US visualization of the proximal subclavian vein
- Longitudinal needle-US approach preferred to avoid pneumothorax
Important: Subclavian cannulation carries the risk of pneumothorax. If one-side attempt fails, get a CXR or US to rule out pneumothorax BEFORE attempting the other side.
Femoral Vein
- Patient supine, reverse Trendelenburg, hip slightly abducted, leg externally rotated
- Femoral vein is just medial to the femoral artery, 1-2 cm below the inguinal ligament
- 45-degree angle of approach
- In pulseless arrest - "V" technique: thumb on pubic tubercle, index finger on anterior superior iliac spine; femoral vein at the interdigital space just below the inguinal ligament
- Always insert below the inguinal ligament
7. Ultrasound Guidance
Ultrasound guidance is a recommended standard practice endorsed by most professional society guidelines. Key points from Murray & Nadel's Textbook of Respiratory Medicine:
- Improves first-attempt success rates and reduces complications, especially for less-experienced operators
- Recommended in both adult and pediatric patients
- Perform a preliminary scan before the procedure to assess vessel patency; for IJV/subclavian, document presence of sliding lung (to serve as a baseline if pneumothorax is later suspected)
- Short-axis (transverse/out-of-plane) view: Allows visualization of the vein and adjacent artery simultaneously; requires transducer fanning to track the needle tip
- Long-axis (longitudinal/in-plane) view: Needle must remain precisely in plane; allows full-length needle visualization; preferred for subclavian
- Neither approach is conclusively superior
- Always visualize the guidewire in short and long axis to confirm venous placement before dilation
- After the procedure, chest radiograph confirms catheter position; ultrasound can also be used with vascular and cardiac views
8. Tip Position
- Ideal position: SVC, just above the right atrium (at the SVC-RA junction)
- Must NOT be in the right atrium or right ventricle - risk of arrhythmia and perforation
- Confirmed by chest radiograph or fluoroscopy
- For tunnelled lines: image intensifier/fluoroscopy in the theatre is the standard
9. Complications
Immediate (Procedural)
| Complication | Notes |
|---|---|
| Arterial puncture | Most common; 1-5% incidence. Subclavian is not compressible - avoid in coagulopathy |
| Pneumothorax | Most common with subclavian approach (1-3%); subclavian artery and vein lie close to the pleura |
| Air embolism | Can occur when line is open to air; keep hubs capped |
| Hematoma | From arterial puncture or venous tear |
| Cardiac arrhythmia | Guidewire or catheter tip in the right atrium/ventricle |
Early
| Complication | Notes |
|---|---|
| Malpositioning | Catheter tip in wrong location (IJ, contralateral vein, SVC angulation) |
| Hydrothorax/hydromediastinum | Infusion into the pleural/mediastinal space from malposition |
| Chylothorax | Injury to the thoracic duct on left-sided attempts |
| Thrombosis | Femoral lines have the highest thrombosis rate (nearly 20% in some studies) |
Late
| Complication | Notes |
|---|---|
| Catheter-associated infection / CLABSI | Femoral site has the highest infection rate; strict aseptic technique is the key prevention |
| Catheter occlusion | From blood backflow or fibrin sheath |
| Venous thrombosis/thromboembolism | DVT risk proportional to duration and site |
| Catheter fracture/embolism | Rare; more common with implanted ports |
| Right atrial/great vessel perforation | Can cause hemopericardium and tamponade |
10. Prevention of Complications
Infection Prevention (CLABSI Bundle)
- Strict maximal sterile barrier precautions
- Chlorhexidine skin antisepsis
- Avoid femoral site when possible
- Remove catheter as soon as no longer needed
- Catheter tunnelling (as in Hickman lines) reduces infection risk
- Biopatch (chlorhexidine disc) at insertion site provides local antisepsis for 7 days
- Dated sterile transparent dressing; change every 7 days or when soiled/loose
- Review of necessity daily
Recent evidence: A 2024 meta-analysis (Boulet et al., Crit Care 2024, PMID 39563416) found that ultrasound guidance significantly reduces catheter-related infections compared to the landmark technique.
Pneumothorax Prevention
- Use US guidance, especially for subclavian lines
- Long-axis approach for the subclavian vein
- Do not attempt bilateral subclavian access without ruling out ipsilateral pneumothorax first
11. Securing and Dressing
From Roberts & Hedges' Clinical Procedures in Emergency Medicine:
- A rubber clamp is placed over the catheter a few centimeters from the insertion site
- Covered with a blue plastic fastener; both are sutured to skin
- The catheter hub is also sutured to skin
- Alternatively, skin staples may be used through anchoring eyes
- Biopatch (chlorhexidine hydrophilic disc) placed at skin entry site for 7 days of local antisepsis
- A clear Tegaderm dressing is applied over the entire site
- CXR is obtained to confirm tip position at the SVC level
12. Special Types and Long-Term Devices
Hickman Line (Tunnelled)
- Cuffed Silastic catheter tunnelled subcutaneously
- Dacron cuff placed halfway along the tunnel acts as a bacterial barrier; it becomes fixed by fibrosis
- Extravascular cuff placement: if placed at the mouth of the tunnel, it seals easily and is simpler to remove; if halfway, it requires more dissection at the end of treatment
- Inserted via cephalic, external jugular, or internal jugular vein
- Used for: prolonged chemotherapy, bone marrow transplantation, long-term TPN
Implantable Port
- Totally subcutaneous; accessed by needle puncture through skin
- Lowest infection rate
- Preferred for intermittent use
Haemodialysis Catheter
- Large-bore, dual-lumen tunnelled line
- Placed in the IJV or subclavian; tip in the SVC/right atrium
13. Paediatric Considerations (Harriet Lane Handbook)
- Choice of catheter size is based on primary disease, intended use, and the child's age, weight, and height
- Femoral access is often the site of choice in infants/small children when other sites are more difficult
- Paediatric indications include inability to obtain peripheral IV access, hemodynamic monitoring, administration of vasopressors, chemotherapy, and TPN (see Pediatric Table 114-3 in Tintinalli's)
14. Site Comparison Summary
| Feature | Internal Jugular | Subclavian | Femoral |
|---|---|---|---|
| Ease of US guidance | Excellent | Moderate (clavicle shadow) | Good |
| Pneumothorax risk | Low | Highest (1-3%) | None |
| Infection risk | Moderate | Low | Highest |
| Thrombosis risk | Moderate | Low | Highest (~20%) |
| Arterial compressibility | Yes (manual) | No | Yes (manual) |
| Use in coagulopathy | Preferred | Avoid | Acceptable |
| Long-term use | Acceptable | Best | Avoid |
| Use in cardiac arrest | Difficult | Difficult | Easiest access |
Sources
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide, Chapter 31 (Central Venous Access and Anatomy, US Technique)
- Roberts & Hedges' Clinical Procedures in Emergency Medicine, Chapter 22 (Central Venous Catheterization, Securing a CVC)
- Murray & Nadel's Textbook of Respiratory Medicine (Ultrasound-guided CVC Placement)
- Pye's Surgical Handicraft, 22nd Edition (Central Venous Access, Tunnelled Lines)
- The Harriet Lane Handbook, 23rd Edition (Paediatric CVC)
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9e (Indications in perioperative monitoring)
Recent literature note: A 2024 systematic review/meta-analysis (Boulet N et al., Crit Care 2024; PMID 39563416) confirms that ultrasound guidance during CVC insertion significantly reduces catheter-related infections vs. the traditional landmark technique. A 2024 systematic review in pediatric oncology (Christison-Lagay et al., J Pediatr Surg 2024; PMID 38637207) provides updated guidance on CVC selection in children with cancer.
This is a shared conversation. Sign in to Orris to start your own chat.