Exercise to train Pelvic drop and also assement and which muscle and how it affects pelvis
Reading File
Finding Sources
Finding Sources
Searching Images
pelvic drop Trendelenburg test hip abductor muscles
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
I have all the information needed from the textbooks. Now let me compile a comprehensive answer.
Pelvic Drop — Muscles, Assessment & Training
What Is Pelvic Drop?
Pelvic drop (also called contralateral pelvic sag) is the descent of the non-stance side of the pelvis during the single-leg stance phase of gait. Normally, during walking, the pelvis moves 6–10° in the frontal plane — pelvic drop on the swing side is controlled by the stance-side hip abductor muscles. When these muscles fail, excessive drop occurs.
"Pelvic motions in the frontal plane are described as pelvic drop and pelvic hike. The total excursion for this motion is approximately 6 to 10 degrees at preferred walking speed." — Imaging Anatomy Text and Atlas Vol. 3
Muscles Involved
Primary Stabilizers (prevent pelvic drop)
| Muscle | Origin | Insertion | Nerve | Key Role |
|---|---|---|---|---|
| Gluteus Medius | External ilium (between anterior & posterior gluteal lines) | Lateral surface of greater trochanter | Superior gluteal nerve (L4, L5, S1) | PRIMARY stabilizer — eccentrically controls pelvic tilt during midstance |
| Gluteus Minimus | External ilium (between inferior & anterior gluteal lines) | Anterolateral greater trochanter | Superior gluteal nerve (L4, L5, S1) | Works with medius to secure pelvis over stance leg |
Both muscles:
- Abduct the femur at the hip
- Hold the pelvis secure over the stance leg and prevent pelvic drop on the opposite swing side during walking
- Medially rotate the thigh
"The gluteus medius and minimus muscles abduct the lower limb at the hip joint and reduce pelvic drop over the opposite swing limb during walking by securing the position of the pelvis on the stance limb." — Gray's Anatomy for Students
Secondary Stabilizers
| Muscle | Role |
|---|---|
| Hip Adductors | Eccentric control of lateral sway in late stance |
| Quadratus Lumborum (ipsilateral) | Lifts the pelvis (pelvic hike) — compensates when abductors fail |
| TFL / IT band | Assists abduction and lateral stabilization |
Gait Table (from Miller's Orthopaedics)
| Phase | Muscle | Action | Function |
|---|---|---|---|
| Midstance | Gluteus medius | Eccentric | Controls pelvic tilt |
| Midstance | Gluteus maximus | Concentric | Powers hip extension |
| Late stance | Hip adductors | Eccentric | Control lateral sway |
How Weakness Affects the Pelvis
When the gluteus medius/minimus are weak on the stance leg:
- The contralateral (swing) side pelvis drops below horizontal
- To compensate, the patient lurches the trunk toward the stance leg (Trendelenburg lurch / compensated gait)
- In bilateral weakness → waddling gait
Causes of weakness leading to pelvic drop:
- Superior gluteal nerve injury (e.g., from pelvic fracture, hip surgery, sciatic foramen lesions)
- Hip OA / arthroplasty
- Neuromuscular disease
- Deconditioning / disuse
Assessment: Trendelenburg Test
How to perform:
- Patient stands with both hands on hips or examiner observes from behind
- Ask patient to lift one foot off the ground (single-leg stance on the limb being tested)
- Observe the pelvis level
Interpretation:
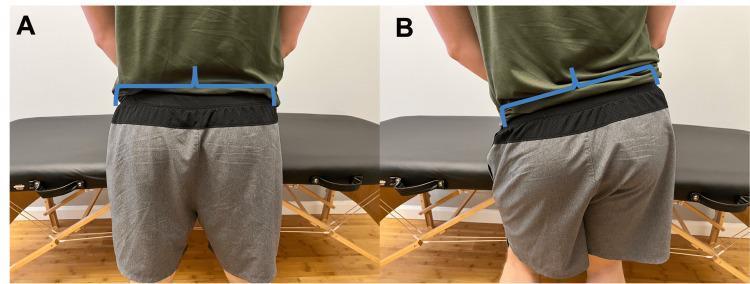
- Negative (normal): Pelvis remains level or the non-stance side rises slightly — abductors functioning
- Positive (abnormal): Pelvis drops on the non-stance (swing) side — indicates weakness of the stance-side abductors
"When the patient stands on the affected limb, the pelvis severely drops over the swing limb." — Gray's Anatomy for Students

Additional gait observation:
- Watch during walking for the trunk sway (Trendelenburg lurch) at midstance
- Compensated gait: lateral trunk lean to the affected side during stance to reduce the moment arm acting on the weakened abductors
Training Exercises for Pelvic Drop
Exercises are progressed from non-weight-bearing isolation → weight-bearing control → dynamic functional tasks.
Stage 1 — Isolation (Non-Weight-Bearing)
| Exercise | Technique | Target |
|---|---|---|
| Side-lying hip abduction | Lie on side, top leg straight; lift 30–40° keeping pelvis neutral | Gluteus medius isolation |
| Clamshell | Side-lying, hips flexed ~45°, knees bent; rotate top knee up keeping feet together | Gluteus medius + external rotators |
| Side-lying abduction with resistance band | Same as above with a band around thighs | Progressive overload |
Stage 2 — Static Weight-Bearing
| Exercise | Technique | Target |
|---|---|---|
| Single-leg stance | Stand on one leg for 30–60 sec; keep pelvis level (do NOT allow drop) | Neuromuscular control |
| Lateral band walk | Resistance band around ankles/knees; step laterally in squat position | Gluteus medius, TFL |
| Step-up with pelvic control | Step up onto a box, drive the hip of the free leg up into a level pelvis | Functional abductor loading |
Stage 3 — Dynamic / Eccentric Control
| Exercise | Technique | Target |
|---|---|---|
| Hip hike / pelvic drop on step (key exercise) | Stand on edge of step on one leg; intentionally lower the non-stance hip below step level, then raise it back level — controlled eccentric + concentric | Direct training of pelvic drop mechanism |
| Single-leg squat | Controlled descent on one leg; monitor pelvis stays level in mirror | Eccentric gluteus medius under load |
| Lateral step-down | Stand sideways on step; lower non-stance foot to ground slowly | Eccentric gluteus medius |
| Reverse lunge | Step backward, keep pelvis neutral throughout | Functional hip abductor + extensor |
Stage 4 — Functional / Gait Retraining
| Exercise | Technique |
|---|---|
| Treadmill gait retraining with mirror/video | Visual feedback to consciously correct pelvic drop during walking |
| Single-leg balance on unstable surface | Bosu ball / foam pad to challenge proprioception |
| Running drills (high knees, A-march) | Emphasize pelvic level and arm drive for runners |
Key Clinical Points
- The pelvic drop exercise on a step most directly mimics the gait demand — it trains the gluteus medius eccentrically during the controlled drop and concentrically during the raise
- Hands on hips or ASIS palpation during exercises helps provide biofeedback on pelvic leveling
- Weakness of gluteus medius also loads the IT band, patellofemoral joint, and lumbar spine — addressing pelvic drop is central to many lower limb pain syndromes (runner's knee, IT band syndrome, low back pain)
- The superior gluteal nerve runs ~5 cm proximal to the greater trochanter — injury here causes Trendelenburg gait from pure gluteal dysfunction
"Superior gluteal nerve approximately 5 cm proximal to greater trochanter. Injury leads to Trendelenburg gait from gluteal dysfunction." — Miller's Review of Orthopaedics
Sources: Gray's Anatomy for Students | Miller's Review of Orthopaedics | Imaging Anatomy Text & Atlas Vol. 3 | Schwartz's Principles of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.