What is LVF
Reading File
Finding Sources
Searching the Web
left ventricular failure LVF causes symptoms treatment
Reading File
Reading File
Finding Sources
Loading Image
Here is a thorough overview of Left Ventricular Failure (LVF):
Left Ventricular Failure (LVF)
LVF occurs when the left ventricle (LV) fails to pump blood effectively to the systemic circulation, leading to a backup of pressure into the pulmonary veins and lungs.
Definition & Pathophysiology
LVF is dysfunction of the left ventricle causing insufficient delivery of oxygenated blood to vital organs. When the LV fails:
- Blood backs up into the left atrium and then the pulmonary veins
- Elevated pulmonary venous pressure forces fluid into the interstitium and alveoli (pulmonary edema)
- The body compensates via sympathetic activation and neurohormonal mechanisms (RAAS activation, ADH release)
- Compensatory cycles of fluid retention, sympathetic activation, and further LV dysfunction cause progressive deterioration
Classification by Ejection Fraction
| Type | LVEF | Description |
|---|---|---|
| HFrEF (reduced EF) | ≤40% | Systolic failure - LV cannot contract forcefully enough |
| HFmrEF (mildly reduced) | 41-49% | Intermediate group |
| HFpEF (preserved EF) | ≥50% | Diastolic failure - LV cannot relax/fill properly |
HFpEF now accounts for about 50% of all heart failure cases. An additional group, HFimpEF, includes patients whose EF was ≤40% but improved with treatment.
Common Causes
- Coronary artery disease / myocardial infarction (most common)
- Hypertension (leads to LV hypertrophy)
- Dilated cardiomyopathy
- Valvular heart disease (aortic stenosis, mitral regurgitation)
- Myocarditis
- Arrhythmias
Signs and Symptoms
(from Miller's Anesthesia, 10e)
| Symptoms | Signs |
|---|---|
| Dyspnea on exertion | Basilar rales (crackles) |
| Paroxysmal nocturnal dyspnea (PND) | Pulmonary edema |
| Orthopnea | S3 gallop rhythm |
| Tachycardia | Pleural effusion |
| Hemoptysis (pink frothy sputum) | Cheyne-Stokes respiration |
In advanced disease, fatigue, poor exercise tolerance, and signs of low cardiac output (cool peripheries, hypotension, poor urine output) may dominate.
Diagnosis
- ECG - may show LV hypertrophy, ischemic changes, arrhythmia
- Echocardiography (TTE) - most useful initial test; measures LVEF, wall motion, valve function
- BNP >35 pg/mL or NT-proBNP >125 pg/mL - elevated in heart failure, especially HFpEF
- Chest X-ray - shows cardiomegaly, pulmonary venous congestion, interstitial/alveolar edema
- Blood tests - renal function, electrolytes, FBC, thyroid function
Treatment (AHA/ACC 2022 Guidelines)
Acute LVF (pulmonary edema):
- Sit upright, supplemental oxygen
- IV furosemide (loop diuretic)
- Morphine (relieves dyspnea and reduces preload/anxiety)
- Vasodilators (GTN/nitrates) to reduce preload
- Consider non-invasive ventilation (CPAP/BiPAP)
Chronic HFrEF (4 foundational "pillars"):
- ARNI (sacubitril/valsartan) or ACEi/ARB
- Beta-blocker (bisoprolol, carvedilol, metoprolol succinate)
- MRA (mineralocorticoid receptor antagonist, e.g. spironolactone)
- SGLT2 inhibitor (dapagliflozin, empagliflozin)
- Diuretics as needed for fluid congestion
Device therapies (selected patients):
- ICD - for LVEF ≤35% with >1 year expected survival (sudden death prevention)
- CRT-D - cardiac resynchronization therapy for LVEF ≤35% + LBBB + QRS ≥150 ms
Advanced/refractory HF:
- Durable mechanical circulatory support (LVAD)
- Cardiac transplant
- Palliative care
Treatment Pathway (HFrEF)
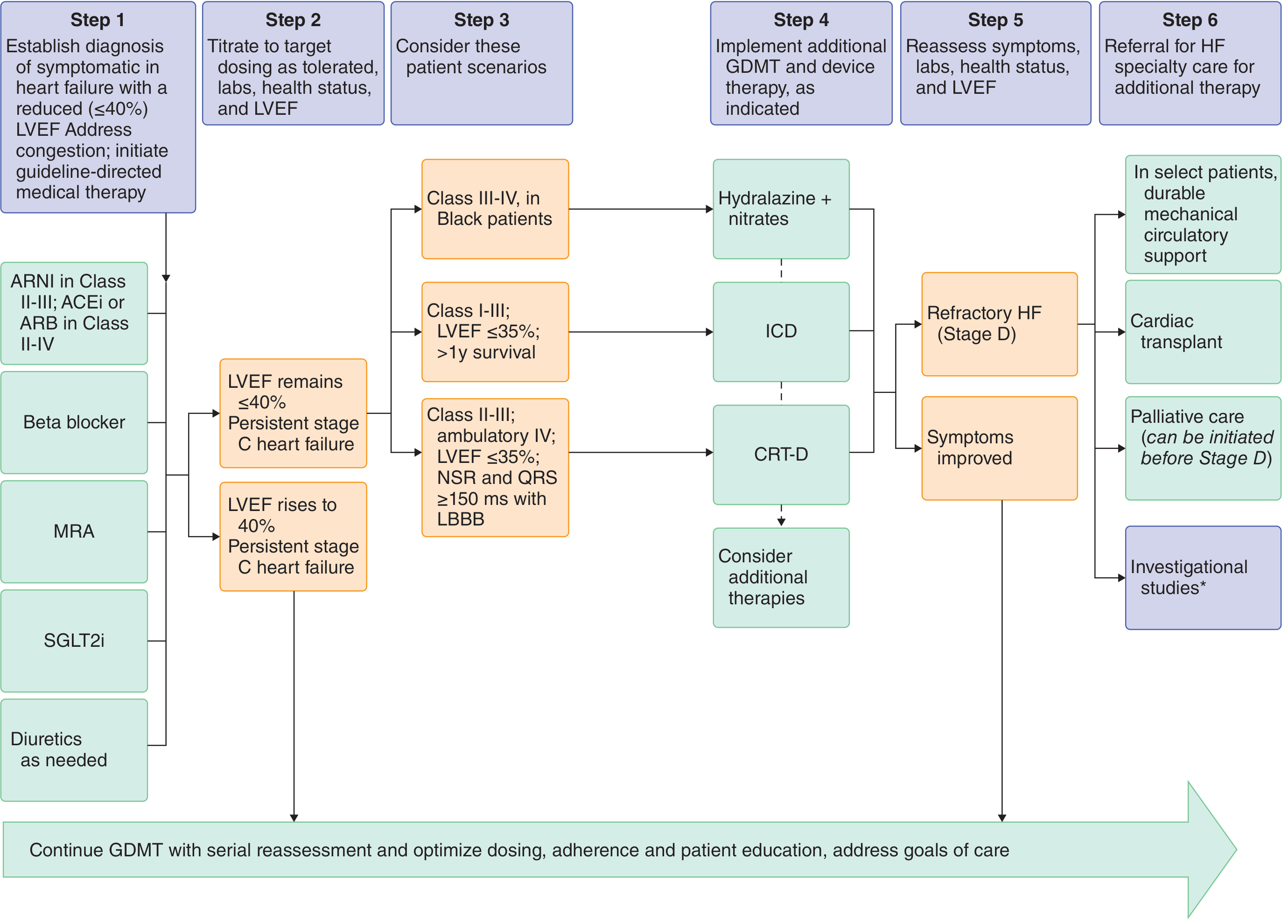
Goldman-Cecil Medicine - AHA/ACC/HFSA 2022 Guideline approach to Stage C HFrEF
Complications
If untreated, LVF leads to:
- Right ventricular failure (biventricular/congestive heart failure) - the increased pulmonary pressure eventually strains the right ventricle
- Cardiogenic shock
- Renal failure (cardiorenal syndrome)
- Arrhythmias and sudden cardiac death
Sources: Miller's Anesthesia 10e; Goldman-Cecil Medicine; Fuster & Hurst's The Heart 15e; StatPearls - Left Ventricular Failure; AHA - Types of Heart Failure
This is a shared conversation. Sign in to Orris to start your own chat.