A 45-year-old male presents with chronic low back pain and stiffness, which is worse in the morning and improves with activity. On examination, there is decreased lumbar lordosis, restricted spinal mobility, and tenderness over the paraspinal muscles. Additionally, Schober's test reveals limited lumbar flexion. Diagnose this case write its deatil ICf(body structure impairment,investigation,clinical reasoning) (body function impairment,investigationclinicalr reasoning more detailed physiotherapy management with short term goals and long term goals with dosage. Take Reference from-Stanley Hoppenfeld and Brotzman
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have sufficient information from the textbook sources. Let me compile the comprehensive ICF-based clinical report on Ankylosing Spondylitis.
Ankylosing Spondylitis (AS) — Comprehensive ICF-Based Clinical Report
Reference Sources: Goldman-Cecil Medicine; Grainger & Allison's Diagnostic Radiology; Murray & Nadel's Respiratory Medicine; Stanley Hoppenfeld (Orthopaedic Physical Examination); Brotzman (Clinical Orthopaedic Rehabilitation)
DIAGNOSIS
Ankylosing Spondylitis (AS) — Axial Spondyloarthropathy
This 45-year-old male presents with the cardinal triad of AS:
- Chronic inflammatory low back pain (>3 months duration)
- Morning stiffness improving with activity (not rest — distinguishing from mechanical back pain)
- Restricted spinal mobility with decreased lumbar lordosis and positive Schober's test
The pattern fits the modified New York Criteria for AS: inflammatory back pain, limited lumbar motion in sagittal and frontal planes, and limited chest expansion, with sacroiliac involvement on imaging.
"Ankylosing spondylitis is diagnosed when there is a history of low back pain and stiffness for more than 3 months, limited chest wall expansion (<2.5 cm at the fourth intercostal space), limited lumbar spine motion in the sagittal and frontal planes, and radiographic evidence of sacroiliitis." — Goldman-Cecil Medicine
PART 1 — ICF: BODY STRUCTURE IMPAIRMENTS
1.1 Sacroiliac Joints (b7 — Neuromusculoskeletal and Movement-Related Functions)
Structure Impaired: Bilateral sacroiliac joints — cartilage, subchondral bone, joint capsule
Pathological Change: Enthesitis → synovitis → subchondral erosions → fibrosis → bony ankylosis
- Sacroiliitis is the hallmark of AS; it is bilateral and symmetrical
- Progresses from erosive sacroiliitis → partial ankylosis → complete bony fusion
Investigations:
| Investigation | Finding |
|---|---|
| X-ray pelvis (AP view) | Bilateral sacroiliac erosions, subchondral sclerosis, joint space loss, eventual fusion |
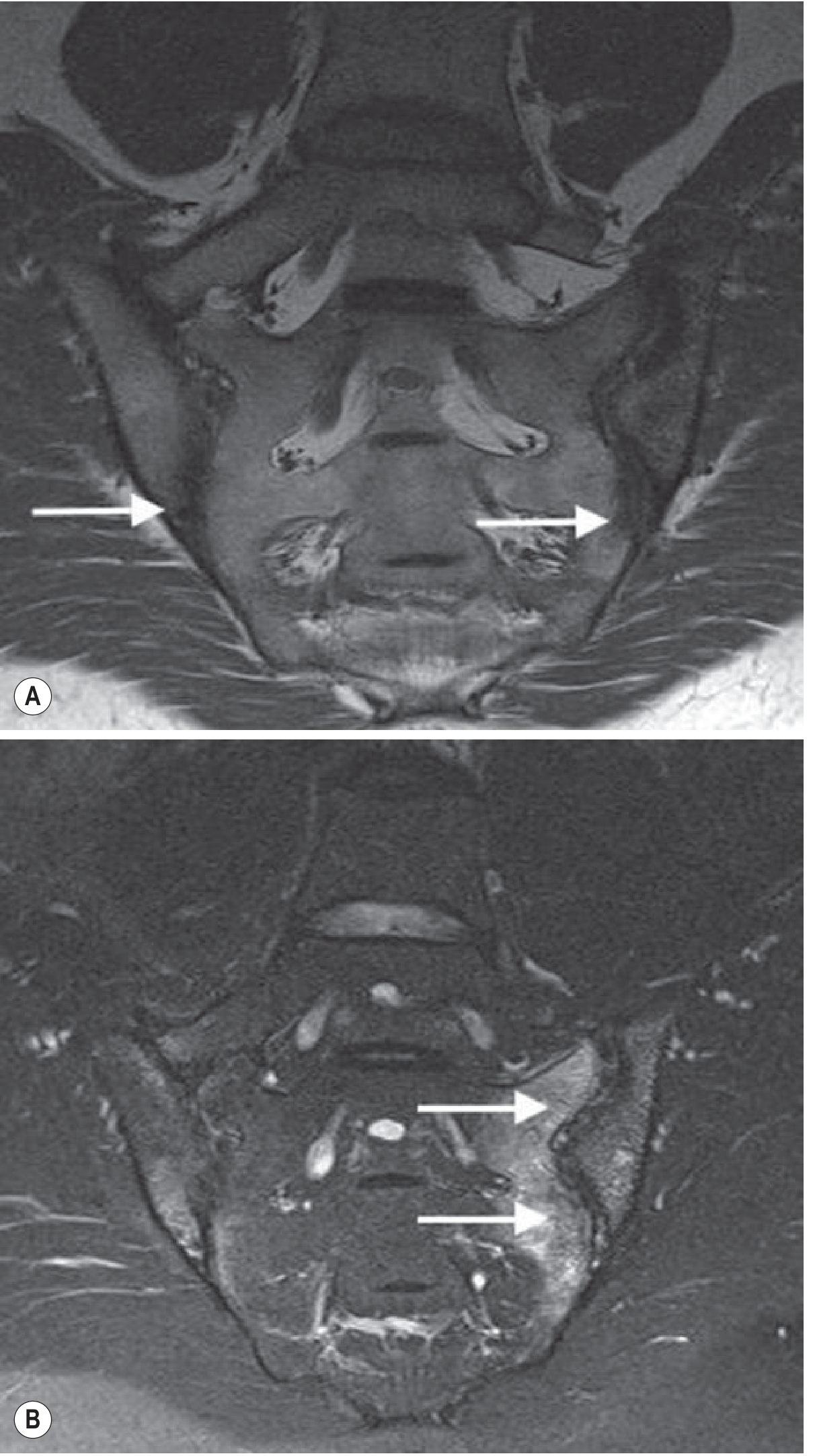
| MRI sacroiliac joints (STIR/T2 fat-suppressed) | Gold standard for early disease — subchondral bone marrow oedema precedes X-ray changes |
| CT pelvis | Detailed erosions and fusion; limited for early inflammatory activity |
| HLA-B27 | Positive in ~95% of White AS patients |
| CRP / ESR | Elevated during active inflammation |
Clinical Reasoning: Sacroiliac inflammation triggers the early morning pain and stiffness. Inflammatory cytokines (TNF-α, IL-17) are released during rest/inactivity causing stiffness that improves with movement due to increased synovial fluid circulation and reduced cytokine concentration.
"Sacroiliitis and enthesitis of the axial skeleton is the hallmark of AS. The earliest feature of sacroiliitis is detected with MRI as subchondral bone marrow oedema." — Grainger & Allison's Diagnostic Radiology
MRI of Sacroiliac Joints in AS:
1.2 Lumbar Spine (Discovertebral Unit, Facet Joints, Posterior Elements)
Structure Impaired: Vertebral bodies, intervertebral discs, facet joints, anterior longitudinal ligament, Sharpey fibres (annulus fibrosus insertion)
Pathological Change:
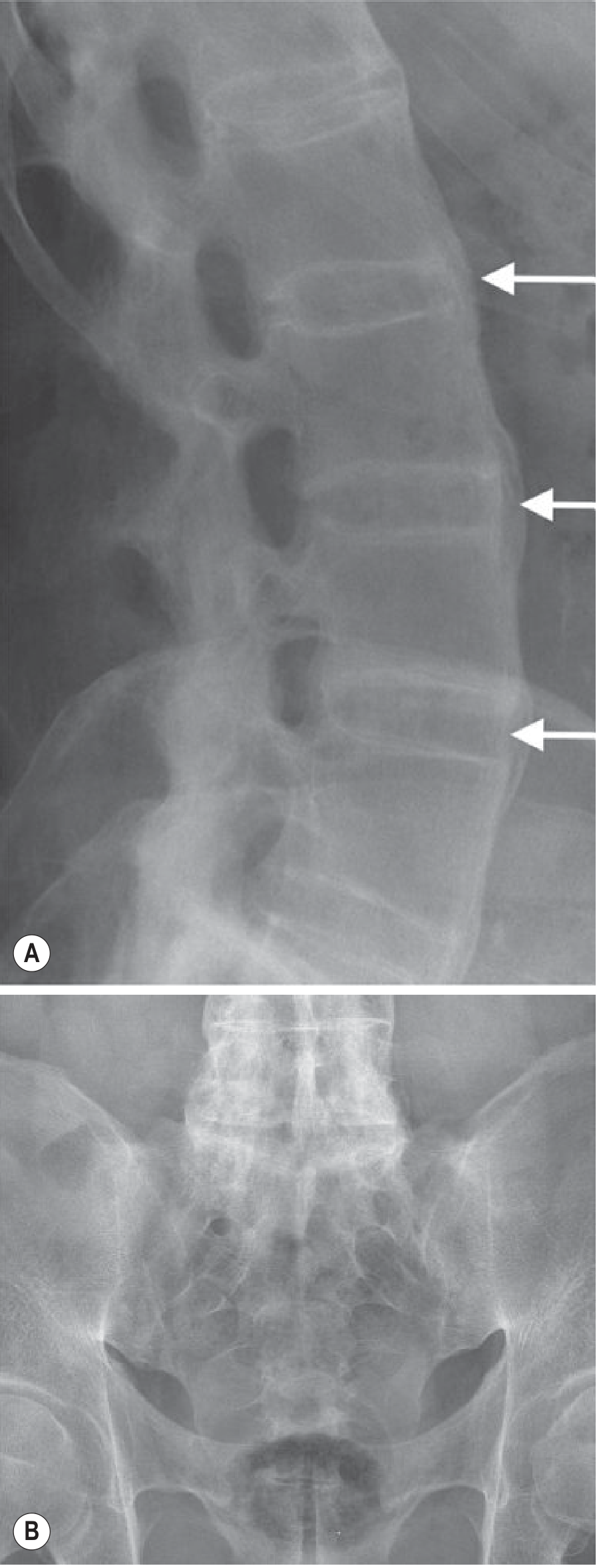
- Romanus lesions: Enthesitis at insertion of Sharpey fibres → sclerotic "shiny corners" on lateral X-ray
- Syndesmophytes: Thin vertical bone outgrowths at vertebral corners → bridging → Bamboo spine (complete fusion)
- Facet joint ankylosis restricts all planes of spinal movement
- Decreased lumbar lordosis due to paraspinal muscle spasm and structural flattening
Investigations:
| Investigation | Finding |
|---|---|
| X-ray lumbosacral spine (lateral view) | Shiny corners (Romanus lesions), squared vertebrae, syndesmophytes |
| MRI lumbar spine | Bone marrow oedema at vertebral corners before X-ray changes; entheseal oedema at facet joints and spinous processes |
| STIR MRI | Active inflammatory oedema at costovertebral joints |
Clinical Reasoning (Hoppenfeld): Physical examination of the lumbar spine in AS reveals:
- Decreased lumbar lordosis: Paraspinal muscle spasm + structural flattening of vertebral bodies
- Schober's Test: Modified Schober's — mark 10 cm above and 5 cm below S1 dimple; <5 cm increase on full flexion = abnormal (normal >5 cm). Indicates restricted lumbar intersegmental movement from facet joint and disc ankylosis
- Loss of lateral flexion and rotation from facet joint involvement
Bamboo Spine X-ray (Advanced AS):
1.3 Paraspinal Muscles and Entheses
Structure Impaired: Erector spinae, multifidus, thoracolumbar fascia insertion points
Pathological Change: Enthesitis (inflammation at bone-tendon/ligament interface) → paraspinal muscle guarding and spasm → progressive atrophy from disuse
Investigations:
| Investigation | Finding |
|---|---|
| MRI (STIR) | Entheseal soft-tissue oedema at paraspinal insertions |
| Ultrasound | Power Doppler shows entheseal vascularity and thickening |
| CRP/IL-17 | Marker of ongoing entheseal inflammation |
1.4 Rib Cage / Costovertebral Joints (In Advanced Disease)
Structure Impaired: Costovertebral and costo-sternal joints, anterior chest wall
Pathological Change: Enthesitis at costovertebral joints → fusion → rib cage fixed in inspiratory position → restrictive lung disease
Investigation: STIR MRI of thoracic spine (extends to costovertebral joints bilaterally); Chest expansion measurement (<2.5 cm at 4th ICS = significant)
Clinical Reasoning:
"Fusion of the costovertebral and sternoclavicular joints produces relative fixation of the rib cage in an inspiratory position... Intercostal muscle atrophy secondary to decreased rib cage mobility may cause inspiratory muscle weakness." — Goldman-Cecil Medicine
PART 2 — ICF: BODY FUNCTION IMPAIRMENTS
2.1 b7100 — Mobility of a Single Joint (Lumbar Spine, SI Joint)
Impairment: Restricted lumbar flexion, extension, lateral flexion, rotation
Measurement / Investigation:
- Modified Schober's Test: <5 cm increase = restricted lumbar flexion
- BASMI (Bath AS Metrology Index): Measures tragus-to-wall distance, lumbar side flexion, modified Schober's, cervical rotation, intermalleolar distance — validated AS-specific mobility tool
- Goniometry: ROM measurement in all lumbar planes
- Finger-to-floor distance: Assesses composite lumbar + hip flexion
Clinical Reasoning: In early AS, restricted mobility is due to pain and muscle guarding (reversible). As disease progresses, structural ankylosis of facet joints and formation of syndesmophytes produces irreversible mechanical restriction. Schober's test specifically isolates lumbar segmental mobility from hip flexion.
2.2 b7101 — Mobility of Multiple Joints / Stiffness
Impairment: Morning stiffness lasting >1 hour; gel phenomenon
Measurement: BASDAI Q1–Q2 (Bath AS Disease Activity Index) scores stiffness on a 0–10 NRS; duration of morning stiffness (>45 min = active disease)
Clinical Reasoning: During inactivity, inflammatory exudate accumulates within affected joints. Physical activity mobilises synovial fluid, disperses inflammatory mediators, and reduces pain — explaining why this patient's stiffness improves with movement (classic inflammatory pattern, distinguishing from mechanical LBP where rest relieves symptoms).
2.3 b7300 — Power of Isolated Muscles / Muscle Groups
Impairment: Paraspinal muscle weakness and atrophy; reduced core stability; hip extensor and abductor weakness
Measurement:
- Manual Muscle Testing (MMT) — erector spinae, gluteus maximus, hip abductors
- Pressure biofeedback unit — transversus abdominis and lumbar multifidus activation
- Dynamometry — quantify lumbar extensor torque
Clinical Reasoning: Chronic enthesitis and pain → reflex inhibition of paraspinal muscles → disuse atrophy → loss of dynamic spinal stabilisation. Multifidus and transversus abdominis are specifically impaired in lumbar inflammatory conditions (Brotzman), contributing to recurrent pain cycles.
2.4 b280 — Sensation of Pain
Impairment: Chronic inflammatory pain — diffuse axial, worse at night and early morning; bilateral SI joint tenderness; paraspinal tenderness
Measurement:
- VAS / NRS (0–10): Pain at rest, with activity, at worst
- BASDAI (Bath AS Disease Activity Index) — composite score including pain and stiffness subscales
- ASDAS (AS Disease Activity Score) — incorporates CRP; score >2.1 = high disease activity
Clinical Reasoning: Inflammatory cytokines (TNF-α, IL-17, IL-23) sensitise peripheral nociceptors at entheseal sites. Neuropeptides (substance P) propagate central sensitisation. The characteristic night pain/morning stiffness is driven by circadian variation in cortisol and inflammatory cytokine peaks during the early morning hours.
2.5 b4400–b4402 — Respiratory Functions
Impairment: Reduced chest expansion → restrictive ventilatory pattern; diaphragmatic overcompensation; reduced aerobic capacity
Measurement:
- Chest expansion at 4th ICS (<2.5 cm = significant)
- Pulmonary Function Tests (PFTs): FVC, FEV1/FVC, TLC — restrictive pattern
- 6-Minute Walk Test (6MWT) — functional aerobic capacity
Clinical Reasoning: Costovertebral fusion fixes the rib cage in inspiration. The diaphragm compensates with increased excursion, raising its work. Intercostal muscles atrophy. This compounds with thoracic kyphosis in advanced disease to further reduce lung volumes.
2.6 b7600 — Control of Voluntary Movement / Posture
Impairment: Altered postural alignment — loss of lumbar lordosis, progressive thoracic kyphosis, forward head posture, compensatory hip flexion contracture
Measurement:
- Tragus-to-wall distance (normal <15 cm)
- Occiput-to-wall distance (0 cm normal; any positive = cervical kyphosis)
- Sagittal vertical axis (SVA) on full-length standing X-ray
- Plumb-line analysis; photographic posture assessment
Clinical Reasoning (Hoppenfeld): The classic AS posture develops as: sacroiliac ankylosis → loss of lumbar lordosis → compensatory thoracic hyperkyphosis → forward-shifted centre of gravity → progressive functional disability. Hip flexors shorten adaptively to maintain forward balance.
PART 3 — PHYSIOTHERAPY MANAGEMENT
SHORT-TERM GOALS (0–6 Weeks)
| # | Goal | Target | Outcome Measure |
|---|---|---|---|
| STG 1 | Reduce pain to ≤3/10 NRS at rest | 6 weeks | VAS/NRS, BASDAI |
| STG 2 | Reduce morning stiffness duration by 50% | 6 weeks | BASDAI Q1–Q2 |
| STG 3 | Improve lumbar flexion by 2 cm on Schober's test | 6 weeks | Modified Schober's |
| STG 4 | Improve chest expansion by 1 cm | 6 weeks | Tape measurement at 4th ICS |
| STG 5 | Achieve painfree ROM in lumbar extension and lateral flexion | 6 weeks | Goniometry |
| STG 6 | Patient educated in home exercise programme and sleep positioning | 2 weeks | Education checklist |
LONG-TERM GOALS (3–6 Months and Beyond)
| # | Goal | Target | Outcome Measure |
|---|---|---|---|
| LTG 1 | Achieve BASDAI score <4 (low/inactive disease) | 6 months | BASDAI |
| LTG 2 | Maintain or improve spinal mobility — BASMI improvement ≥1 point | 6 months | BASMI |
| LTG 3 | Achieve symmetrical posture — occiput-to-wall distance 0 cm | 6 months | Postural assessment |
| LTG 4 | Independent in daily stretching and strengthening HEP | 3 months | Adherence diary |
| LTG 5 | Return to full occupational function and social participation | 6 months | BASFI (Bath AS Functional Index) |
| LTG 6 | Aerobic capacity >400 m on 6MWT | 6 months | 6MWT |
| LTG 7 | Prevent further postural deformity — maintain neutral lordosis | Ongoing | Sagittal balance imaging |
DETAILED PHYSIOTHERAPY INTERVENTIONS WITH DOSAGE
A. PAIN MANAGEMENT PHASE (Weeks 1–2)
1. Hydrotherapy / Aquatic Physiotherapy
- Rationale: Warm water reduces pain, aids joint mobility, unloads spine. Highly evidence-based in AS (ASAS guidelines).
- Dosage: 30–45 min/session, 3×/week
- Exercises: Spinal extension in water, lateral side-bends, pelvic tilts, walking
2. Superficial Heat (Hot Pack / Infrared)
- Rationale: Reduces muscle spasm; increases collagen extensibility before stretching
- Area: Lumbar paraspinals, thoracic spine
- Dosage: 20 minutes, pre-exercise, daily
3. TENS (Transcutaneous Electrical Nerve Stimulation)
- Type: Conventional TENS (high frequency 80–100 Hz, low intensity)
- Rationale: Gate control — reduces pain perception at dorsal horn
- Electrode placement: Paraspinal muscles L1–L5 bilaterally; over SI joints
- Dosage: 20–30 min/session, 1–2×/day during acute exacerbation
4. Ultrasound Therapy
- Area: SI joints, lumbar paraspinal entheses
- Parameters: Pulsed (1:4 duty cycle), 1 MHz, 0.5–1.0 W/cm², 5–8 min/area
- Dosage: 5 sessions/week × 2 weeks (acute phase)
B. FLEXIBILITY AND MOBILITY PHASE (Weeks 1–6, ongoing)
Based on Brotzman's principle of maintaining mobility before it is lost permanently to fibrosis and ossification.
5. Spinal Extension Exercises (PRIORITY in AS)
- Rationale: Counteracts the natural tendency toward flexion deformity (kyphosis). The deformity of AS, if it occurs, must be in maximum extension to preserve function.
- Exercises:
- Prone lying (passive extension stretch): Start 5 min → build to 20–30 min/day
- Prone press-ups (cobra stretch): Hold 10 sec × 10 reps
- Standing wall extension: Spine flat against wall, feet 30 cm away, head contact maintained
- "Wall standing" daily posture check (Hoppenfeld): Heels, buttocks, shoulders, occiput against wall — 5 min/day
- Dosage: 2–3×/day, 7 days/week (crucial — consistency matters more than intensity)
6. Chest Expansion Exercises (Respiratory Physiotherapy)
- Rationale: Prevents costovertebral ankylosis in fixed inspiration position; maintains vital capacity
- Exercises:
- Deep diaphragmatic breathing: 5 deep breaths × 5 sets/day
- Lateral costal breathing: Therapist applies resistance to lateral rib cage
- Incentive spirometry: 10 breaths × 3 sets, 2×/day
- Arm elevation with deep inspiration: 3×/day
- Dosage: Chest physiotherapy 15–20 min twice daily
7. Hip Flexor Stretching
- Rationale: Hip flexors shorten as compensation for lost lumbar lordosis (Hoppenfeld)
- Exercises:
- Thomas stretch position: 30-second holds × 3 reps, 2×/day
- Prone hip extension stretch
- Dosage: 2×/day, 5 days/week
8. Thoracic Spine Mobilisation
- Technique: Maitland Grades I–II (in acute phase) → Grades III–IV (subacute)
- Area: Thoracic facet joints, costovertebral joints
- Dosage: 3 sets × 30 sec/level, 3×/week
C. STRENGTHENING PHASE (Weeks 3–8)
9. Core Stabilisation (Transversus Abdominis + Multifidus)
- Rationale (Brotzman): Specific impairment of deep stabilisers in chronic inflammatory back pain. Restoring co-contraction protects the spine dynamically.
- Progression:
- Stage 1: Abdominal hollowing in supine (PBU target 4–10 mmHg below resting) × 10 sec holds × 10 reps
- Stage 2: Four-point kneeling arm/leg raises (bird-dog)
- Stage 3: Side plank, prone plank (progress as tolerated)
- Dosage: 3 sets × 10 reps, 3×/day
10. Gluteal and Hip Extensor Strengthening
- Exercises: Bridging, clamshell, prone hip extension with knee bent
- Dosage: 3 sets × 15 reps, 2×/day, 4×/week
11. Erector Spinae and Paraspinal Strengthening
- Exercises:
- Prone back extension (Superman) on mat: 3 × 10 reps
- Romanian deadlift (light resistance): 3 × 12 reps
- Pull-down exercises for thoracic extensor
- Dosage: 3×/week
12. Scapular Retractor and Upper Back Strengthening
- Rationale: Counteracts thoracic kyphosis and forward head posture
- Exercises: Rows, reverse flies, prone Y–T–W exercises
- Dosage: 3 sets × 12 reps, 3×/week
D. AEROBIC / CARDIOVASCULAR RECONDITIONING (Weeks 4–12)
13. Aerobic Exercise
- Preferred modalities: Swimming (MOST recommended — non-impact, promotes spinal extension), cycling (upright posture), walking
- Rationale: Improves cardiorespiratory fitness (impaired by restrictive chest), reduces systemic inflammation, improves 6MWT performance
- Target: 50–70% HRmax (moderate intensity)
- Dosage: 30 min/session, 3–5×/week
- Progression: Add 5 min/week until 45–60 min sustained
"Exercise and physiotherapy programs can enhance cardiorespiratory fitness and spinal mobility." — Goldman-Cecil Medicine
E. POSTURAL CORRECTION AND EDUCATION (Ongoing)
14. Postural Training
- Key principle (Hoppenfeld): Educate patient to maintain maximum extension. If the spine fuses, it must fuse in as straight a position as possible.
- Techniques:
- Wall-standing exercise (daily posture check against wall)
- Ergonomic advice: Firm mattress, low pillow, sleeping prone or supine (NOT side-lying fetal position)
- Workstation modification: Monitor at eye level, lumbar roll, standing desk intervals
- Avoid prolonged flexed postures (forward bending, stooping)
- Sleep posture education: Prone lying or supine with one pillow — prevents flexion contracture during prolonged nocturnal rest
15. Patient Education
- Disease process explanation and long-term course
- Importance of lifelong daily exercise — even during remission
- Warning signs of disease flare vs. fracture (catastrophic risk in fused rigid spine)
- Medication adherence (NSAIDs, biologics — TNF-α inhibitors) in conjunction with physiotherapy
- Joining AS support groups / NASS (National Ankylosing Spondylitis Society)
PRECAUTIONS IN PHYSIOTHERAPY
| Precaution | Rationale |
|---|---|
| Avoid high-impact contact sports | Rigid fused spine highly susceptible to transverse fractures with minimal trauma |
| No spinal manipulation (thrust techniques) | Risk of fracture through ossified fused spine |
| Avoid prolonged flexion exercises | Accelerates kyphotic deformity |
| Screen for atlantoaxial subluxation before cervical treatment | Cervical spine involvement in advanced AS |
| Monitor respiratory function | Restrictive ventilatory defect worsens with costovertebral fusion |
OUTCOME MEASURES SUMMARY
| Domain | Measure | Frequency |
|---|---|---|
| Disease activity | BASDAI (0–50), ASDAS | 4-weekly |
| Functional disability | BASFI (Bath AS Functional Index) | 4-weekly |
| Spinal mobility | BASMI (5-component index) | 4-weekly |
| Pain | NRS 0–10, BASDAI pain subscale | Weekly |
| Quality of life | ASQoL (AS Quality of Life) | 8-weekly |
| Aerobic capacity | 6-Minute Walk Test | Monthly |
| Chest expansion | Tape measure at 4th ICS | Monthly |
| Lumbar flexion | Modified Schober's test | Monthly |
MULTIDISCIPLINARY TEAM
- Rheumatologist: NSAIDs (first-line), TNF-α inhibitors (e.g., etanercept, adalimumab), IL-17 inhibitors (secukinumab) for refractory disease
- Physiotherapist: Core of management — spinal mobility, strengthening, aerobic conditioning, postural correction
- Occupational Therapist: Workstation ergonomics, adaptive aids, energy conservation
- Respiratory Physiotherapist: Chest expansion exercises, breathing training
- Orthopaedic Surgeon: Corrective osteotomy for severe kyphotic deformity; hip replacement for hip joint ankylosis
Key Clinical Pearl (Hoppenfeld / Brotzman):
In AS, physiotherapy is not adjunctive — it is a primary intervention. The disease will progress toward deformity if untreated, but the direction of that deformity can be influenced by consistent daily exercise. The therapeutic goal is to ensure that if ankylosis does occur, the spine fuses in maximum extension, preserving upright posture, vision, ambulation, and respiratory function.
This is a shared conversation. Sign in to Orris to start your own chat.