Melonoma medicine
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive content to provide a thorough answer. Here is a complete overview of melanoma medicine:
Melanoma (Malignant Melanoma)
Overview
Melanoma is the most lethal cutaneous malignancy, responsible for more than 77% of skin cancer deaths. It arises from melanocytes — pigment-producing cells found predominantly in skin, but also in the eyes, ears, GI tract, leptomeninges, and oral/genital mucous membranes. Almost half arise from preexisting nevi; the remainder develop on previously normal-appearing skin.
— Textbook of Family Medicine 9e
Risk Factors
- Fair complexion, light eyes, red or blond hair
- Inability to tan; predisposition to burn; heavy freckling
- Excessive childhood sun exposure; >3 blistering childhood sunburns
- Large number of common or dysplastic nevi
- Giant congenital nevi
- Family or personal history of melanoma
- Immunosuppression
- PUVA, tanning lamps, xeroderma pigmentosum
- BRAF gene mutations — frequent in melanomas on non-chronically sun-exposed skin in Caucasians
- KIT gene mutations / cyclin D1 amplification — associated with acral and mucosal lentiginous subtypes
— Andrews' Diseases of the Skin
Clinical Recognition — ABCDE Criteria
| Letter | Feature |
|---|---|
| A | Asymmetry |
| B | Border irregularity |
| C | Color variegation |
| D | Diameter >6 mm |
| E | Evolving (change over time) |
A changing or newly acquired nevus in a person over 20 is the most common warning sign. Bleeding, itching, ulceration, or pain in a pigmented lesion are less common but also warrant evaluation.
Subtypes
| Subtype | Frequency | Notes |
|---|---|---|
| Superficial spreading | 60–70% | Most common; occurs on trunk or legs |
| Nodular | 15–30% | Often solid black; thickness predicts poor prognosis |
| Lentigo maligna | 5–15% | Face in elderly; prolonged radial growth phase |
| Acral lentiginous | 5–10% | Great toe, thumb; most common in African Americans |
— Textbook of Family Medicine 9e
Diagnosis & Biopsy
- Excisional biopsy with 1–2 mm of surrounding normal skin is optimal
- "Scoop shave" biopsies are acceptable if specimen depth >1–2 mm
- Breslow depth (tumor thickness in mm) is the single most important prognostic indicator
- Staging also considers: ulceration (histologic), lymph node involvement, and metastasis site
- Thin tumors (Breslow <1 mm) carry >90% 10-year survival
Staging — Breslow Depth Summary
| Breslow Depth | Surgical Margin |
|---|---|
| <1 mm | 1 cm margin |
| 1–2 mm | 1–2 cm margin |
| >2 mm | 2 cm margin |
Sentinel lymph node biopsy (SLNB) is performed for lesions >1 mm, or <1 mm with ulceration or increased mitotic rate.
Treatment Algorithm
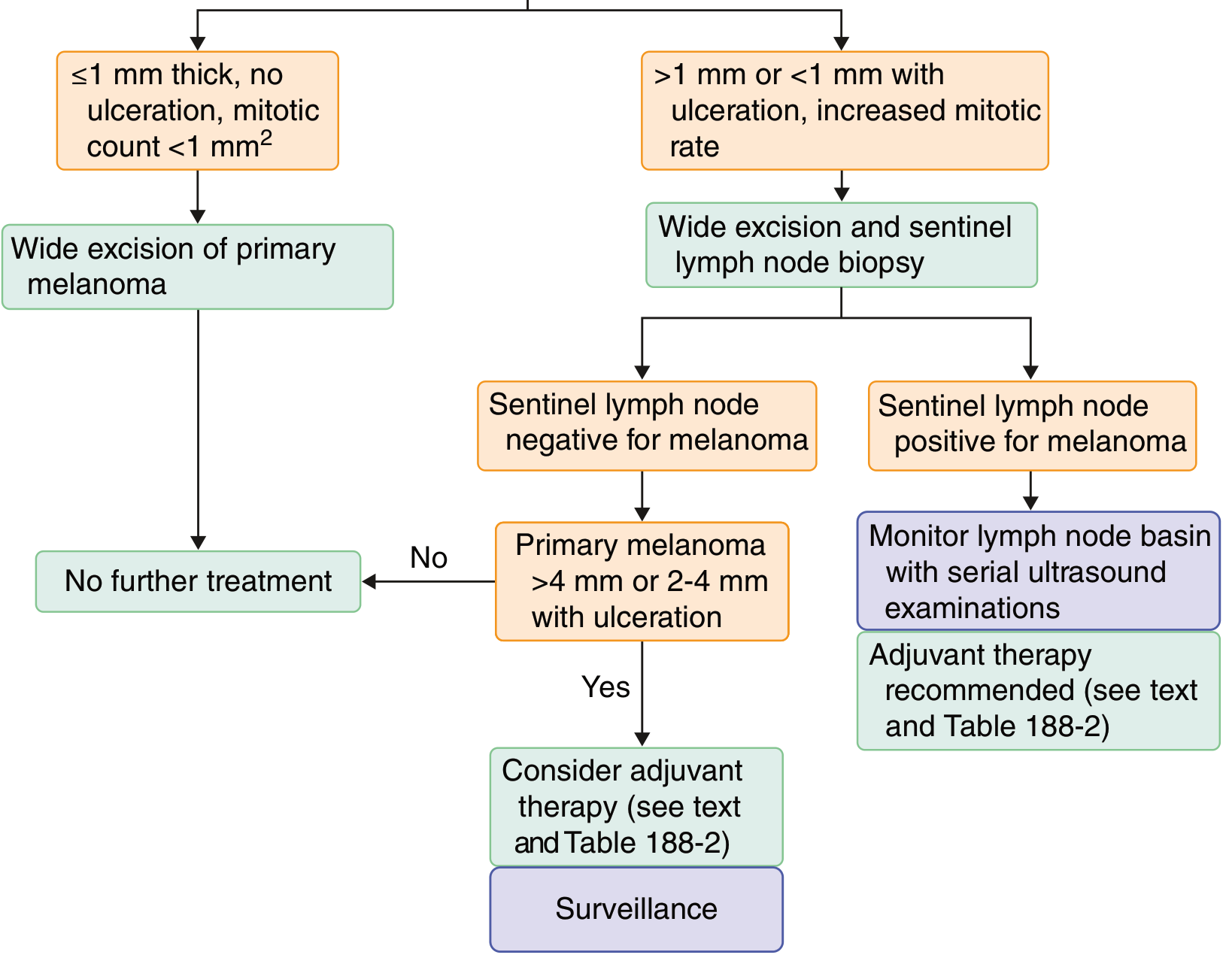
Goldman-Cecil Medicine — Treatment pathways for newly diagnosed melanoma
Key decision points:
- ≤1 mm, no ulceration, mitotic count <1/mm² → Wide local excision only; no further treatment
- >1 mm, or <1 mm with ulceration/high mitotic rate → Wide excision + SLNB
- SLNB negative + tumor >4 mm or 2–4 mm with ulceration → Consider adjuvant therapy + surveillance
- SLNB positive → Monitor lymph node basin with serial ultrasound + adjuvant therapy recommended
Adjuvant & Systemic Therapies
Immunotherapy
- Ipilimumab (anti-CTLA-4) — demonstrated improved survival in recalcitrant metastatic melanoma in phase III trials
- PD-1 inhibitors (nivolumab, pembrolizumab) — checkpoint blockade; mainstay of advanced disease
- High-dose interleukin-2 (IL-2) — older option; significant toxicity
Targeted Therapy
- BRAF inhibitors (vemurafenib, dabrafenib) — for BRAF V600E-mutant melanoma (~50% of cases)
- MEK inhibitors (trametinib, cobimetinib) — often combined with BRAF inhibitors to delay resistance
- KIT inhibitors (imatinib) — for KIT-mutant acral/mucosal melanomas
Radiation
- Adjuvant radiation considered for high-risk nodal disease or extensive regional involvement
Chemotherapy
- Dacarbazine (DTIC) — historically first-line; largely replaced by immunotherapy and targeted agents
- Temozolomide — oral alkylating agent with CNS penetration
Prognosis
- Stage I (thin, localized): >90% 5-year survival
- Stage III (nodal involvement): ~40–70% depending on burden
- Stage IV (distant metastasis): historically <10% 5-year survival; significantly improved with modern immunotherapy/targeted therapy combinations
Special Populations
- Pregnancy: Nevi often darken uniformly due to estrogen/progesterone receptor expression on melanocytes. Asymmetric or irregularly pigmented changes still warrant biopsy. Melanoma during pregnancy is associated with shorter disease-free intervals but no proven adverse effect on overall survival.
- Children: Melanoma is rare; occurs equally from normal skin and preexisting nevi. Diagnosis is often delayed due to low clinical suspicion.
- Darker skin types: Acral lentiginous is the predominant subtype; incidence of other subtypes is very low.
— Andrews' Diseases of the Skin; Textbook of Family Medicine 9e
This is a shared conversation. Sign in to Orris to start your own chat.