Meineiers disease etiopathologyand its management
Reading File
Finding Sources
Searching PubMed
"Meniere disease" AND management
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
I now have all the information needed for a comprehensive answer. Let me compose it.
Meniere's Disease (Ménière Disease)
Definition & Overview
Meniere's disease (MD) is a disorder of the inner ear characterized by the clinical tetrad of:
- Episodic spontaneous vertigo (lasting 20 minutes to several hours)
- Fluctuating sensorineural hearing loss (SNHL)
- Tinnitus (typically low-pitched "buzzing" or "roaring")
- Aural fullness/pressure
It is defined as idiopathic endolymphatic hydrops - when a known cause is identified, the condition is termed "secondary endolymphatic hydrops." About 85% of cases are unilateral; bilateral involvement can occur in up to 50% of patients within 20 years of onset.
- Cummings Otolaryngology Head and Neck Surgery, p. 3034
- K.J. Lee's Essential Otolaryngology, p. 76
Etiopathology
Histopathological Hallmark
The pathologic basis is distortion of the membranous labyrinth by endolymphatic hydrops - over-accumulation of endolymph within the scala media and saccule/utricle, which expands at the expense of the perilymphatic space. Reissner's membrane distends toward the scala tympani.
Mechanism of Endolymph Overaccumulation
Endolymph is produced by the stria vascularis (cochlea) and dark cells (vestibular labyrinth). It circulates in both radial and longitudinal directions and is reabsorbed primarily by the endolymphatic sac. The prevailing theory is:
Inadequate absorption of endolymph by the endolymphatic sac leads to hydrops. The endolymphatic duct may act as a regulatory valve. Experimental animal models confirm that surgical disruption of the endolymphatic sac induces hydrops. Imaging shows hypoplasia of the endolymphatic sac and duct, and reduced vestibular aqueduct size in MD patients, with these anatomic features developing as early as age 3 years.
How Attacks Are Generated (Schuknecht's Membrane Rupture Theory)
Ruptures in the distended membranous labyrinth allow potassium-rich endolymph to leak into the perilymph, bathing the hair cells and 8th nerve dendrites. High extracellular K⁺ depolarizes and then inactivates these nerve cells, producing:
- Acute hearing loss
- Vertigo (acute vestibular paralysis) Membrane healing restores normal ionic milieu, terminating the attack. Repeated episodes cause cumulative damage, explaining progressive hearing loss.
Etiological Theories
| Proposed Mechanism | Evidence |
|---|---|
| Mechanical obstruction of the endolymphatic duct | Reduced duct size on imaging; induced by duct obstruction in animals |
| Autoimmune | Increased incidence of specific HLA types; response to steroids and desensitization in some patients |
| Viral infection | Delayed endolymphatic hydrops (profound deafness years before hydrops) suggests subclinical viral injury; no specific virus identified |
| Ischemia of endolymphatic sac | Links Meniere's with migraine (shared vascular mechanism); 56% lifetime migraine incidence in MD vs. 25% in controls |
| Multifactorial | Genetic predisposition + environmental triggers (trauma, AOM, labyrinthitis, congenital inner ear anomalies) |
The etiology is likely multifactorial, representing the final common pathway of multiple injuries. Meniere's disease may not be a single homogeneous entity.
- Cummings Otolaryngology, Etiology of Ménière Disease section, pp. 3208-3209
MRI Finding (Gadolinium-Enhanced)
Here is the MRI appearance showing endolymphatic sac enhancement:
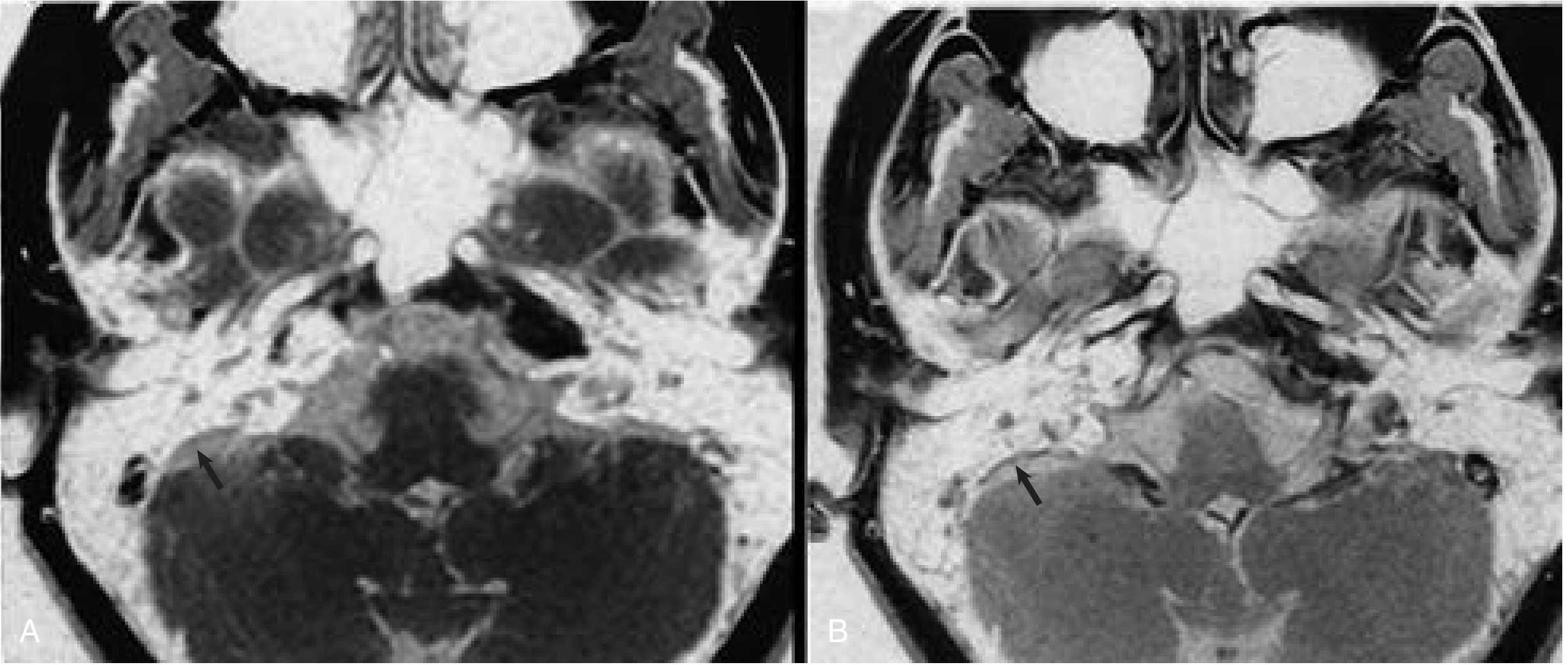
Fig: Axial T1 MRI of petrous bone in Meniere's disease. (A) Non-enhanced: endolymphatic sac (arrow) not enhancing. (B) Post-gadolinium: sac enhances (arrow). (Cummings, Fig. 167.4)
Diagnosis
Diagnostic Criteria (AAO-HNS):
- Two or more spontaneous episodes of vertigo, each lasting 20 min to 12 hours
- Audiometrically documented low-to-mid frequency SNHL in the affected ear on at least one occasion
- Fluctuating aural symptoms (hearing, tinnitus, or fullness) in the affected ear
- Not better accounted for by another vestibular diagnosis
Glycerol Test: Oral glycerol (1.2 mL/kg + equal volume saline) - hearing improvement within 1-3 hours suggests endolymphatic hydrops.
Audiometry: Fluctuating low-tone SNHL (early stages), electrocochleography (elevated SP/AP ratio > 0.4 suggests hydrops).
Variants:
- Cochlear hydrops: Fluctuating SNHL + tinnitus, no vertigo
- Vestibular hydrops: Episodic vertigo + aural fullness, no hearing loss
- Lermoyez syndrome: SNHL/tinnitus worsen pre-attack, then paradoxically improve when vertigo begins
- Tumarkin crisis (drop attack): Sudden fall without loss of consciousness; occurs in late disease
Management
Management is stepwise from conservative to destructive, guided by the severity of vertigo and status of residual hearing.
1. Lifestyle Modifications (First Line)
- Low-sodium diet (< 1500-2000 mg/day) - reduces endolymph production
- Avoidance of caffeine, alcohol, and smoking
- Stress reduction
- Adequate sleep, regular exercise
2. Medical Management
| Agent | Mechanism | Use |
|---|---|---|
| Diuretics (hydrochlorothiazide + triamterene, acetazolamide) | Reduce endolymph volume | First-line with low-Na diet; vertigo control, limited effect on hearing |
| Vestibular suppressants (meclizine, diazepam, promethazine) | Symptomatic relief during acute attacks | Acute attack management only |
| Betahistine (vasodilator) | Improves endolymph reabsorption, cochlear microcirculation | Widely used in Europe; evidence mixed |
| Steroids (systemic or IT) | Anti-inflammatory/immune modulation | Used in acute hearing drops or refractory vertigo |
No therapy to date has been proven to be effective for treatment of the hearing loss in Meniere's disease. - Cummings, p. 3034
3. Intratympanic (IT) Therapies
IT Dexamethasone:
- Less destructive; preserves hearing
- Itoh & Sakata (1987): 4-5 weekly injections of 2 mg dexamethasone - vertigo relief in 80%, tinnitus reduction in 74%
- Variable protocols exist; ablative surgery avoided in 81-91% of patients
- Preferred first when hearing preservation is priority
IT Gentamicin (chemical ablation):
- Selectively destroys vestibular hair cells (type I > type II)
- Highly effective for vertigo control (>90%)
- Risk of sensorineural hearing loss (titrated dosing minimizes this)
- Used in refractory cases with serviceable hearing or prior to surgical ablation
4. Surgical Management
Reserved for patients with disabling vertigo refractory to medical/IT therapy (~10% of patients).
Hearing-preserving procedures:
- Endolymphatic sac decompression/shunting (ELS): Decompresses the sac ± mastoid-sac or subarachnoid shunts; results comparable to placebo in blinded RCTs but still widely performed
- Selective vestibular neurectomy (retrolabyrinthine, middle cranial fossa, retrosigmoid): Cuts vestibular nerve while preserving cochlear branch; high vertigo control (~90%), hearing preservation in most
Hearing-destructive procedures (when hearing not useful):
- Labyrinthectomy (transmastoid): Destroys cochlea + vestibule; definitive vertigo control; use when no serviceable hearing
- Translabyrinthine 8th nerve section: Sacrifices all hearing; rarely used today
Cochleosacculotomy: Indicated in elderly patients with disabling vertigo, poor hearing, and residual vestibular function; can be done under local anesthesia.
- K.J. Lee's Essential Otolaryngology, p. 76-77
- Cummings Otolaryngology, pp. 3034-3035
Management Summary Flowchart
Diagnosis confirmed
↓
Lifestyle (low-Na, diuretics, vestibular suppressants for attacks)
↓ [Refractory vertigo]
IT Dexamethasone (hearing preservation priority)
↓ [Still refractory]
IT Gentamicin
↓ [Still refractory, useful hearing]
Endolymphatic sac surgery OR Vestibular neurectomy
↓ [No useful hearing]
Labyrinthectomy
Prognosis
- Spontaneous remission occurs in ~60% of patients
- Natural history is unpredictable - high inter-episode variability
- Bilateral involvement in up to 50% within 20 years
- Progressive hearing loss to moderate-severe level in most; profound loss is rare
Recent Evidence Update
Recent systematic reviews (2025-2026) are examining specific management areas:
- A 2026 network meta-analysis (PMID 41194325) comparing IT to surgical management in refractory Meniere's shows IT gentamicin and surgical approaches have comparable vertigo control; surgical options carry higher morbidity
- A 2025 systematic review on Tumarkin drop attacks (PMID 39428593) highlights that drop attacks remain difficult to manage and may require IT gentamicin or surgical ablation
- A 2026 systematic review on endolymphatic sac surgery (PMID 41673972) shows continued evolution of sac surgery techniques, though efficacy remains debated
What is otosclerosis
Reading File
Finding Sources
Reading File
Reading File
Reading File
Searching PubMed
"otosclerosis" AND management
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I have all the information needed. Here is the full, well-structured answer:
Otosclerosis
Definition
Otosclerosis is a disease of abnormal bone remodeling unique to the otic capsule, in which normal dense enchondral bone is replaced by irregular, vascular, spongy bone. The result is progressive fixation of the stapes, leading most commonly to conductive hearing loss. It is the most common cause of progressive conductive hearing loss (CHL) in adults.
- Cummings Otolaryngology Head and Neck Surgery (Ch. 146)
- Robbins, Cotran & Kumar Pathologic Basis of Disease
Epidemiology
| Feature | Detail |
|---|---|
| Prevalence (clinical) | 0.3 - 0.4% in Caucasians of European descent |
| Prevalence (histologic) | 10 - 12% (most cases subclinical) |
| Sex | Women 2:1 over men |
| Age of onset | Third decade (20s-30s) |
| Laterality | Bilateral in ~75%; usually asymmetric |
| Race | Predominantly White; rare in Africans, Asians, Native Americans |
| Family history | Positive in ~60% of clinical cases |
Etiology & Risk Factors
Otosclerosis is multifactorial - genetic + environmental:
- Genetics: Autosomal dominant with variable penetrance (25-40%). Multiple loci implicated (OTSC1-OTSC10, COL1A1 mutations). ~40-50% of cases are sporadic.
- Viral trigger (measles): Several studies link measles virus (paramyxovirus) persistence in the otic capsule to disease induction; measles RNA detected in otosclerotic foci. The decline of otosclerosis in measles-vaccinated populations supports this link.
- Hormonal factors: Pregnancy accelerates the disease. Many women first notice hearing loss during or just after their first pregnancy. Estrogen may promote osteoblast activity.
- Fluoride deficiency: Low fluoride in drinking water correlates with higher disease incidence (basis for sodium fluoride therapy).
- Autoimmune factors: Some evidence of anti-collagen type II antibodies.
Histopathology
The process has two phases:
Active Phase ("Otospongiosis")
- Osteoclasts resorb normal lamellar otic capsule bone
- Creates pseudovascular (haversian) spaces filled with marrow-like tissue
- Lesions have affinity for hematoxylin - appear darker than normal bone
- Osteoclasts are multinucleated and found at the advancing edge in finger-like projections
- Early lesions arise adjacent to the fissula ante fenestram (anterior to the oval window)
Inactive/Sclerotic Phase
- Osteoblasts deposit new, disorganized, denser bone
- Lesion enlarges, crosses the stapedial annular ligament
- Causes progressive stapedial fixation
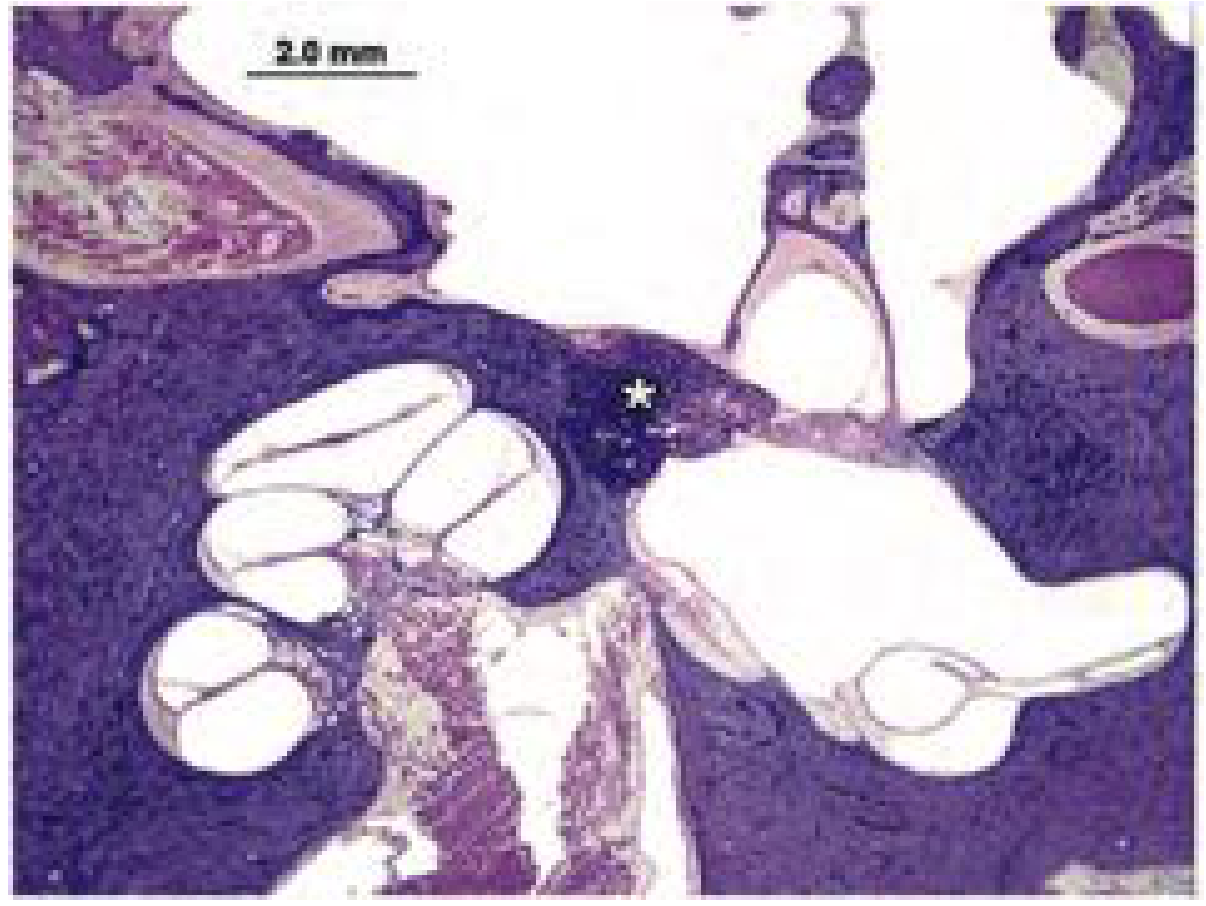
Fig. 146.1 - H&E section showing otosclerotic focus (asterisk) at fissula ante fenestram replacing stapes footplate bone. (Cummings)
Types of Footplate Fixation
- Anterior fixation (most common) - lesion at fissula ante fenestram
- Bipolar fixation - lesion at both anterior and posterior annular ligament
- "Biscuit footplate" (obliterative otosclerosis) - entire footplate replaced by thick, solid otosclerotic bone; annular ligament totally obliterated
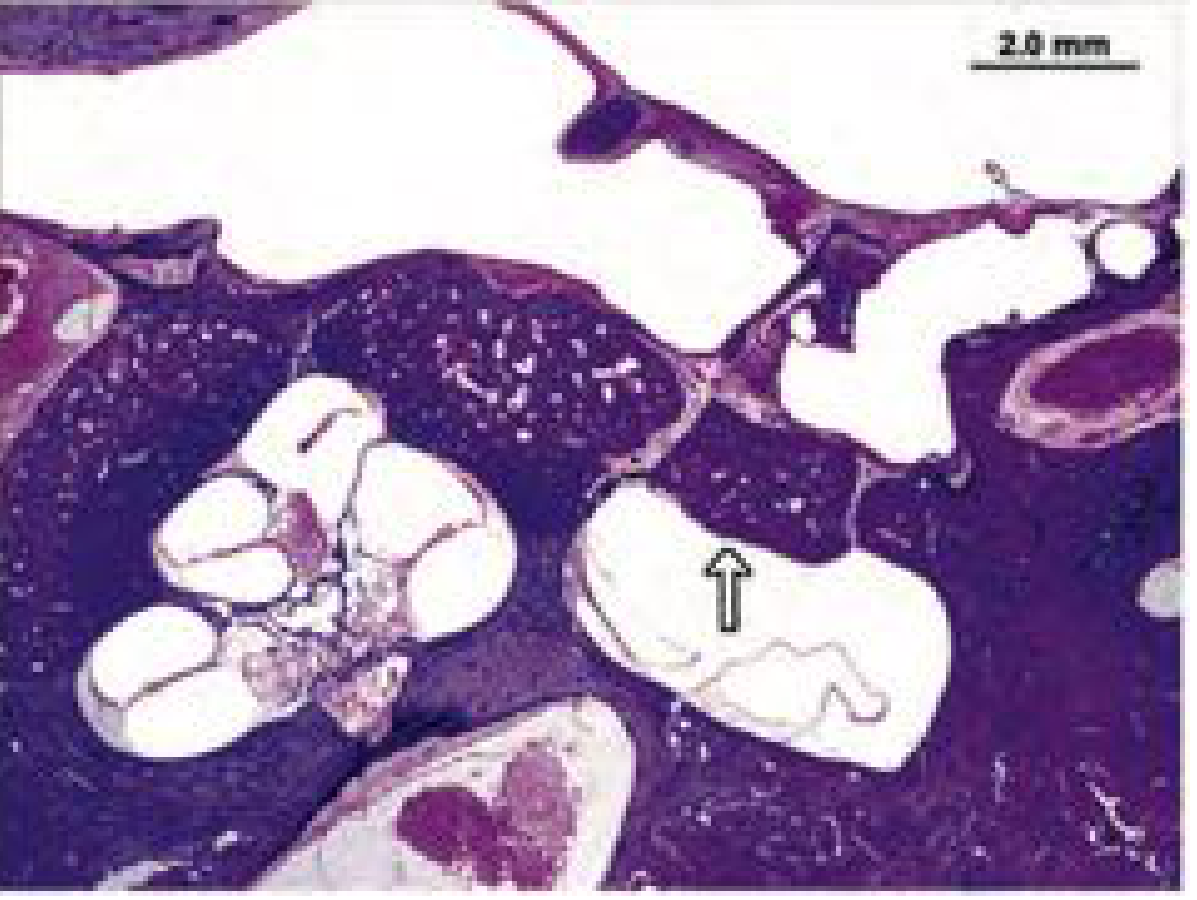
Fig. 146.3 - "Biscuit footplate" with total replacement of annular ligament (arrow). (Cummings)
Types / Locations
| Type | Location | Hearing Loss |
|---|---|---|
| Fenestral otosclerosis | Fissula ante fenestram → stapes footplate | Pure CHL |
| Cochlear (retrofenestral) otosclerosis | Endosteum of cochlea; spiral ligament | SNHL (collagen deposition + hyalinization of spiral ligament) |
| Mixed | Both fenestral + cochlear | Mixed CHL + SNHL |
Clinical Features
Symptoms
- Progressive, bilateral conductive hearing loss - typically insidious onset in 20s-30s
- Hearing is often better in noisy environments (paracusis Willisii - the ability to hear better in noisy surroundings because others raise their voice)
- Tinnitus - low-frequency
- No pain, no discharge (otoscopy is normal)
- Rarely, vertigo (if cochlear otosclerosis or coexisting Meniere's disease)
Signs
- Tympanic membrane: Normal
- Schwartze sign (flamingo pink blush): Reddish blush visible through tympanic membrane over the promontory, due to increased vascularity of active otosclerosis - indicates active disease and favorable prognosis
- Normal external canal
Tuning Fork Tests
| Test | Result |
|---|---|
| Rinne | Negative (BC > AC) in affected ear |
| Weber | Lateralizes to worse ear |
| Absolute Bone Conduction (ABC) | Normal (inner ear not affected in fenestral disease) |
Investigations
Pure Tone Audiometry (PTA)
- Low-to-mid frequency air-bone gap (conductive loss)
- Carhart's notch: A characteristic dip in bone conduction at 2000 Hz (mechanical - not true SNHL; it is a mechanical resonance effect of stapes fixation and reverses after stapedectomy)
- Cookie-bite or flat audiogram in advanced cases
Tympanometry
- Type As (shallow) - reduced compliance due to stapes fixation
- Stapedial reflexes absent (stapedius cannot move fixed stapes)
CT Temporal Bone (High-Resolution HRCT)
- Halo sign (double ring sign): Band of demineralization around cochlear capsule in cochlear otosclerosis
- Loss of definition of the oval window margin
- Narrowing or obliteration of the oval window niche
- Evaluates footplate thickness (important pre-operative planning)
Management
Management options: Observation, hearing aids, surgery (stapedotomy/stapedectomy), sodium fluoride (cochlear disease), or cochlear implant.
1. Hearing Aids
- Always a valid option, especially in elderly patients or those unfit for surgery
- Suitable when air-bone gap is the primary deficit
- Recommended trial before surgery is offered
2. Sodium Fluoride (Medical)
- Dose: 20 mg NaF + calcium/vitamin D daily for 2 years
- Mechanism: Fluoride promotes conversion of hydroxyapatite to fluoroapatite, stabilizing bone remodeling and reducing osteoclast activity
- Indication: Cochlear otosclerosis - to slow or halt SNHL progression
- No effect on established CHL; does not reverse stapes fixation
- Evidence is weak for arresting SNHL; Cummings notes limited definitive proof
3. Surgery - Stapedotomy (Preferred)
Stapedotomy (small fenestra procedure) has replaced stapedectomy as the procedure of choice, due to less inner ear trauma and equivalent hearing outcomes.
Stapedotomy Steps (Cummings, Box 146.1):
- Four-quadrant canal block with lidocaine + epinephrine
- Tympanomeatal flap elevated; enter middle ear
- Remove posterosuperior canal wall overhang (curette/microdrill)
- Palpate ossicular chain - confirm stapes fixation
- Measure incus-to-footplate distance (typically 4.5 mm)
- Laser rosette made in center of footplate
- Microdrill (0.7 mm diamond bur) creates fenestra in footplate
- Piston prosthesis placed into fenestra and onto incus
- Crimp prosthesis hook (or laser for nitinol prostheses)
- Down-fracture and remove stapes superstructure
- Tissue graft + blood around prosthesis to seal
Prosthesis types: Teflon piston, titanium clip, nitinol (shape-memory, MRI-compatible). Size based on incus-to-footplate distance.
Stapedectomy vs. Stapedotomy:
- Stapedotomy: Small fenestra (0.6-0.8 mm) in footplate; prosthesis piston through it
- Stapedectomy (total/partial): Removes footplate entirely; covered with tissue graft (vein, fat, perichondrium)
- Stapedotomy is preferred (last 35+ years); stapedectomy reserved for obliterative ("biscuit") footplates where a fenestra cannot be made
4. Cochlear Implantation
- Indicated in bilateral severe-profound mixed or SNHL where stapedotomy cannot restore adequate hearing
- Cochlear otosclerosis causing obliteration of the scala tympani makes implantation technically difficult
Complications of Stapes Surgery
| Complication | Rate / Comment |
|---|---|
| Profound SNHL (dead ear) | 0.2% - the most significant risk |
| Partial SNHL | 1-2% |
| Vertigo (transient) | Common post-op; usually resolves |
| Chorda tympani injury | Taste disturbance; ~10-30% transient |
| Perilymph gusher | Rare; associated with X-linked deafness (dilated IAC) |
| Tympanic membrane perforation | Rare |
| Prosthesis displacement | Late complication; revision surgery needed |
| Reparative granuloma | Sterile inflammatory reaction; early post-op severe SNHL |
Contraindications to Surgery
- Only hearing ear (relative)
- Active otitis media
- Uncontrolled Meniere's disease
- Perilymph gusher risk (X-linked stapes fixation, widened IAC on CT)
- Bone conduction >45 dB at 500 Hz with high-frequency loss (Cummings)
- Patient unwilling to accept hearing aid as alternative
Differential Diagnosis
- Tympanosclerosis - calcification of middle ear mucosa/ossicles
- Congenital stapes fixation - younger patients, no family history pattern
- Superior semicircular canal dehiscence (SSCD) - third window effect; must exclude
- Fixed malleus head - check full ossicular chain mobility
- Paget's disease of bone - also causes otic capsule remodeling
Recent Evidence
A 2026 umbrella review (PMID 41696966) on otosclerosis diagnosis and management confirms stapes surgery as the primary intervention for fenestral disease. A 2026 meta-analysis on anesthesia in stapes surgery (PMID 41165060) found local and general anesthesia have equivalent outcomes, with local anesthesia offering the advantage of real-time intraoperative hearing monitoring.
Sources: Cummings Otolaryngology Head and Neck Surgery (Ch. 146), Robbins Pathologic Basis of Disease, Scott-Brown's Otorhinolaryngology Vol 1 & 2, Shambaugh Surgery of the Ear, K.J. Lee's Essential Otolaryngology
Pathophysiology of csom
Finding Sources
Searching PubMed
"chronic suppurative otitis media" AND pathophysiology
Finding Sources
Searching PubMed
"chronic otitis media" AND biofilm AND pathogenesis
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have all the essential material. Let me compile the comprehensive answer.
Pathophysiology of Chronic Suppurative Otitis Media (CSOM)
Definition
CSOM is a persistent, chronic infection of the middle ear cleft (tympanic cavity + mastoid) characterized by:
- Tympanic membrane perforation (central or marginal)
- Recurrent or continuous purulent otorrhea for > 6 weeks (some definitions say > 2 weeks)
- Varying degrees of conductive hearing loss
It exists in two major forms:
- Tubotympanic (safe/benign) CSOM - central perforation, no cholesteatoma
- Atticoantral (unsafe/dangerous) CSOM - marginal/attic perforation, with cholesteatoma, bone erosion
Step 1 - Predisposing Factors (Setting the Stage)
Eustachian Tube (ET) Dysfunction - The Primary Driver
The entire pathophysiological cascade begins with ET dysfunction:
- The ET normally maintains middle ear pressure, drains secretions into the nasopharynx, and provides mucosal protection
- Dysfunction (obstruction, patulous ET, or impaired mucociliary clearance) causes negative middle ear pressure and impaired drainage
- Results from: adenoid hypertrophy, cleft palate, Down syndrome, craniofacial abnormalities, recurrent upper respiratory infections, poor socioeconomic conditions, and underdeveloped mastoid pneumatization
Mastoid Pneumatization
- Poorly pneumatized mastoid (common in CSOM patients) reduces the air reservoir, worsens negative middle ear pressure, and limits buffering capacity
- Reduced mastoid volume is an almost invariable finding in acquired CSOM with cholesteatoma
Step 2 - Acute to Chronic Transition
From AOM to CSOM
Recurrent AOM / OME
↓
Persistent middle ear effusion (serous → purulent)
↓
Mucosal edema + inflammatory mediator release
↓
TM perforation (acute AOM rupture or chronic retraction)
↓
Failure of TM to heal → Chronic perforation
↓
CSOM established
Spontaneous TM perforation during AOM usually heals. When it fails to heal - due to continued infection, poor healing factors (malnutrition, immunocompromise), or epithelial migration across the perforation edge - CSOM is established.
Step 3 - Mucosal Pathology in the Middle Ear
Once chronic infection is established, the normal flat, single-layered cuboidal middle ear mucosa undergoes profound changes:
Mucosal Metaplasia & Secretory Change
- Normal middle ear mucosa transforms under chronic inflammation into secretory (respiratory-type) mucosa with:
- Goblet cell hyperplasia
- Submucosal gland development
- Ciliated columnar epithelium (normally absent in tympanic cavity)
- This converted mucosa produces mucus, which perpetuates the effusion and creates a substrate for biofilm formation
Inflammatory Cell Infiltration
- Bacterial toxins and inflammatory mediators interact with edematous mucosa
- Basement membrane ruptures - inflammatory cells from the lamina propria enter the middle ear lumen
- Lamina propria extrudes through the disrupted basement membrane
Granulation Tissue Formation
-
Chemical mediators trigger:
- Angiogenic growth factors → neovascularization
- Epithelial growth factors (EGF) → epithelial proliferation
- Fibroblast recruitment → fibrous tissue formation
-
Combined result: granulation tissue polyps that fill the middle ear and mastoid
-
These polyps are friable, bleed easily, and produce enzymes that damage surrounding structures
-
Shambaugh Surgery of the Ear, p. 527
Step 4 - Tympanic Membrane Changes
Enzymatic Weakening
- Granulation tissue and chronic effusion contain proteolytic enzymes (collagenase, tPA - tissue plasminogen activator)
- These enzymes degrade the fibrous collagen skeleton of the TM (fibrous middle layer = lamina propria)
- TM loses tensile strength
Retraction Pocket Formation
- ET dysfunction creates chronic negative middle ear pressure
- Combined with enzymatic weakening, the pars flaccida (Shrapnell's membrane - no fibrous layer) and pars tensa retract medially
- Retraction pockets deepen over time
- Contact with underlying mucosa/granulation tissue → fibrous bands anchor the retracted membrane medially
- Eventually → perforation (central in tubotympanic; marginal/attic in atticoantral disease)
Perforation Perpetuation
- Once perforated, the squamous epithelium from the EAC migrates medially over the perforation edge
- This epithelial migration prevents healing and creates a pathway for ongoing contamination from the ear canal
Step 5 - Cholesteatoma Formation (Atticoantral CSOM)
Cholesteatoma = accumulation of desquamating keratinizing squamous epithelium in the middle ear cleft, capable of bone erosion and expansion.
Four Theories of Acquired Cholesteatoma Pathogenesis:
| Theory | Mechanism |
|---|---|
| 1. Invagination theory (most accepted) | Deep retraction pocket of pars flaccida or pars tensa becomes an epithelial-lined sac; desquamated keratin accumulates inside; negative middle ear pressure drives deepening |
| 2. Migration theory | Squamous epithelium migrates inward through a perforation along the path of least resistance; keratin accumulates in the middle ear |
| 3. Basal cell hyperplasia (proliferating) theory | Chronic inflammation stimulates basal cells in the EAC/TM junction to proliferate through the fibrous layer (Wendt's postulate) |
| 4. Metaplasia theory | Chronic irritation causes middle ear mucosa (cuboidal) to undergo squamous metaplasia, producing keratinizing epithelium |
Why Cholesteatoma Causes Bone Destruction
Once formed, cholesteatoma expands and erodes bone via:
- Osteoclast activation - the main mechanism
- IL-1, IL-6, TNF-α, EGF, PGE₂, PTH-rP, TGF-β, OPGL, and M-CSF from cholesteatoma keratinocytes and macrophages activate osteoclasts locally
- Matrix metalloproteinases (MMPs) and collagenase - directly degrade bone matrix
- tPA (tissue plasminogen activator) - enables local invasion
- Pressure necrosis - expansile mass effect compresses and ischemia-necroses surrounding bone
- Bacterial biofilm LPS - biofilms within chronically infected cholesteatomas elaborate lipopolysaccharide, which amplifies the osteoclast response and contributes to aggressiveness
"The main mechanism of bone resorption in chronic otitis media with and without cholesteatoma is thought to be the increased number and activity of osteoclasts. PGE₂, OPGL, and MCSF are some of the most potent osteoclast-activating metabolites. Cytokines and growth factors such as IL-1, IL-6, TNFα, EGF, PTH-rP, and TGFβ seem to play an important role in middle ear infections and cholesteatoma." - Cummings Otolaryngology, p. 2697
Step 6 - Microbiology & Biofilm Role
Organisms
- Pseudomonas aeruginosa - most common (especially in persistent/resistant CSOM)
- Staphylococcus aureus - including MRSA
- Proteus mirabilis
- Klebsiella pneumoniae
- Anaerobes (Bacteroides, Peptostreptococcus) - in atticoantral disease
- Fungi (Candida, Aspergillus) - especially after prolonged topical antibiotics
Biofilm Formation
- Bacteria in CSOM form biofilms - structured communities encased in an extracellular polysaccharide matrix adhered to mucosal surfaces
- Biofilm bacteria are 100-1000x more resistant to antibiotics than planktonic (free-floating) bacteria
- Explain chronic, treatment-refractory nature of CSOM
- Biofilms in cholesteatoma elaborate LPS which further activates osteoclasts
Step 7 - Ossicular Erosion & Hearing Loss
Ossicular Involvement (in order of frequency)
- Long process of incus - most commonly eroded (watershed zone, tenuous blood supply)
- Stapes suprastructure
- Malleus handle
Mechanism of Erosion
- Enzymatic (collagenase, MMPs) from granulation tissue/cholesteatoma
- Osteoclast-mediated bone resorption
- Pressure necrosis from expanding cholesteatoma mass
Hearing Loss
- Conductive (CHL) - from TM perforation + ossicular erosion (CHL > 30 dB suggests ossicular involvement)
- Sensorineural (SNHL) - from:
- Toxin/enzyme spread through the round window membrane to the inner ear
- Labyrinthitis (serious complication)
- Fistula of the lateral semicircular canal
- Note: SNHL of 5-33 dB is found in many CSOM patients and should be documented preoperatively
Summary: Pathophysiological Cascade
ET Dysfunction + Poor Mastoid Pneumatization
↓
Negative Middle Ear Pressure → Persistent Effusion
↓
Mucosal Edema → Bacterial Infection → Purulent Effusion
↓
Mucosal Metaplasia (secretory) → Granulation Tissue Formation
↓
Enzymatic Weakening of TM → Retraction Pockets → Perforation
↓
TUBOTYMPANIC CSOM ATTICOANTRAL CSOM
(Central perforation) (Marginal/attic perforation)
Granulation tissue ↓
Mucosal thickening CHOLESTEATOMA FORMATION
Ossicular erosion ↓
(enzymatic/granulation) Osteoclast activation
(IL-1, IL-6, TNF-α, PGE₂)
+ Biofilm amplification
↓
Bone erosion → Complications
Complications (by Extension of Pathophysiology)
| Complication | Mechanism |
|---|---|
| Mastoiditis | Extension of infection into mastoid air cells |
| Labyrinthine fistula | Cholesteatoma erodes lateral SCC (most common site) |
| Facial nerve palsy | Erosion of bony canal of facial nerve (vertical segment most common) |
| Petrous apicitis | Spread through petrous air cells |
| Meningitis / Brain abscess | Tegmen (roof) erosion or sigmoid sinus thrombophlebitis |
| Profound SNHL | Labyrinthitis from toxins, enzymes, or fistula |
| Carcinoma | Long-standing CSOM is found in ~68% of temporal bone SCC; HPV 16/18 implicated |
Sources: Shambaugh Surgery of the Ear (Etiology of CSOM), Cummings Otolaryngology Head and Neck Surgery (Ch. 131, 158), Scott-Brown's Otorhinolaryngology Vol 2, Cummings Ch. 146 (molecular mediators of bone resorption)
This is a shared conversation. Sign in to Orris to start your own chat.