what are the Indication, physiological effect and technique of insertion of intra aortic ballon pump for 10 marks Dnb anesthesia exam
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compose the complete DNB Anesthesia exam answer.
Intra-Aortic Balloon Pump (IABP) - DNB Anesthesia Exam Answer (10 Marks)
Introduction
The IABP, first described by Harken in 1958 and in clinical use since 1968, is the most commonly used mechanical circulatory support (MCS) device. It is a counterpulsation device - a double-lumen, 7.5 to 8.0 French catheter with a polyethylene balloon at its distal end, placed in the descending thoracic aorta just distal to the left subclavian artery, extending to the level of the renal arteries. It is inflated with helium (low viscosity allows rapid transfer; rapidly absorbed in blood if balloon ruptures).
I. INDICATIONS (3 marks)
A. Established / Class I Indications
| Category | Specific Indication |
|---|---|
| Cardiogenic Shock | Cardiogenic shock during/after AMI or cardiac surgery (most common use) |
| Mechanical complications of AMI | Acute mitral regurgitation due to papillary muscle rupture; acute ventricular septal defect (VSD) |
| Pre-operative stabilization | High-risk patients with severe CAD, LV dysfunction, or refractory unstable angina before cardiac surgery (CABG) |
| High-risk PCI | Prophylactic support during high-risk percutaneous coronary intervention |
| Post-cardiac surgery | Low cardiac output state after CABG; failure to wean from cardiopulmonary bypass |
| Bridge to definitive therapy | Bridge to heart transplantation or permanent VAD implantation |
| Refractory unstable angina | When medical therapy fails |
B. Contraindications
Absolute:
- Aortic regurgitation (balloon inflation in diastole worsens AR and increases LV end-diastolic pressure)
- Aortic dissection
Relative:
- Abdominal aortic aneurysm
- Severe peripheral arterial disease (especially at the proposed insertion site)
- Significant coagulopathy
- Uncontrolled sepsis
- Severe tachyarrhythmias (reduces diastolic filling time, impairing efficacy)
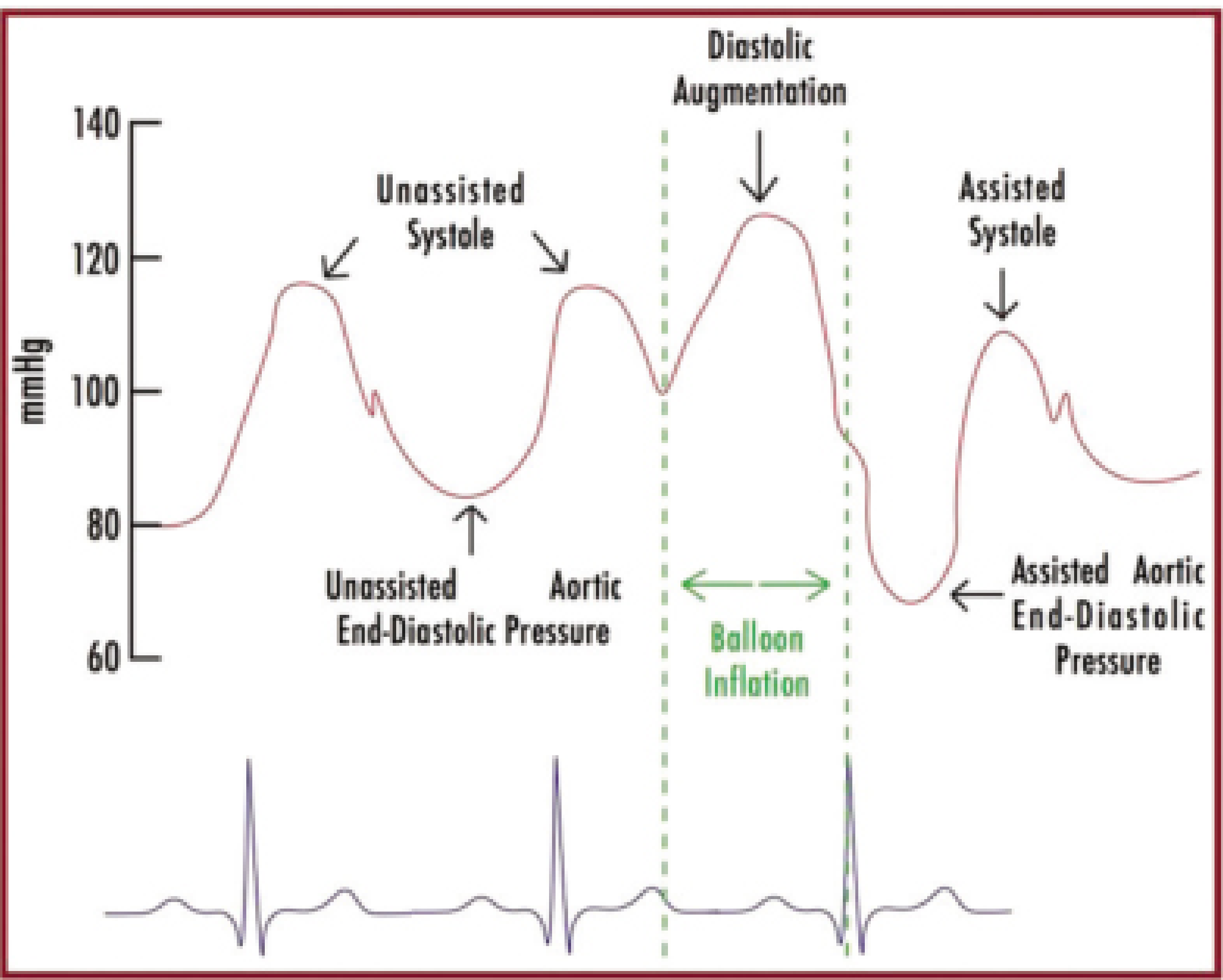
II. PHYSIOLOGICAL EFFECTS - Mechanism of Counterpulsation (4 marks)
The IABP works on the principle of diastolic augmentation and systolic unloading.
A. Balloon Inflation (During Diastole)
- Triggered at the dicrotic notch (aortic valve closure) - ECG trigger: middle of T-wave
- Balloon rapidly inflates, displacing blood proximally and distally
- Effect: Raises diastolic aortic pressure (diastolic augmentation)
- Increases coronary artery perfusion pressure (coronary arteries fill during diastole)
- Increases cerebral perfusion
- Increases peripheral organ blood flow
B. Balloon Deflation (Just Before Systole)
- Triggered at the R wave peak on ECG (onset of LV systole)
- Balloon rapidly deflates, creating a "vacuum" effect in the aorta
- Effect: Reduces aortic end-diastolic pressure
- Decreases LV afterload (the LV ejects against a lower resistance)
- Decreases LV wall stress
- Reduces myocardial oxygen consumption (MVO2)
C. Net Hemodynamic Effects (Summary Table)
| Parameter | Effect of IABP |
|---|---|
| Diastolic blood pressure | Increased (augmentation) |
| Systolic blood pressure | Decreased (afterload reduction) |
| Mean arterial pressure | Increased |
| Aortic end-diastolic pressure | Decreased |
| LV afterload | Decreased |
| Cardiac output / Cardiac index | Modestly increased (~10-20%) |
| Myocardial oxygen consumption | Decreased |
| Coronary perfusion pressure | Increased |
| LV preload (LVEDP/PCWP) | Decreased |
| Heart rate | Minimal direct effect |
Important: The IABP does NOT generate cardiac output independently - it requires the heart to have some residual LV function. Any increase in cardiac output depends on the work of the heart itself.
D. Optimal Effect Depends On:
- Correct balloon position in the aorta
- Blood displacement volume (balloon size matched to patient's aortic diameter)
- Balloon diameter relative to aortic diameter (ideally 85-95% of aortic diameter)
- Correct timing of inflation/deflation
- Patient's heart rate, blood pressure, and vascular resistance
III. TECHNIQUE OF INSERTION (3 marks)
A. Equipment
- Double-lumen, 7.5-8.0 Fr catheter with polyethylene balloon
- Balloon size chosen based on patient height (typically 25-50 mL volume)
- Helium gas for inflation
- Pump console (ECG or pressure-triggered)
- Fluoroscopy or bedside X-ray / ultrasound guidance
B. Standard Percutaneous Seldinger Technique (Femoral Approach - most common)
Step 1 - Patient preparation:
- Patient supine. Access is usually the left femoral artery (can also use right femoral)
- Sterile prep and drape
- Local anesthesia (or GA/sedation if already in theatre)
Step 2 - Arterial access:
- Palpate femoral artery at the femoral crease
- Puncture the common femoral artery (above the femoral bifurcation) with a needle at 30-45° angle
- Confirm arterial blood flashback
Step 3 - Guidewire placement (Seldinger technique):
- Insert a 0.035-inch J-tip guidewire through the needle into the aorta
- Remove the needle; make a small skin incision at the wire entry point
Step 4 - Sheath insertion:
- Pass an introducer sheath (8-9 Fr) over the guidewire using serial dilation
- Remove dilator, leave sheath in situ
Step 5 - Balloon catheter placement:
- Pre-fold/wrap the balloon catheter
- Advance the balloon catheter over the guidewire through the sheath
- Position the tip of the catheter 2-3 cm distal to the left subclavian artery (around the carina level on X-ray, or 2nd-3rd intercostal space)
- Confirm position with fluoroscopy or chest X-ray (tip at level of carina / aortic knuckle)
- Note: Too high → risk of subclavian/carotid occlusion; Too low → risk of renal/mesenteric artery occlusion
Step 6 - Connecting to console and timing:
- Connect catheter to the pump console
- Select trigger mode: ECG trigger (R-wave) preferred in sinus rhythm; pressure trigger if ECG unreliable; internal trigger if in asystole/pacing
- Set inflation timing: balloon inflates at dicrotic notch of arterial trace (ECG: middle of T-wave)
- Set deflation timing: balloon deflates just before the R wave (peak of QRS)
- Start at 1:2 ratio (assists every other beat) to check timing and waveform; increase to 1:1 (augments every beat)
Step 7 - Confirmation of correct timing (from arterial waveform):
- Correct: Diastolic augmentation peak > unassisted systolic peak; assisted aortic end-diastolic pressure lower than unassisted end-diastolic pressure; assisted systolic pressure lower than unassisted
- Early inflation: Augmentation peak merges with systolic upstroke (increases afterload - dangerous)
- Late inflation: Diastolic augmentation begins after dicrotic notch; reduced coronary perfusion benefit
- Early deflation: "V" shape notch before diastole ends; no afterload reduction
- Late deflation: Assisted end-diastolic pressure = unassisted (no afterload reduction)
Step 8 - Heparinization:
- Systemic anticoagulation with heparin (ACT 150-180 sec) to prevent thrombosis and limb ischemia
C. Alternative Access Sites
- Axillary / subclavian artery (surgical cut-down) - when bilateral femoral access not possible
- Ascending aorta (intra-operative surgical placement)
- Brachial artery (rarely)
IV. COMPLICATIONS
| Complication | Rate |
|---|---|
| Limb ischemia (most common major complication) | ~1-2% major |
| Bleeding / hematoma at insertion site | Common |
| Balloon rupture (helium embolism) | Rare |
| Aortic dissection | Rare |
| Thrombocytopenia (mechanical destruction) | 5-10% |
| Infection | <1% |
| Stroke / cerebral embolism | Rare |
| Renal / mesenteric ischemia (if too low) | Position-related |
| Overall major complications | ~2.6% (Benchmark Registry) |
V. WEANING
- Gradually reduce ratio from 1:1 → 1:2 → 1:3 as hemodynamics improve
- Generally used for a few days; wean as cardiac function recovers
- Remove sheath with direct pressure/compression of femoral artery for 30 minutes post-removal
Sources: Braunwald's Heart Disease 12e; Fischer's Mastery of Surgery 8e; Sabiston Textbook of Surgery; Schwartz's Principles of Surgery 11e; Mulholland & Greenfield's Surgery 7e; Tintinalli's Emergency Medicine
principle of ultrasound and uses in anesthesia for 10 marks dnb exam
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.