Pain behind and deep under Achilles tendon . Give me possible structures that may be involved from physiotherapy perspective
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
structures involved posterior deep Achilles tendon pain physiotherapy anatomy retrocalcaneal
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Excellent - I now have very rich, authoritative content. Let me compile the comprehensive answer.
Structures Involved in Pain Behind and Deep Under the Achilles Tendon - A Physiotherapy Perspective
Pain specifically described as behind and deep under the Achilles tendon localises to the posterior heel/retromalleolar region, which contains several distinct structures that physiotherapists must differentiate. This region is best understood through the concept of the Achilles Enthesis Organ - a collective of anatomically interrelated structures that all work together to reduce stress concentration at the calcaneal insertion.
The Achilles Enthesis Organ (The Master Concept)
The Achilles enthesis organ, as described in Rheumatology (Elsevier, 2022), comprises:
"The enthesis itself, the sesamoid and periosteal fibrocartilage, the bursa, and the fat pad collectively comprise the Achilles enthesis organ... Together, they all function in one way or another to reduce stress concentration at the enthesis itself."
Understanding this organ concept explains why these structures are so frequently co-affected. Here is a detailed breakdown:
1. Retrocalcaneal Bursa (Primary Suspect for Deep Pain)
This is the most clinically important structure for pain that is deep to and anterior to the Achilles tendon.
- Location: Between the anteroinferior wall of the Achilles tendon and the posterosuperior surface of the calcaneus - exactly "deep under" the tendon
- Structure: A saddle-shaped, synovial-lined space. Its anterior margin is fibrocartilage, posterior margin is the paratenon of the Achilles tendon, and the superior margin is adipose tissue
- Function: Reduces friction associated with tendon movement. During dorsiflexion, the Achilles tendon is compressed against the calcaneal tuberosity; the bursa allows smooth gliding
- Clinical features when inflamed: Deep posterior heel pain, fullness/swelling palpable medially and laterally to the tendon, pain worsened by ankle dorsiflexion (classic finding), morning stiffness on first rising
- Associations: Often co-occurs with Haglund deformity; linked to RA, seronegative spondyloarthropathies (ankylosing spondylitis, psoriatic arthritis), gout, as well as mechanical overuse in runners
(Campbell's Operative Orthopaedics 15th Ed 2026; Miller's Review of Orthopaedics 9th Ed; Rheumatology, Elsevier 2022)
2. Insertional Achilles Tendon (Deep Surface and Insertional Footprint)
The Achilles inserts broadly into the posterior calcaneal tuberosity over the lower half of the posterior calcaneal surface. The deep/anterior surface of the tendon at the insertion is the portion under compressive load.
- Insertional tendinopathy involves degeneration of tendon fibres at or within 2 cm of the calcaneal insertion
- Intratendinous calcification commonly develops with chronicity, creating focal compressive pain deep within the tendon
- The sesamoid fibrocartilage on the deep surface of the Achilles (adjacent to the retrocalcaneal bursa) and the periosteal fibrocartilage on the posterosuperior calcaneus are compressed against each other during dorsiflexion - the mechanical basis of deep insertional pain
- Key clinical distinction: Insertional tendinopathy pain is reproduced on the tendon itself at the heel bone, often with visible/palpable thickening; pain worsens with dorsiflexion and in closed-back shoes
(Campbell's Operative Orthopaedics 15th Ed 2026; Rheumatology, Elsevier 2022)
3. Kager's Fat Pad (Pre-Achilles Fat Pad)
This is often overlooked but clinically relevant from a physiotherapy standpoint.
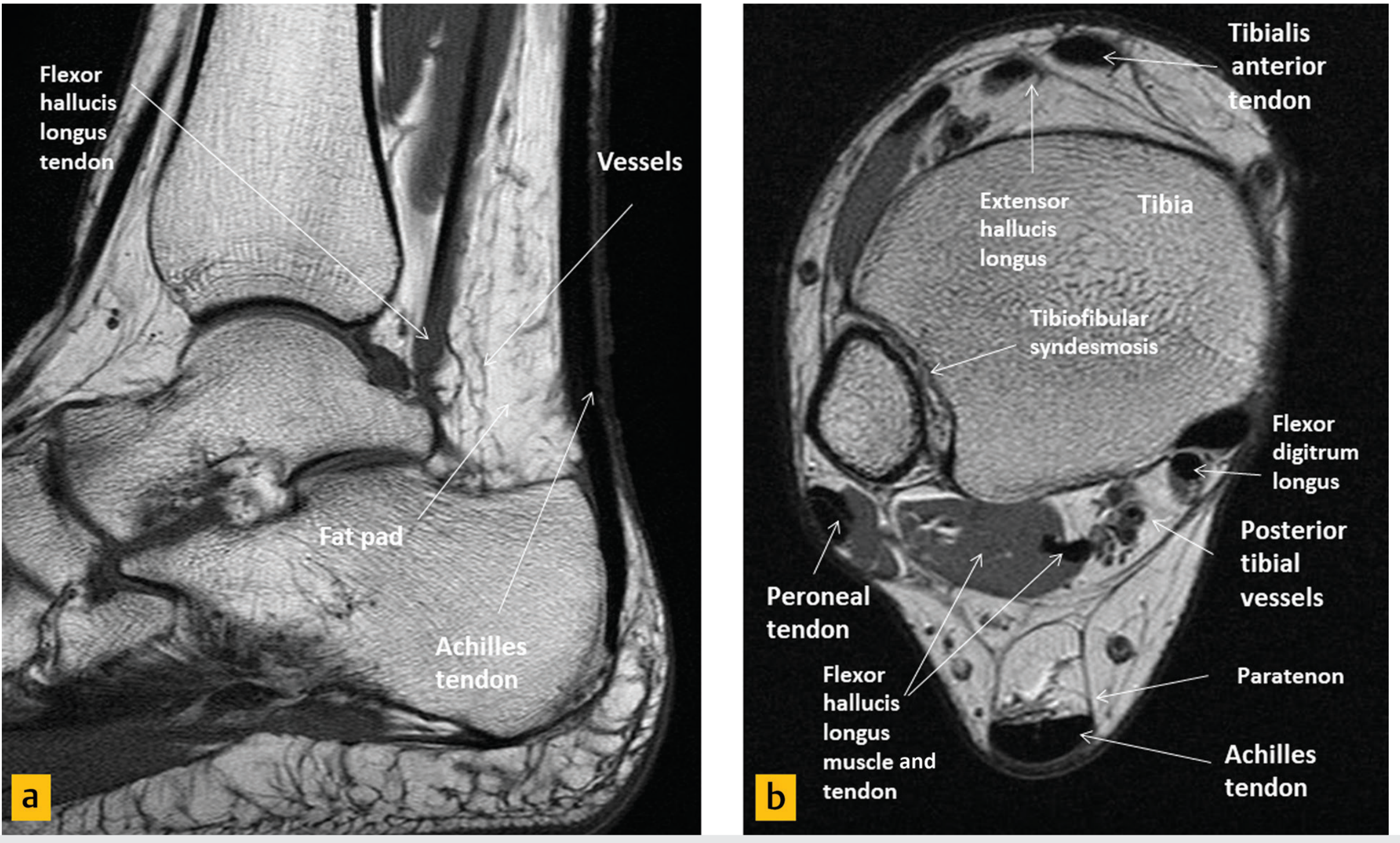
MRI of the hindfoot showing Kager's fat pad (triangular, anterior to Achilles tendon), alongside the FHL tendon - Imaging Anatomy Atlas Vol.3
- Location: A triangular space bounded by:
- Posterior: Achilles tendon
- Anterior: Flexor hallucis longus muscle and tendon
- Inferior: Superior cortex of the calcaneus
- Function: Highly vascular and sensory nerve-innervated (contains mechanoreceptors). During movement, the tip of Kager's fat pad slides in and out of the retrocalcaneal bursa to minimise pressure changes and promote boundary lubrication
- Pathology: In Achilles tendinopathy, oedema and fibrosis of Kager's fat pad is a recognised finding on MRI/ultrasound. This causes pain because it is richly innervated. Fat pad impingement can occur independently of tendon pathology
- Clinical note: A hardened or fibrotic Kager's fat pad may impair normal tendon gliding, perpetuating pain cycles even after the primary tendinopathy improves
(Imaging Anatomy Text and Atlas Vol.3; Rheumatology, Elsevier 2022)
4. Haglund Deformity (Posterosuperior Calcaneal Prominence)
While this is a bony structure, it is a key driver of soft tissue pain in this region.
- A prominent exostosis off the posterosuperior calcaneal tuberosity, located anterior to the Achilles tendon
- During dorsiflexion, the bony prominence repetitively abrades the deep surface of the Achilles tendon and compresses the retrocalcaneal bursa
- This leads to the classic triad: Haglund deformity + retrocalcaneal bursitis + insertional Achilles tendinopathy - often co-existing
- Physiotherapy relevance: Heel lifts reduce dorsiflexion range, taking mechanical stress off the tendon-bursa-bone interface; footwear modification (open-backed shoes) reduces compression
(Campbell's Operative Orthopaedics 15th Ed 2026; Miller's Review of Orthopaedics 9th Ed)
5. Calcaneal Bone / Insertional Footprint (Subtendinous Calcaneus)
- The posterosuperior calcaneal tuberosity where the Achilles inserts can develop:
- Calcaneal enthesophytes (insertional spurs) - bony outgrowths within the tendon at the insertion
- Bone marrow oedema (stress reaction) at the calcaneal tuberosity - visible on MRI as a signal change
- Calcaneal stress reactions cause deep, diffuse aching pain precisely "under" the tendon
- May be a primary source of pain independent of the overlying tendon
(General Anatomy and Musculoskeletal System, Thieme Atlas)
6. Flexor Hallucis Longus (FHL) Tendon
Sitting immediately anterior to Kager's fat pad in the posteromedial ankle:
- FHL runs in a groove under the talus (posterior talar process/os trigonum) and can develop tenosynovitis or stenosis
- Pain is often deep, posteromedial, and can mimic or co-exist with retrocalcaneal pathology
- Key differentiator: FHL pain is most prominent with toe/great toe motion, particularly in athletes (dancers, runners); a "trigger toe" phenomenon may be present
- Associated with posterior ankle impingement and os trigonum syndrome
(Rheumatology, Elsevier 2022 - Differential Diagnosis Table for Posterior Ankle Pain)
7. Superficial (Retro-Achilles / Pre-tendinous) Bursa
This is distinct from the retrocalcaneal bursa and sits posterior to (not deep under) the tendon, between the skin and the posterior Achilles tendon.
- An adventitious bursa - not always present anatomically
- Especially prone to friction from shoe heel counters
- Pain when wearing shoes is a hallmark; less painful on first arising than retrocalcaneal bursitis
- Relevant when differentiating purely deep pain (retrocalcaneal) from superficial posterior pain (retro-Achilles)
(Roberts and Hedges' Clinical Procedures in Emergency; Rheumatology, Elsevier 2022)
8. Os Trigonum / Posterior Talar Impingement
- The os trigonum is an accessory ossicle at the posterior lateral tubercle of the talus, present in ~5-14% of the population
- During forced plantarflexion, it becomes pinched between the tibia and calcaneus, causing posterior ankle impingement syndrome
- Pain is deep, posterior, and reproduced on full plantarflexion (contrast with retrocalcaneal bursitis which worsens on dorsiflexion)
- Often confused with Achilles pathology but requires very different physiotherapy management
(Rheumatology, Elsevier 2022 - Differential Diagnosis Table)
Summary Table - Key Differentiating Features
| Structure | Exact Location | Pain Provocation | Key Clinical Clue |
|---|---|---|---|
| Retrocalcaneal bursa | Deep to Achilles, anterior to tendon insertion | Dorsiflexion, palpation medial/lateral to tendon | Morning stiffness, consider systemic arthritis |
| Insertional Achilles tendon | At calcaneal footprint, deep surface | Dorsiflexion, direct palpation at bone | Calcification on X-ray, thickening |
| Kager's fat pad | Triangular space anterior to tendon | Tendon movement, compression | MRI oedema, often overlooked |
| Haglund deformity | Posterosuperior calcaneal tuberosity | Dorsiflexion, closed-back shoes | Visible bony lump, positive radiograph |
| Calcaneal enthesophyte/BMO | Within/at Achilles insertion on calcaneus | Loading, palpation | MRI confirms, X-ray spur |
| FHL tendon | Posteromedial, deep to fat pad | Great toe flexion, passive toe extension | Tendon pathology in runners/dancers |
| Retro-Achilles bursa | Posterior to tendon (superficial) | Shoe counter pressure | Pain only in shoes |
| Os trigonum | Posterior talus | Forced plantarflexion | Pain on plantarflexion, not dorsiflexion |
Physiotherapy Clinical Pearl
Campbell's Operative Orthopaedics makes a key point worth embedding in your assessment:
"In prolonged or severe cases, all aspects of insertional tendinopathy (retrocalcaneal bursitis, Achilles tendinopathy, and pretendinous bursitis) can exist concomitantly."
This means careful palpation - medial and lateral to the tendon for bursa, directly on the insertion for tendinopathy, and superficial for pretendinous bursa - is essential to identify the dominant pain generator before planning rehabilitation.
Sources: Campbell's Operative Orthopaedics 15th Ed 2026 | Rheumatology 2-Volume Set, Elsevier 2022 | Imaging Anatomy Text and Atlas Vol.3 | Miller's Review of Orthopaedics 9th Ed | General Anatomy and Musculoskeletal System, Thieme Atlas
This is a shared conversation. Sign in to Orris to start your own chat.