hepatocellular insufficiency syndrome i want full information give this topics for every type Etiology ,pathology, diagnostic,mechanism, medication,normal physiology,, physical examination, therapy,related syndromes, complications
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Here is a comprehensive, structured reference on Hepatocellular Insufficiency Syndrome — covering all three major clinical types: Acute Liver Failure (ALF), Chronic Liver Failure (CLF) / Cirrhosis, and Acute-on-Chronic Liver Failure (ACLF).
Hepatocellular Insufficiency Syndrome
A Comprehensive Clinical Reference
Note: "Hepatocellular insufficiency syndrome" is the collective term describing the clinical state in which the liver's functional reserve falls below the threshold necessary to maintain homeostasis. 80–90% of functional hepatic capacity must be lost before frank failure appears.
🔬 Normal Liver Physiology (Baseline)
Before understanding failure, one must understand normal hepatic function:
| Function | Detail |
|---|---|
| Protein synthesis | Albumin, clotting factors (I, II, V, VII, IX, X), binding proteins |
| Metabolic detoxification | Ammonia → urea (urea cycle); drug metabolism (CYP450) |
| Bilirubin metabolism | Conjugation and biliary excretion |
| Glucose homeostasis | Gluconeogenesis, glycogen storage |
| Immune function | Kupffer cells, acute-phase reactant synthesis |
| Lipid metabolism | Lipoprotein synthesis, fatty acid oxidation |
| Bile production | Emulsification of fats, excretion of waste products |
In acute liver failure, the liver's inability to metabolize ammonia via the urea cycle is central — ammonia from the GI tract (produced by microorganisms and enterocytes during glutamine metabolism) transits the portal vein but is no longer cleared, entering systemic circulation and causing cerebral toxicity. — Robbins, Cotran & Kumar Pathologic Basis of Disease
─────────────────────────────────────
TYPE 1: ACUTE LIVER FAILURE (ALF)
─────────────────────────────────────
📌 Definition
Acute liver illness producing encephalopathy + coagulopathy (INR > 1.5) within 26 weeks of initial injury, in the absence of pre-existing liver disease. Most cases manifest within 8 weeks; many progress to coma within 1 week. — Robbins, Cotran & Kumar
🧪 Etiology
| Cause | Frequency / Notes |
|---|---|
| Acetaminophen toxicity | ~50% of adult US cases; causes massive zone 3 necrosis within 1 week |
| Idiosyncratic drug-induced liver injury (DILI) | Wide range of agents (NSAIDs, antibiotics, anticonvulsants) |
| Autoimmune hepatitis | May present as fulminant ALF |
| Acute hepatitis B | Predominant cause in Asia and Mediterranean |
| Acute hepatitis E | Particularly dangerous in pregnant women (up to 20% mortality) |
| Hepatitis A | Most common cause worldwide overall |
| Herpes simplex / CMV / adenovirus | In immunocompromised hosts |
| Wilson disease | Metabolic cause; can present as acute copper release |
| Shock liver / ischemic hepatitis | Hypoperfusion → zone 3 centrilobular necrosis |
| Acute fatty liver of pregnancy | Mitochondrial dysfunction → microvesicular steatosis |
| Malignant infiltration | Leukemia/lymphoma (33%), metastatic breast cancer (30%), colon cancer (7%) |
| Indeterminate | ~15% adult cases; ~50% pediatric cases |
— Robbins, Cotran & Kumar Pathologic Basis of Disease; Goldman-Cecil Medicine
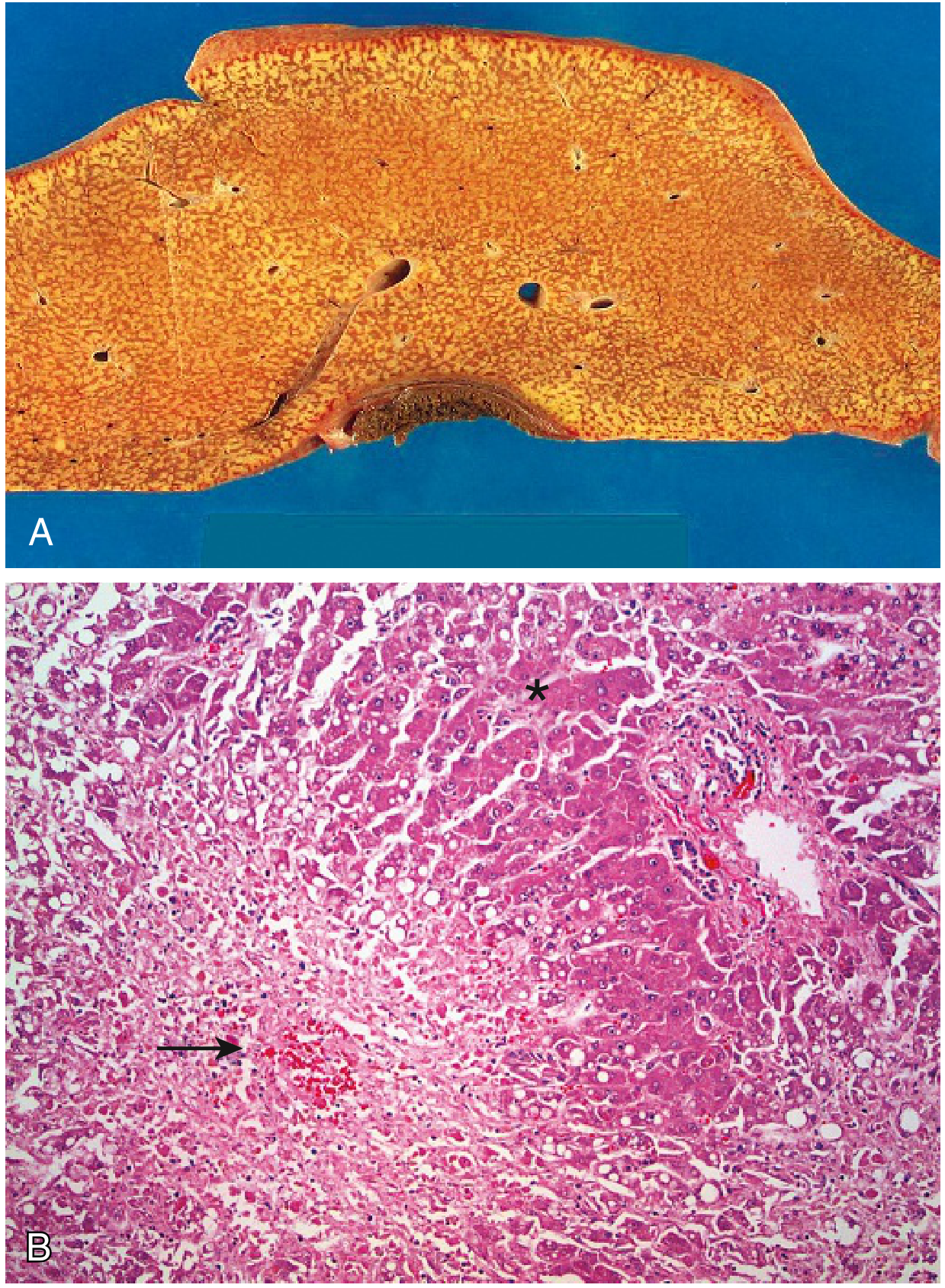
🧫 Pathology / Morphology
- Macroscopic: Liver is small, shrunken, bile-stained, soft, and congested (due to massive parenchymal loss).
- Microscopic: Broad zones of hepatocellular necrosis surrounding residual islands of hepatocytes or regenerating cells. Scarring is absent in rapid toxic injuries (insufficient time). Acetaminophen characteristically causes perivenular (zone 3) confluent necrosis with little inflammation.
- In AFLP and valproate toxicity: microvesicular steatosis without overt necrosis — mitochondrial dysfunction impairs metabolism without cell death.
- Non-hepatotropic viral infections: panlobular necrosis in immunocompromised patients.
⚙️ Mechanism / Pathophysiology
- Hepatocyte necrosis → massive cytokine release (TNF-α, IL-1, IL-6) → systemic inflammatory response, tissue hypoxia, lactic acidosis.
- Synthetic failure: Loss of clotting factors (especially Factor V — shortest half-life, most sensitive biomarker) → coagulopathy.
- Ammonia accumulation: Failure of urea cycle → hyperammonemia → crosses blood-brain barrier → astrocyte swelling → cerebral edema + hepatic encephalopathy.
- Hypoglycemia: Loss of gluconeogenesis and glycogen stores.
- Immune paralysis: Increased susceptibility to bacterial/fungal infections.
- Renal vasoconstriction: Cytokine-mediated + hypotension → hepatorenal syndrome.
- Vascular collapse: Vasodilation from inflammatory mediators → circulatory failure.
The encephalopathy of ALF is primarily driven by cerebral edema — distinct from chronic liver failure, where portosystemic shunting dominates. — Goldman-Cecil Medicine
🩺 Physical Examination
| Finding | Significance |
|---|---|
| Jaundice / icterus | Bilirubin retention; scleral yellowing |
| Hepatomegaly (early) | Edema and inflammation |
| Shrinking liver (late) | Parenchymal destruction — palpable loss of dullness |
| Asterixis ("liver flap") | Non-rhythmic extension-flexion of dorsiflexed wrists; indicates encephalopathy |
| Fetor hepaticus | Sweet, musty breath from mercaptan accumulation |
| Altered consciousness | Graded 1–4 (Grade 1: subtle; Grade 4: coma) |
| Bleeding | Ecchymoses, petechiae, oozing from venipuncture sites |
| Ascites | Portal hypertension / low oncotic pressure |
| Hypotension | Vasodilatory shock |
| Fever | Systemic inflammation or superimposed infection |
🔬 Diagnostic Evaluation
| Test | Findings |
|---|---|
| Serum transaminases (AST/ALT) | Markedly elevated (thousands); fall as hepatocytes are destroyed |
| INR / PT | Prolonged — most important coagulopathy marker |
| Factor V level | Most sensitive (shortest half-life); guides prognosis |
| Serum bilirubin | Elevated (both direct and indirect) |
| Serum albumin | Low (synthetic failure) |
| Serum ammonia (arterial) | Elevated; correlates with encephalopathy grade and cerebral edema risk |
| Blood glucose | Hypoglycemia common |
| Serum lactate / pH | Lactic acidosis; key prognostic marker in acetaminophen ALF (King's College Criteria) |
| Creatinine / BUN | Hepatorenal syndrome assessment |
| Viral serology | Anti-HAV IgM, HBsAg, Anti-HBc IgM, HCV RNA, HEV IgM |
| Autoimmune panel | ANA, ASMA, anti-LKM-1 (autoimmune hepatitis) |
| Ceruloplasmin / serum copper | Wilson disease |
| Toxicology screen | Acetaminophen level, drug screen |
| CBC, cultures | Leukocytosis; sepsis workup |
| CT head / ICP monitoring | Cerebral edema in Grade III–IV encephalopathy |
| Liver biopsy | Occasionally used; transjugular route preferred due to coagulopathy |
💊 Medication & Therapy
Specific antidotes / etiology-targeted:
| Cause | Treatment |
|---|---|
| Acetaminophen | N-acetylcysteine (NAC) — 140 mg/kg loading dose, then 70 mg/kg q4h × 17 doses |
| Hepatitis B | Nucleoside/nucleotide analogues (entecavir, tenofovir) |
| Herpes simplex | Acyclovir IV |
| Wilson disease | Copper chelation (D-penicillamine, trientine) |
| Autoimmune hepatitis | High-dose corticosteroids |
| Idiosyncratic DILI | Withdrawal of offending drug; NAC may be beneficial |
| AFLP | Immediate delivery of fetus |
| Budd-Chiari | Anticoagulation, TIPS, or surgical decompression |
Supportive ICU management:
| Issue | Intervention |
|---|---|
| Encephalopathy | Minimize sedatives; lactulose (limited evidence in ALF); avoid nephrotoxins |
| Cerebral edema (Grade III–IV) | Prophylactic hypertonic saline (Na⁺ target 145–155 mEq/L); mannitol 0.5–1 g/kg for confirmed ICP elevation |
| Hypotension | Judicious IV normal saline; norepinephrine first-line vasopressor; add vasopressin for escalating doses |
| Adrenal insufficiency | Trial of hydrocortisone in persistent hypotension |
| Coagulopathy / bleeding | FFP, vitamin K, cryoprecipitate; avoid prophylactic correction unless active bleeding or procedure planned |
| Hypoglycemia | Continuous dextrose infusion |
| Infections | Broad-spectrum antibiotics empirically; antifungals if at risk |
| Renal failure | Continuous renal replacement therapy (CRRT) preferred |
| Nutrition | Enteral feeding; target nitrogen balance; restrict protein only if severe encephalopathy |
| Respiratory failure | Intubation; bilevel positive airway pressure (BiPAP) generally avoided (aspiration risk) |
| Liver support | MARS (Molecular Adsorbent Recirculating System) — temporary bridge; no confirmed mortality benefit alone |
Definitive Treatment: Liver Transplantation
- Only curative therapy for irreversible ALF
- King's College Criteria guide listing urgency
- Must be referred to transplant center early
- Without transplant: mortality ~80%
— Goldman-Cecil Medicine; Tintinalli's Emergency Medicine; Robbins, Cotran & Kumar
─────────────────────────────────────
TYPE 2: CHRONIC LIVER FAILURE (CLF) / CIRRHOSIS
─────────────────────────────────────
📌 Definition
End-stage liver disease resulting from years of progressive injury and fibrosis, leading to cirrhosis — diffuse parenchymal nodules surrounded by fibrous bands with portosystemic shunting. CLF and cirrhosis, while frequently associated, are not synonymous.
🧪 Etiology
| Cause | Notes |
|---|---|
| Chronic hepatitis B (HBV) | Most common worldwide; integrates into host DNA |
| Chronic hepatitis C (HCV) | Most common indication for liver transplant (now declining with DAAs) |
| Alcohol-associated liver disease (ALD) | Now #1 indication for transplant in US (post-HCV treatment era); steatosis → steatohepatitis → cirrhosis |
| Metabolic dysfunction-associated steatotic liver disease (MASLD/NAFLD) | Strongly linked to obesity, insulin resistance, metabolic syndrome; rapidly growing indication for transplant |
| Primary biliary cholangitis (PBC) | Autoimmune bile duct destruction |
| Primary sclerosing cholangitis (PSC) | Stricturing bile duct fibrosis; associated with IBD |
| Autoimmune hepatitis | If untreated |
| Hemochromatosis | Iron overload |
| Wilson disease | Copper accumulation |
| Alpha-1 antitrypsin deficiency | Polymer accumulation in hepatocytes |
| Cryptogenic cirrhosis | No clear etiology identified |
🧫 Pathology / Morphology
- Macroscopic: Bumpy, nodular liver surface with depressed scarring zones and bulging regenerative nodules. Liver may initially be enlarged (fatty change) then shrink.
- Microscopic: Parenchymal nodules surrounded by dense collagen bands — visualized with Masson's trichrome or Sirius red stains. Fibrous bands may link portal-to-portal tracts (biliary pattern) or portal-to-central veins (post-necrotic/viral pattern).
- Vascular shunting: portosystemic anastomoses form — basis of portal hypertension complications.
- Morphologic regression (if injury ceases): thin, incomplete scars with ductular reactions.

⚙️ Mechanism / Pathophysiology
- Repeated hepatocyte injury → activation of hepatic stellate cells (HSC) → excessive collagen (type I/III) deposition → fibrosis.
- Architectural distortion → impaired blood flow through hepatic sinusoids → portal hypertension.
- Portosystemic shunting → ammonia bypasses liver → hepatic encephalopathy (mediated by portosystemic shunting, not cerebral edema as in ALF).
- Splanchnic vasodilation (via NO and vasodilators) → effective arterial underfilling → RAAS and sympathetic activation → sodium/water retention → ascites.
- Renal vasoconstriction via renin-angiotensin → hepatorenal syndrome (HRS).
- Reduced synthetic capacity: Hypoalbuminemia → edema; reduced clotting factors → coagulopathy; reduced thrombopoietin → thrombocytopenia.
- Intrapulmonary vascular dilation → ventilation-perfusion mismatch → hepatopulmonary syndrome.
- Immune dysfunction → susceptibility to spontaneous bacterial peritonitis (SBP).
🩺 Physical Examination
| Finding | Mechanism |
|---|---|
| Jaundice | Impaired bilirubin conjugation/excretion |
| Spider angiomata | Estrogen excess (impaired hepatic metabolism); >5 pathological |
| Palmar erythema | Hyperestrogenemia |
| Dupuytren's contracture | Fibroblast proliferation (especially in alcoholic cirrhosis) |
| Gynecomastia | Elevated estradiol/testosterone ratio |
| Testicular atrophy | Hypogonadism |
| Caput medusae | Dilated periumbilical veins (portal hypertension) |
| Splenomegaly | Portal hypertension |
| Ascites | Shifting dullness, fluid wave |
| Asterixis | Hepatic encephalopathy |
| Leukonychia (white nails) | Hypoalbuminemia |
| Clubbing | Hepatopulmonary syndrome |
| Parotid enlargement | Alcoholic cirrhosis |
| Muscle wasting / cachexia | Protein-calorie malnutrition |
| Fetor hepaticus | Mercaptan/sulfur compound accumulation |
🔬 Diagnostic Evaluation
| Test | Findings |
|---|---|
| LFTs (AST, ALT, GGT, ALP) | Variable; AST:ALT > 2:1 in alcoholic disease |
| Albumin | Low (<3.5 g/dL) |
| INR/PT | Prolonged |
| Platelet count | Low (portal hypertension → splenomegaly → sequestration; reduced thrombopoietin) |
| Bilirubin | Elevated |
| Serum ammonia | Elevated (correlates with encephalopathy) |
| Na-MELD score | Predicts 90-day mortality; guides transplant listing (score ≥15 = likely benefit) |
| Child-Pugh score | Bilirubin + albumin + INR + ascites + encephalopathy; grades A/B/C |
| Ultrasound + Doppler | Nodular liver, splenomegaly, ascites, portal vein flow |
| Liver biopsy | Gold standard for staging fibrosis; transjugular preferred |
| Fibroscan / elastography | Non-invasive fibrosis staging |
| Upper endoscopy | Esophageal/gastric varices surveillance |
| Paracentesis | SAAG ≥1.1 g/dL confirms portal hypertension-related ascites; cell count/culture for SBP |
| Serum alpha-fetoprotein + imaging | HCC surveillance every 6 months |
Scoring systems for prognosis:
- MELD (Model for End-stage Liver Disease) = 3.78×ln(bilirubin) + 11.2×ln(INR) + 9.57×ln(creatinine) + 6.43
- Na-MELD adds serum sodium; MELD ≥15 = transplant benefit
💊 Medication & Therapy
Portal hypertension management:
| Complication | Treatment |
|---|---|
| Esophageal varices (prophylaxis) | Non-selective beta-blockers (propranolol, nadolol, carvedilol) |
| Acute variceal hemorrhage | Octreotide (somatostatin analogue) + endoscopic band ligation (EBL); terlipressin where available; antibiotic prophylaxis (norfloxacin/ceftriaxone) |
| Refractory varices | TIPS (transjugular intrahepatic portosystemic shunt) |
Ascites management:
| Step | Treatment |
|---|---|
| First-line | Sodium restriction (<2 g/day) + spironolactone (100 mg/day); add furosemide if needed (100:40 ratio) |
| Refractory | Large-volume paracentesis + IV albumin (6–8 g per liter removed) |
| Last resort | TIPS; peritoneovenous shunt |
Hepatic encephalopathy:
| Agent | Mechanism |
|---|---|
| Lactulose | Non-absorbable disaccharide → acidifies colon → traps NH₄⁺; alters gut flora |
| Rifaximin | Non-absorbable antibiotic → reduces ammonia-producing gut bacteria |
| Dietary protein adjustment | Branch-chain amino acids (BCAAs) preferred over aromatic amino acids |
| Zinc supplementation | Cofactor in urea cycle enzymes |
Spontaneous bacterial peritonitis (SBP):
- Cefotaxime or ceftriaxone IV; + IV albumin reduces HRS risk
- Secondary prophylaxis: norfloxacin 400 mg/day or ciprofloxacin
Hepatorenal syndrome (HRS):
- Terlipressin (preferred) or norepinephrine + IV albumin
- Bridge to liver transplantation
Specific etiology treatment:
- HBV: entecavir / tenofovir (lifelong)
- HCV: direct-acting antivirals (DAAs) — curative in >95%
- ALD: abstinence ± corticosteroids (severe alcoholic hepatitis)
- MASLD: weight loss, metabolic control, GLP-1 agonists (emerging)
- Hemochromatosis: phlebotomy
- Wilson disease: penicillamine, trientine, zinc
Liver transplantation:
- Na-MELD ≥15: survival benefit confirmed
- Waiting list criteria: decompensation (ascites, variceal bleed, encephalopathy, SBP), HCC within Milan criteria
- 1-year post-transplant survival: >85%; 5-year: ~75%
─────────────────────────────────────
TYPE 3: ACUTE-ON-CHRONIC LIVER FAILURE (ACLF)
─────────────────────────────────────
📌 Definition
Acute deterioration of a previously compensated or decompensated chronic liver disease, precipitated by an acute hepatic or extrahepatic insult, resulting in organ failure and high short-term mortality. Defined by the EASL-CLIF consortium as ≥1 organ failure in a patient with cirrhosis.
🧪 Etiology
Chronic baseline (predisposing): Cirrhosis from any cause (HBV, HCV, alcohol, MASLD).
Acute precipitants (triggering):
| Type | Precipitant |
|---|---|
| Hepatic triggers | Alcoholic hepatitis flare, HBV reactivation, superimposed HAV/HEV, DILI |
| Extrahepatic triggers | Bacterial infection (SBP, pneumonia, UTI — most common), GI bleeding, surgery, TIPS-related, acute kidney injury |
| No identifiable trigger | ~40% of ACLF cases |
ACLF can be classified as Type A (on non-cirrhotic chronic liver disease), Type B (compensated cirrhosis), or Type C (decompensated cirrhosis). — Sleisenger & Fordtran's GI and Liver Disease
🧫 Pathology / Morphology
- Superimposed acute injury on a background of fibrosis/cirrhosis.
- Histology reflects both the chronic changes (nodular architecture, fibrous bands) and the acute insult (zone-specific necrosis, lobular inflammation).
- Systemic inflammation: markedly elevated pro-inflammatory cytokines (TNF-α, IL-6, IL-8) → drives organ failure cascade.
- Immune paralysis (CARS — compensatory anti-inflammatory response) coexists with SIRS → high infection susceptibility.
⚙️ Mechanism / Pathophysiology
- Two-hit model: Chronic liver injury (fibrosis, portal hypertension) + acute precipitant.
- Systemic inflammatory response: Massive cytokine storm → multiorgan dysfunction.
- Circulatory dysfunction: Splanchnic vasodilation → reduced effective arterial volume → renal, adrenal, and cerebral hypoperfusion.
- Bacterial translocation: Gut dysbiosis + increased intestinal permeability → bacterial products (LPS, PAMPs) enter portal circulation → activate Kupffer cells → perpetuate inflammation.
- Organ failure cascade: Renal failure (most common) → hepatic → coagulation → neurological → circulatory → respiratory.
🩺 Physical Examination
Combines features of chronic liver disease + acute decompensation:
- Jaundice (typically deep/rapidly worsening)
- Ascites (often tense, rapidly accumulating)
- Encephalopathy (asterixis, confusion, coma)
- Signs of infection (fever, hypotension, peritoneal tenderness)
- Oliguria (hepatorenal syndrome)
- Evidence of GI bleeding (melena, hematemesis)
- Signs of chronic liver disease (spider angiomata, caput medusae, splenomegaly)
🔬 Diagnostic Evaluation
- All tests from CLF apply, plus:
- CLIF-SOFA score (or CLIF-C ACLF score) — quantifies organ failure; score correlates directly with 28-day mortality
- Blood / ascitic fluid cultures — SBP diagnosis (PMN ≥250/mm³)
- Renal function trending — AKI (most common organ failure in ACLF)
- INR, factor V — acute coagulopathy on chronic background
- Lactate — tissue hypoperfusion
- Procalcitonin — bacterial infection marker
Prognosis:
- ACLF Grade 1 (1 organ failure): 28-day mortality ~22%
- ACLF Grade 2 (2 organ failures): ~32%
- ACLF Grade 3 (≥3 organ failures): ~74%
💊 Medication & Therapy
- Treat the precipitant first: antibiotics for infection, alcohol cessation + corticosteroids for alcoholic hepatitis (Maddrey's discriminant function ≥32), antiviral therapy for HBV reactivation.
- IV albumin (20–40 g/day × 5 days): reduces systemic inflammation and improves survival (ATTIRE/INFECIR trials).
- Renal support: CRRT preferred over intermittent hemodialysis.
- Vasopressors: Norepinephrine ± vasopressin for circulatory failure.
- Liver support systems: MARS, Prometheus — bridges but no definitive mortality benefit.
- Liver transplantation: Increasingly used for ACLF Grades 2–3 despite physiologic severity; survival benefit confirmed when transplanted within a narrow window.
🔄 Related Syndromes (Complications of Hepatocellular Insufficiency)
| Syndrome | Definition & Key Points |
|---|---|
| Hepatic Encephalopathy (HE) | Neuropsychiatric dysfunction from ammonia accumulation + neuro-inflammation. Graded 1–4. Asterixis is pathognomonic. Treat with lactulose + rifaximin. |
| Hepatorenal Syndrome (HRS) | Functional renal failure (no intrinsic kidney pathology) due to splanchnic vasodilation → renal vasoconstriction. Type 1 HRS = rapid onset (AKI pattern); Type 2 = chronic. Treat with terlipressin + albumin. Reversible with liver transplant. |
| Hepatopulmonary Syndrome (HPS) | Intrapulmonary vascular dilation → right-to-left shunting → hypoxemia. Platypnea-orthodeoxia (worsening hypoxia on standing). Diagnosed by contrast echocardiography. Transplant is curative. |
| Portopulmonary Hypertension | Pulmonary arterial hypertension in setting of portal hypertension. Elevated mean PAP >25 mmHg. May contraindicate transplantation if severe. |
| Spontaneous Bacterial Peritonitis (SBP) | Bacterial infection of ascitic fluid (PMN ≥250/mm³) without obvious source. Treat with cefotaxime + albumin. Prophylaxis with norfloxacin. |
| Hepatocellular Carcinoma (HCC) | Develops in 1–4% of cirrhotics per year. AFP + ultrasound surveillance every 6 months. Often the terminal event. |
| Coagulopathy of Liver Disease | Complex — reduced clotting factors AND reduced anticoagulants (Protein C/S) → "rebalanced hemostasis" that can tip toward bleeding OR thrombosis. |
| Hyponatremia | Dilutional (water retention > sodium retention); major complication; treated with fluid restriction + Na-MELD-guided transplant listing. |
| Hepatic Hydrothorax | Transdiaphragmatic passage of ascitic fluid → pleural effusion (usually right-sided). |
⚠️ Complications Summary
| System | Complication |
|---|---|
| Neurological | Hepatic encephalopathy, cerebral edema, intracranial hypertension |
| Cardiovascular | Cirrhotic cardiomyopathy, hyperdynamic circulation, hypotension |
| Renal | Hepatorenal syndrome (Types 1 & 2), acute tubular necrosis, hyponatremia |
| Pulmonary | Hepatopulmonary syndrome, portopulmonary hypertension, hepatic hydrothorax, aspiration pneumonia |
| Hematological | Coagulopathy, thrombocytopenia, variceal hemorrhage, DIC |
| Infectious | Spontaneous bacterial peritonitis, bacteremia, fungal infections, SIRS |
| Metabolic | Hypoglycemia, hyponatremia, metabolic alkalosis, hypophosphatemia, hypomagnesemia |
| Musculoskeletal | Sarcopenia, hepatic osteodystrophy |
| Oncological | Hepatocellular carcinoma (1–4%/year in cirrhotics) |
| Endocrine | Adrenal insufficiency, hypogonadism, hypothyroidism |
📊 Prognostic Scoring Summary
| Score | Components | Use |
|---|---|---|
| Child-Pugh | Bilirubin, albumin, INR, ascites, encephalopathy | Surgical risk, cirrhosis staging |
| MELD / Na-MELD | Creatinine, bilirubin, INR, Na | Transplant listing, 90-day mortality |
| King's College Criteria | pH, PT, creatinine, bilirubin, encephalopathy grade | ALF — transplant urgency |
| CLIF-SOFA / CLIF-C ACLF | 6 organ systems scored | ACLF grading and prognosis |
Sources:
- Robbins, Cotran & Kumar — Pathologic Basis of Disease (10th ed.)
- Robbins & Kumar — Basic Pathology
- Goldman-Cecil Medicine (International Edition)
- Tintinalli's Emergency Medicine
- Mulholland and Greenfield's Surgery
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.