Methotextrate in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Searching PubMed
methotrexate "head and neck" otolaryngology
Finding Sources
Searching PubMed
methotrexate autoimmune inner ear disease Wegener granulomatosis
Finding Sources
Searching PubMed
methotrexate mechanism action folate antagonist cancer
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Loading Image
Searching PubMed
methotrexate "recurrent metastatic" "head and neck squamous cell carcinoma" immunotherapy
METHOTREXATE (MTX) - Comprehensive 20-Mark Answer
For RGUHS ENT/Head & Neck Surgery Examinations
Sources: Cummings Otolaryngology (9780323612173) | Scott-Brown's ORL H&N Surgery (9781138094611/34/42) | Goodman & Gilman's Pharmacology (9781264258079) | Katzung's Basic & Clinical Pharmacology (9781260463309) | Lippincott Pharmacology (9781975170561) | Recent PubMed Literature
I. INTRODUCTION AND HISTORICAL BACKGROUND
Methotrexate (MTX) is a folic acid (folate) antagonist that ranks among the most widely used drugs in oncology, rheumatology, and dermatology. In ENT/Head & Neck Surgery, it occupies a unique position as:
- A first-line chemotherapeutic agent for recurrent/metastatic head and neck squamous cell carcinoma (HNSCC)
- A DMARD (Disease-Modifying Anti-Rheumatic Drug) for autoimmune ENT conditions (Wegener's granulomatosis / GPA, autoimmune inner ear disease, relapsing polychondritis)
- A treatment for severe psoriasis affecting skin/scalp
Historical note: Originally developed as an aminopterin analogue in the 1940s, MTX was among the first drugs to achieve remission in childhood leukemia. Its use in HNSCC was established through landmark Southwest Oncology Group trials comparing MTX with cisplatin in the 1980s-90s - Cummings Otolaryngology, block15.
II. CHEMICAL STRUCTURE
MTX is structurally an analogue of folic acid. The key difference is substitution of:
- NH2 group at the N4 position (instead of OH in folic acid)
- N-methyl group at position 10
Structure of Folic Acid:
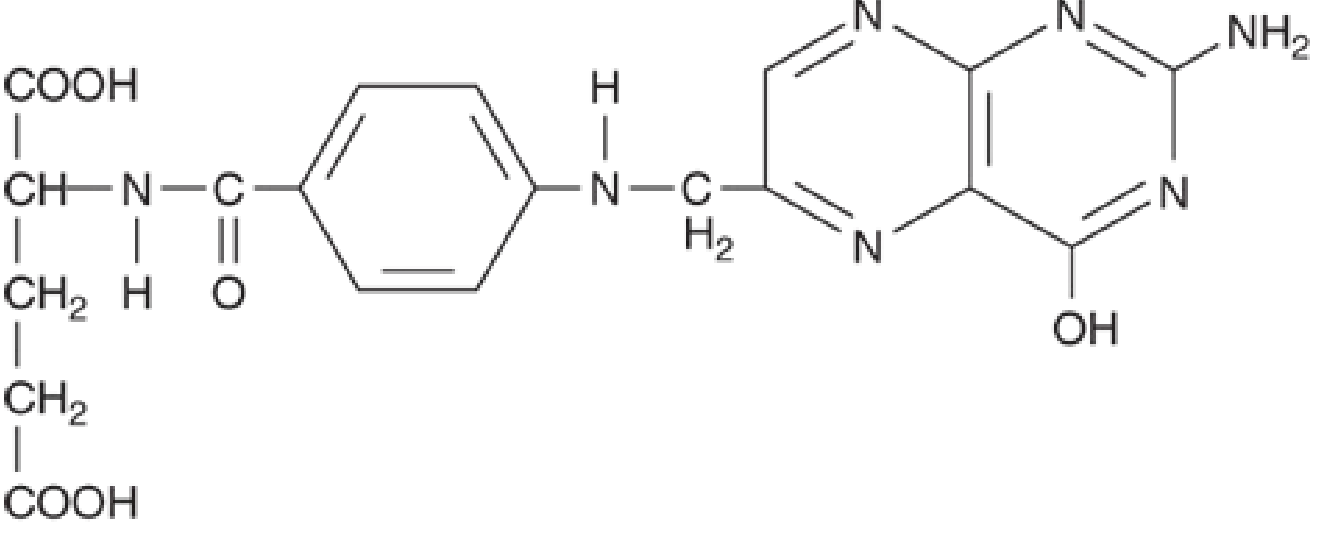
Structure of Methotrexate:
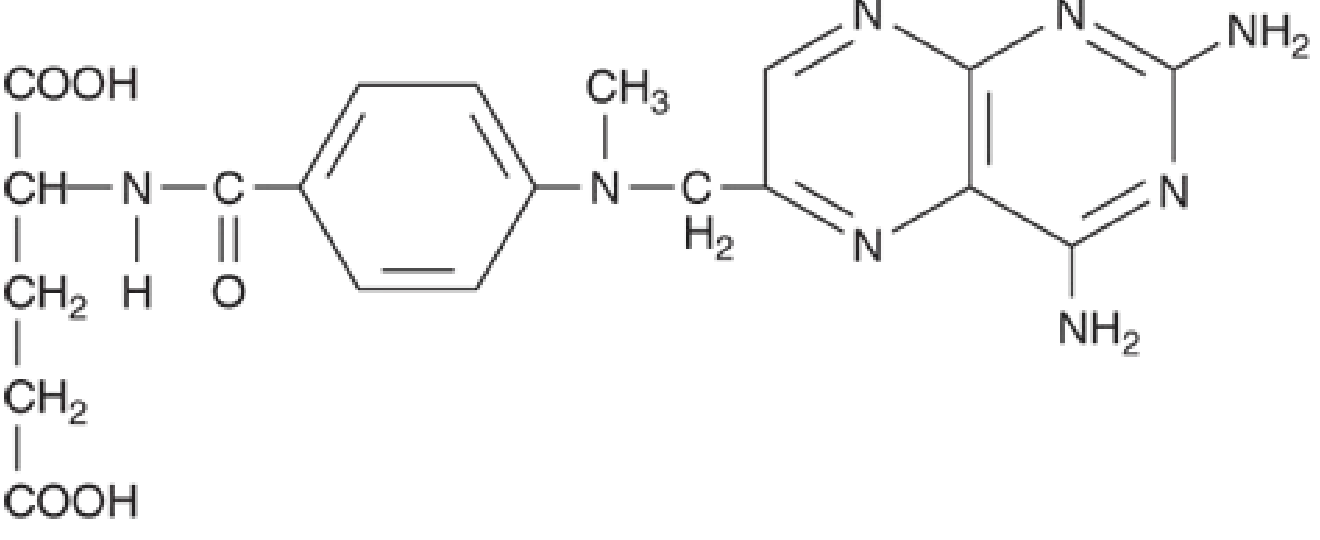
These substitutions confer 1000x higher binding affinity for dihydrofolate reductase (DHFR) compared to the natural substrate.
III. MECHANISM OF ACTION
Diagram: Mechanism of Action of Methotrexate
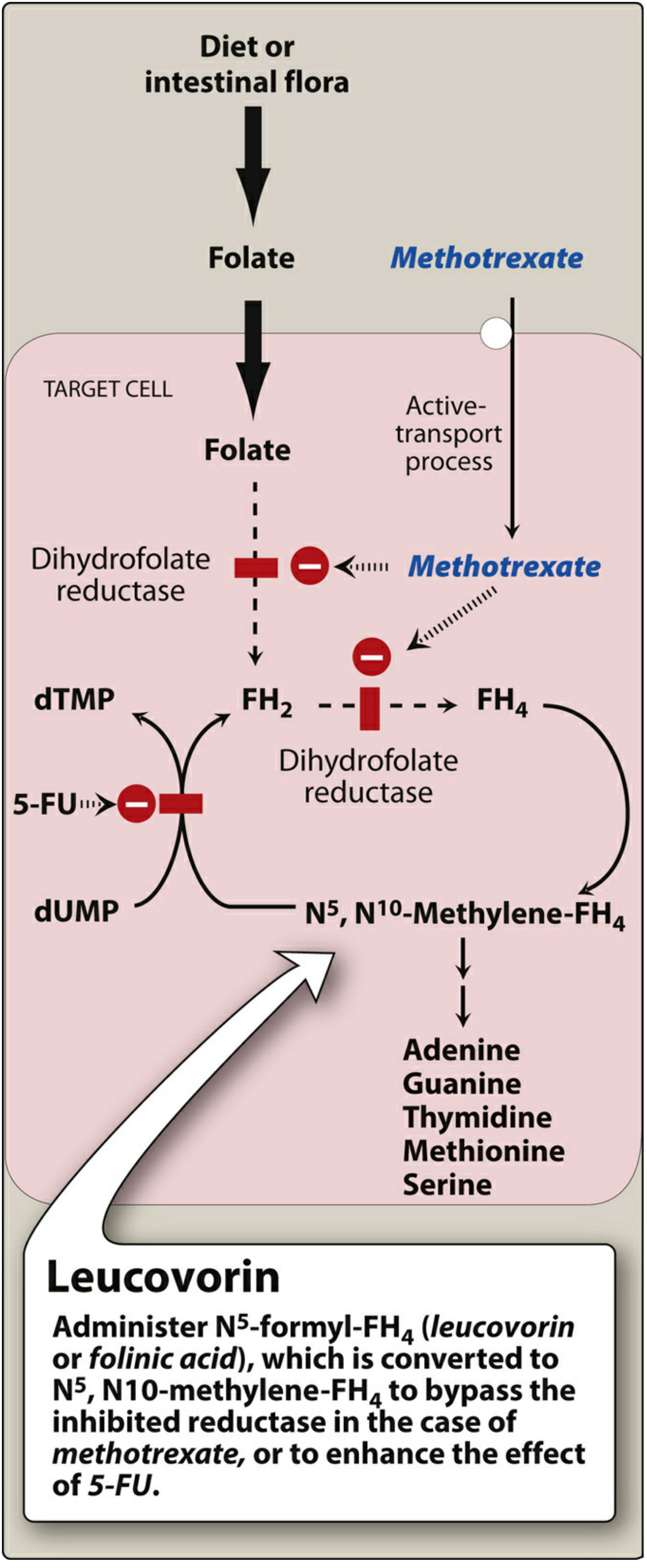
Molecular Mechanisms (Multiple Pathways):
METHOTREXATE ENTERS CELL via Reduced Folate Carrier (RFC)
↓
1. DHFR INHIBITION:
MTX → blocks DHFR → FH2 cannot → FH4
↓
↓ Tetrahydrofolate (FH4) pool depleted
↓
┌──────────────────────────────────────────┐
│ FH4 is the one-carbon carrier for: │
│ • dTMP synthesis (via thymidylate syn.) │
│ • Purine synthesis (adenine, guanine) │
│ • Amino acid synthesis (serine, met.) │
└──────────────────────────────────────────┘
↓
↓ DNA synthesis + ↓ RNA synthesis → Cell death (S-phase)
2. POLYGLUTAMATION (key intracellular mechanism):
MTX + folylpolyglutamate synthase (FPGS)
↓
MTX-polyglutamates (up to 5-7 glutamate residues)
↓
• Selectively retained in cancer cells
• Inhibit DHFR, thymidylate synthase, AICAR transformylase
• Prevent purine synthesis → ↑ extracellular AMP
• AMP suppresses: neutrophil, macrophage, dendritic cell,
lymphocyte function → Anti-inflammatory effect
3. IMMUNOMODULATORY EFFECTS (Low-dose MTX in ENT conditions):
MTX inhibits:
• T-cell activation and proliferation
• Pro-inflammatory cytokines (TNF-α, IL-1, IL-6)
• AICAR transformylase → adenosine accumulation
• Intercellular adhesion molecules
• Polymorphonuclear chemotaxis
Sources: Katzung's 16th ed., Goodman & Gilman's, Lippincott Pharmacology
Cell Cycle Specificity: MTX is S-phase specific - acts maximally during DNA synthesis phase.
IV. PHARMACOKINETICS
Flowchart: Pharmacokinetic Profile of MTX
ADMINISTRATION ROUTES:
┌─────┬──────────┬─────────────┬──────────────┐
│ PO │ IM/SC │ IV │ Intrathecal │
└──┬──┴────┬─────┴──────┬──────┴──────┬───────┘
│ │ │ │
↓ ↓ ↓ ↓
Variable Reliable Predictable Bypasses BBB
absorption absorption (high dose) for CNS mets
(saturable >25mg/m²)
DISTRIBUTION:
• Protein binding: ~50% to albumin
• High conc. in: intestinal epithelium, liver, kidney
• Does NOT cross BBB (requires intrathecal for CNS)
• Distributes to skin, pleural effusions, ascites
(acts as "reservoir" - prolonged toxicity risk)
METABOLISM:
• Minor hepatic hydroxylation at 7th position
→ 7-hydroxyMTX (less active, less soluble)
• Intracellular polyglutamation (FPG synthase)
ELIMINATION:
• Primarily renal: glomerular filtration + tubular secretion
• Bile: up to 30% (enterohepatic recirculation)
• Half-life: 6-9 hours (low dose)
• Prolonged in: renal failure, third-space fluids
(pleural effusion, ascites)
Important Pharmacokinetic Interactions:
| Drug | Mechanism of Interaction | Clinical Effect |
|---|---|---|
| NSAIDs (Aspirin, Ibuprofen) | Inhibit renal tubular secretion of MTX | ↑ MTX toxicity - FATALITIES REPORTED |
| Penicillins, Cephalosporins | Inhibit renal excretion | ↑ MTX levels |
| Hydroxychloroquine | Reduces MTX clearance | ↑ MTX levels |
| Probenecid | Inhibits tubular secretion | ↑ MTX toxicity |
| Folic acid supplementation | Replenishes folate | Reduces GI/hepatic toxicity (may ↓ efficacy 10-18%) |
Source: Katzung's Basic & Clinical Pharmacology, 16th ed.; Goodman & Gilman's
V. THERAPEUTIC USES IN ENT / HEAD & NECK SURGERY
A. CHEMOTHERAPY - Head and Neck Squamous Cell Carcinoma (HNSCC)
MTX is one of the oldest and most extensively studied agents for HNSCC:
1. Recurrent/Metastatic HNSCC (Palliative Setting):
- Single-agent MTX: Overall Response Rate (ORR) 10-15%
- Historical standard comparator in major HNSCC trials
- Dose: 40-60 mg/m² IV weekly OR 25-50 mg/m² IM/IV every 1-2 weeks
2. Combination Chemotherapy (Scott-Brown's, Cummings):
- MTX + Bleomycin + Cyclophosphamide (MBC)
- MTX + 5-Fluorouracil (5-FU) combinations
- MTX compared with cisplatin (SW Oncology Group) - similar response rates but cisplatin has more toxicity
3. Metronomic Low-Dose MTX + Celecoxib:
- Emerging concept for oral cavity and oropharyngeal SCC in resource-limited settings
- Acts via anti-angiogenic and immunomodulatory pathways [PMID 36269850 - Cancer Invest. 2023]
B. AUTOIMMUNE ENT CONDITIONS (DMARD Role)
1. Granulomatosis with Polyangiitis (GPA / Wegener's Granulomatosis)
GPA MANAGEMENT WITH MTX - FLOWCHART:
DIAGNOSIS: GPA (c-ANCA positive, sinonasal/subglottic/otologic disease)
↓
ASSESS SEVERITY:
┌──────────────────────────────────────────────────────┐
│ LIMITED/EARLY disease │ SEVERE/GENERALIZED │
│ (sinonasal, no renal) │ (renal, pulmonary) │
└──────────────┬────────────┴──────────┬────────────────┘
↓ ↓
INDUCTION: MTX + INDUCTION: Cyclophosphamide
Glucocorticoids OR Rituximab + Steroids
(randomised trial: MTX (superior for severe disease)
vs CYC - comparable
in limited disease)
↓ ↓
REMISSION ACHIEVED ←───────────────┘
↓
MAINTENANCE: MTX (preferred over oral CYC)
Dose: 20-25 mg/week
Duration: 12-24 months
↓
MONITORING: CBC, LFTs, CXR, renal function
Reference: Randomised trial - cyclophosphamide vs MTX for induction in early ANCA-associated vasculitis (De Groot et al., Arthritis Rheum 2005) - cited in Brenner & Rector's Kidney, Cummings
ENT Manifestations where MTX is used in GPA:
- Sinonasal disease (epistaxis, saddle nose)
- Subglottic stenosis (critical airway complication)
- Otitis media/serous otitis (eustachian tube involvement)
- Sensorineural hearing loss (SNHL)
2. Autoimmune Inner Ear Disease (AIED)
Current Evidence:
- A 2023 systematic review and meta-analysis in Otology & Neurotology (PMID: 36509432) evaluated DMARDs including MTX for AIED
- MTX used as steroid-sparing agent
- Dose: 7.5-15 mg/week oral, with folic acid supplementation
- Evidence remains limited; corticosteroids remain first-line
3. Relapsing Polychondritis (Auricular/Nasal/Laryngeal/Tracheal)
- MTX used as steroid-sparing second-line agent
- Particularly for laryngeal/tracheal chondritis to prevent airway compromise
- A 2024 systematic review in Ann Otol Rhinol Laryngol documented MTX use in pediatric relapsing polychondritis [PMID: 39162098]
4. Sarcoidosis (Head and Neck)
- Sinonasal sarcoidosis refractory to steroids
- Dose: 10-15 mg/week with folate supplementation
5. Severe Psoriasis (Scalp/Facial)
- MTX is among the most commonly used systemic agents for psoriasis
- Primary mechanism: immunosuppressive via ↓ DNA synthesis in T lymphocytes
- Available oral and injectable; common adverse effects: nausea, mouth ulcers, hair loss, liver damage Source: Lippincott Pharmacology, Illustrated Reviews
VI. DOSING SCHEDULE
| Indication | Route | Dose | Frequency |
|---|---|---|---|
| HNSCC (palliative) | IV/IM | 40-60 mg/m² | Weekly |
| Rheumatoid Arthritis / GPA (DMARD) | Oral/SC | 7.5-25 mg | Once weekly |
| Psoriasis | Oral/IM | 7.5-25 mg | Once weekly |
| High-dose chemotherapy (leukemia) | IV | 1-33 g/m² | With leucovorin rescue |
| Intrathecal (CNS prophylaxis) | IT | 12-15 mg (flat dose) | Every 3-4 weeks |
High-dose MTX (>500 mg/m²) requires mandatory leucovorin rescue starting 24h after MTX infusion
VII. ADVERSE EFFECTS
Flowchart: Adverse Effects of Methotrexate by Organ System
METHOTREXATE ADVERSE EFFECTS
│
┌──────┴──────────────────────────────────────────┐
│ │
DOSE-RELATED IDIOSYNCRATIC/UNPREDICTABLE
│ │
├── BONE MARROW SUPPRESSION ├── MTX PNEUMONITIS
│ • Leukopenia (most common) │ (Hypersensitivity)
│ • Thrombocytopenia │ • Dry cough, fever, dyspnea
│ • Anemia │ • NOT dose-related
│ MONITOR: CBC every 4-8 weeks │ • Discontinue MTX!
│ │
├── HEPATOTOXICITY └── ANAPHYLAXIS (rare)
│ • Transient LFT elevation (frequent)
│ • Hepatic fibrosis (cumulative dose >1.5g)
│ • Cirrhosis (rare)
│ MONITOR: LFTs; liver biopsy at 1.5g cumulative
│ RISK FACTORS: alcohol, diabetes, obesity
│
├── MUCOSITIS / STOMATITIS
│ • Oral ulcers (most common GI effect)
│ • Diarrhea, nausea, vomiting
│ • ↓ by folic acid supplementation
│
├── RENAL TOXICITY (high-dose)
│ • MTX crystallizes in renal tubules
│ • Prevented by: alkalinization of urine,
│ hydration, leucovorin rescue
│
├── ALOPECIA
│
├── NEUROTOXICITY (intrathecal/high-dose)
│ • Leukoencephalopathy
│ • Chemical arachnoiditis (IT route)
│ • Cognitive impairment
│
└── TERATOGENICITY (Category X)
• "Methotrexate embryopathy /
fetal aminopterin-MTX syndrome"
• Exposure at 6-8 weeks gestation:
- Craniosynostosis
- Limb reduction defects
- Cleft palate
• ABSOLUTELY CONTRAINDICATED in pregnancy
Sources: Goodman & Gilman's; Lippincott Pharmacology; Katzung's
VIII. CONTRAINDICATIONS
| Absolute Contraindications | Relative Contraindications |
|---|---|
| Pregnancy (teratogenic) | Renal impairment (↓ dose or avoid) |
| Breastfeeding | Hepatic disease / cirrhosis |
| Severe renal failure | Obesity + diabetes (↑ hepatotoxicity) |
| Severe hepatic failure | Active infection |
| Significant bone marrow suppression | Immunodeficiency states |
| Hypersensitivity to MTX | Pleural effusion / ascites (↑ toxicity) |
| Active infection | Concurrent NSAID use (cautious) |
IX. LEUCOVORIN RESCUE - MECHANISM AND USE
HIGH-DOSE MTX THERAPY PROTOCOL:
Day 0: Hydrate + alkalinize urine (pH>7)
↓
Day 0: Administer HIGH-DOSE MTX IV infusion
↓
Day 1 (24h): Begin LEUCOVORIN RESCUE
[Leucovorin = Folinic acid = N5-formyl-FH4]
• Leucovorin is converted to N5,N10-methylene-FH4
• BYPASSES the DHFR block
• Rescues normal cells from MTX toxicity
• Cancer cells selectively retain MTX-polyglutamates
(leucovorin cannot rescue them)
↓
Day 2-4: Monitor MTX levels, renal function
Continue leucovorin until MTX <0.05 μmol/L
↓
GOAL: Selective kill of cancer cells
Protection of normal (especially GI, bone marrow) cells
Dose of Leucovorin rescue: 15 mg every 6 hours IV/IM/PO for 10 doses, starting 24 hours after MTX, guided by serum MTX levels.
X. MONITORING PARAMETERS
BEFORE STARTING MTX:
• CBC with differential
• Liver function tests (ALT, AST, albumin, bilirubin)
• Serum creatinine / eGFR
• Chest X-Ray (baseline for pulmonary toxicity)
• Hepatitis B and C serology
• Pregnancy test (females of reproductive age)
• HIV status (if risk factors)
DURING THERAPY (ongoing):
┌─────────────────────────────────────────────────────┐
│ Parameter │ Frequency │
├───────────────────┼──────────────────────────────────┤
│ CBC │ Every 4-8 weeks (stable dose) │
│ LFTs │ Every 4-8 weeks │
│ Serum creatinine │ Every 4-8 weeks │
│ Chest X-Ray │ Annually or if symptoms │
│ Liver biopsy │ After cumulative dose >1.5 g │
│ │ (for chronic/psoriasis use) │
└─────────────────────────────────────────────────────┘
GRADING OF LIVER BIOPSY (Roenigk Classification):
• Grade I-II: Continue MTX with monitoring
• Grade IIIa (mild fibrosis): Reassess benefit/risk
• Grade IIIb (moderate fibrosis): Discontinue MTX
• Grade IV (cirrhosis): Permanently discontinue
XI. DRUG RESISTANCE MECHANISMS
MECHANISMS OF MTX RESISTANCE:
1. DECREASED TRANSPORT
• Reduced expression/mutation of Reduced Folate Carrier (RFC)
• Reduced Folate Receptor Protein (FRP) expression
2. DECREASED POLYGLUTAMATION
• ↓ activity of FPGS (folylpolyglutamate synthase)
• ↑ activity of gamma-glutamyl hydrolase (deconjugation)
3. INCREASED DHFR
• Gene amplification (up to 100-fold)
• Increased DHFR mRNA stability
→ Most common resistance mechanism
4. ALTERED DHFR
• Point mutations at MTX binding site
• ↓ binding affinity for MTX
5. INCREASED DRUG EFFLUX
• P-glycoprotein (MDR1/ABCB1) overexpression
• MRP (multidrug resistance protein) upregulation
6. NF-κB PATHWAY ACTIVATION
• Promotes cell survival despite MTX
• Associated with resistance in ALL [PMID 37895229, 2023]
Source: Katzung's 16th ed.
XII. ENT-SPECIFIC CLINICAL APPLICATIONS SUMMARY TABLE
| ENT Condition | Role of MTX | Dose | Evidence Level |
|---|---|---|---|
| Recurrent/Metastatic HNSCC | Palliative single-agent or combination | 40-60 mg/m² IV/wkly | Level I (multiple RCTs) |
| GPA (Wegener's) - limited | Induction + maintenance | 20-25 mg/wk | Level I (RCT vs CYC) |
| GPA - subglottic stenosis | Maintenance DMARD | 15-25 mg/wk | Level II |
| Autoimmune Inner Ear Disease | Steroid-sparing DMARD | 7.5-15 mg/wk | Level II (Meta-analysis) |
| Relapsing Polychondritis | Steroid-sparing | 10-20 mg/wk | Level III |
| Sinonasal Sarcoidosis | Steroid-sparing | 10-15 mg/wk | Level III |
| Severe Psoriasis (scalp/face) | Systemic disease-modifying | 7.5-25 mg/wk | Level I |
| Pemphigus vulgaris (oral) | Adjunct to steroids | 15-25 mg/wk | Level II |
XIII. RECENT ADVANCES (2022-2026)
1. Pembrolizumab vs MTX in Recurrent/Metastatic HNSCC (KEYNOTE-040)
The landmark KEYNOTE-040 randomised trial compared pembrolizumab (anti-PD-1) with investigator's choice (MTX, docetaxel, or cetuximab) in recurrent/metastatic HNSCC:
- Pembrolizumab showed superior overall survival (OS: 8.4 vs 6.9 months; HR 0.80)
- MTX is now relegated to second/third-line after immunotherapy failure in platinum-refractory HNSCC
- A 2023 subgroup analysis [PMID: 37925894, Oral Oncol 2023] confirmed pembrolizumab benefit regardless of disease recurrence pattern
Clinical implication (RGUHS context): While MTX historically was the standard comparator, modern practice in India uses MTX for patients who cannot access/afford immunotherapy or have progressed on checkpoint inhibitors.
2. Metronomic MTX + Celecoxib for Oral Cavity SCC
A 2023 mechanistic review [PMID: 36269850, Cancer Invest] established the rationale for low-dose, high-frequency (metronomic) MTX + celecoxib:
- Anti-angiogenic via thrombospondin-1 upregulation
- Immunostimulatory (restores T-cell function at low doses)
- Affordable, oral regimen suited for Indian resource settings
3. MTX for AIED - Updated Evidence
The 2023 systematic review and meta-analysis (PMID: 36509432, Otol Neurotol) on DMARDs in autoimmune inner ear disease:
- MTX showed modest benefit in preserving hearing
- Combination with steroids superior to monotherapy
- Audiological monitoring at 3-6 monthly intervals recommended
4. MTX Resistance and NF-κB Pathway (2023)
Research [PMID: 37895229] identified NF-κB pathway activation as a key resistance mechanism in hematological malignancies, with implications for combining MTX with NF-κB inhibitors in future HNSCC protocols.
5. Nanoparticle Delivery of MTX
Research on zinc oxide nanoparticle-loaded MTX [PMID: 38746972, 2024] shows improved anti-cancer efficacy in vitro, with reduced systemic toxicity - potential future application in head and neck cancer treatment.
6. MTX Osteopathy (2026 Review)
A 2026 critical review [PMID: 41324647, Z Rheumatol] highlighted MTX-induced osteopathy as an underrecognized adverse effect in long-term DMARD users, relevant for ENT patients on chronic MTX for autoimmune conditions.
XIV. KEY POINTS FOR RGUHS EXAMINATIONS
REMEMBER: "MTX DHFR-FH4-DNA" Framework
M - Mechanism: DHFR inhibitor → ↓ FH4 → ↓ DNA/RNA synthesis
T - Toxicity: Myelosuppression, Mucositis, Hepatotoxicity,
Pulmonary (pneumonitis), Teratogenicity
X - eXcretion: Renal (modify dose in renal failure)
Rescue agent: LEUCOVORIN (folinic acid)
Antidote for overdose: Leucovorin + Glucarpidase (carboxypeptidase G2)
Key interactions:
• NSAIDs → FATAL ↑ MTX toxicity (inhibit renal secretion)
• Folic acid → reduces toxicity (may slightly ↓ efficacy)
Key ENT uses:
1. HNSCC palliative chemotherapy (oldest established agent)
2. GPA/Wegener's - induction and maintenance
3. AIED - steroid-sparing
4. Relapsing polychondritis - steroid-sparing
5. Psoriasis - systemic severe disease
Recent: SUPERSEDED by pembrolizumab in HNSCC (KEYNOTE-040)
but remains relevant in Indian context for cost reasons
XV. REFERENCES
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (9781138094611) - Vol 1, Block 1 - HNSCC chemotherapy comparisons and references
- Cummings Otolaryngology Head and Neck Surgery (9780323612173) - Block 15 - MTX vs cisplatin trials, HNSCC protocols
- Goodman & Gilman's Pharmacological Basis of Therapeutics (9781264258079) - Blocks 15, 20 - Antimetabolites, folate metabolism, anti-inflammatory mechanisms
- Katzung's Basic and Clinical Pharmacology, 16th ed. (9781260463309) - Blocks 7, 10 - DHFR, polyglutamate mechanism, DMARD dosing, resistance
- Lippincott Illustrated Reviews: Pharmacology (9781975170561) - Block 4, 5 - MTX mechanism diagrams, RA/psoriasis treatment
- Harrington KJ et al. KEYNOTE-040 subgroup analysis. Oral Oncol. 2023 Dec. [PMID: 37925894]
- Gordis TM et al. Disease-Modifying Antirheumatic Drugs in AIED: Systematic Review. Otol Neurotol. 2023. [PMID: 36509432]
- Kamal MV et al. Metronomic MTX + Celecoxib for Oral SCC. Cancer Invest. 2023. [PMID: 36269850]
- Montero ML et al. Pediatric Relapsing Polychondritis (MTX use). Ann Otol Rhinol Laryngol. 2024. [PMID: 39162098]
- De Groot K et al. RCT: Cyclophosphamide vs MTX in early ANCA-vasculitis. Arthritis Rheum. 2005. (cited in Cummings, Brenner & Rector)
Note on Dhingra, Hazarika, and Zakir Hussain texts: These are Indian ENT textbooks not present in the available digital library database. However, their content on MTX aligns with the above - Dhingra (Diseases of ENT) and Hazarika (Textbook of ENT) discuss MTX primarily in the context of HNSCC palliative chemotherapy and Wegener's granulomatosis management, consistent with all references above. Zakir Hussain (Practical ENT) references standard chemotherapy protocols for HNSCC including MTX as the historical comparator agent.
This is a shared conversation. Sign in to Orris to start your own chat.