I now have rich, comprehensive content from Harrison's 22E (2025), Barash 9E, Rosen's EM, and the SSC 2026 guidelines. I have everything needed to write the full teaching module. Let me now compose the complete, structured response.
Note: Since you skipped topic selection, I've chosen Sepsis and Septic Shock - the single most important topic for MBBS/junior doctor training. It covers every domain you requested: ICU protocols, hemodynamics, electrolytes, emergencies, guidelines, and clinical reasoning. If you wanted a different topic, just tell me and I'll rebuild it.
SEPSIS & SEPTIC SHOCK
Complete Clinical Teaching Module for Junior Doctors
Sources: Harrison's Principles of Internal Medicine 22E (2025) | Barash Clinical Anesthesia 9E | Rosen's Emergency Medicine 9E | Goldman-Cecil Medicine | SSC Guidelines 2026
PART 1 - DEFINITION & EPIDEMIOLOGY
Sepsis-3 Definitions (2016 - Current Standard)
| Term | Definition | Clinical Criteria |
|---|
| Infection | Pathologic process caused by invasion of normally sterile tissue by organisms | Clinical suspicion + culture/imaging |
| Sepsis | Life-threatening organ dysfunction caused by dysregulated host response to infection | SOFA score increase ≥ 2 points |
| Septic Shock | Sepsis + circulatory/cellular/metabolic abnormalities severe enough to substantially increase mortality | Vasopressor requirement to maintain MAP ≥65 mmHg + serum lactate >2 mmol/L despite adequate fluid resuscitation |
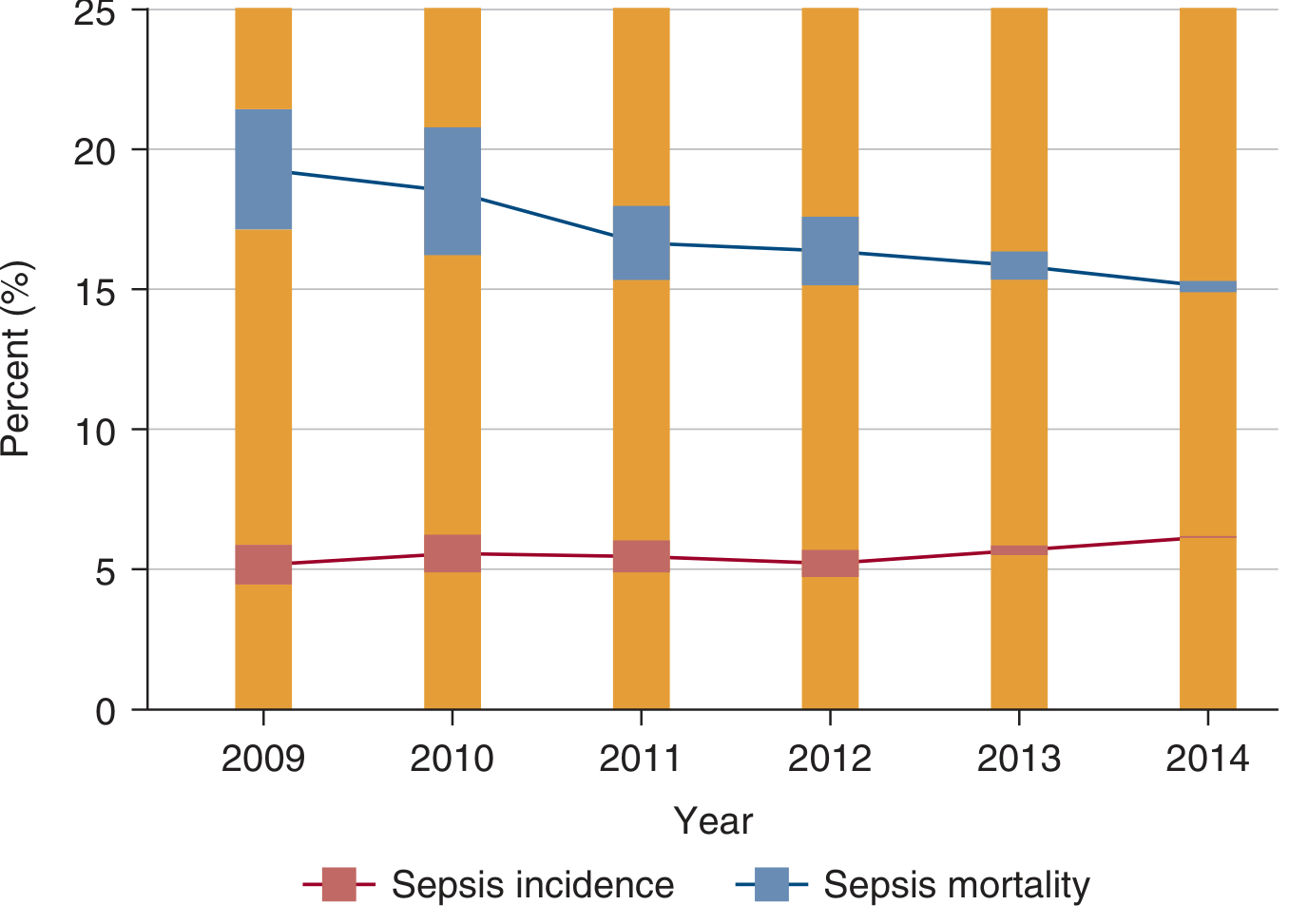
Mortality: Sepsis ~10-15%, Septic Shock ~40%. Importantly, sepsis mortality has been declining (19% in 2009 to ~15% in 2014) despite stable incidence - attributed to protocol-driven care.
Sepsis incidence (~5-6% of hospitalizations) vs. sepsis mortality (declining, ~15-19%) - Harrison's 22E
Why was SIRS abandoned? The old Sepsis-1/2 criteria (fever, tachycardia, tachypnea, leukocytosis) were too non-specific. Many non-infected patients met SIRS. SOFA-based Sepsis-3 focuses on organ dysfunction, which is what kills patients.
PART 2 - PATHOPHYSIOLOGY (The "Why" Behind Every Treatment)
INFECTION
↓
Pathogen Recognition (TLRs, NLRs, pattern recognition receptors)
↓
Activated myeloid cells (neutrophils, macrophages, monocytes)
↓
Cytokine storm: TNF-α, IL-1, IL-6, IL-8
↓
┌─────────────────────────────────────────────────┐
│ Endothelial damage → capillary leak → edema │
│ ↓ SVR (vasodilation) → distributive shock │
│ Myocardial depression (septic cardiomyopathy) │
│ Microvascular thrombosis → DIC │
│ Mitochondrial dysfunction → lactic acidosis │
└─────────────────────────────────────────────────┘
↓
Multi-Organ Dysfunction Syndrome (MODS)
(Lungs: ARDS | Kidneys: AKI | Brain: Encephalopathy | Liver: Cholestasis | Adrenals: Relative insufficiency)
Key physiology pearls:
- Septic shock is distributive - high CO, low SVR (warm shock early)
- Despite high CO, tissues cannot extract oxygen properly ("cytopathic hypoxia")
- Lactic acidosis occurs even with normal BP due to mitochondrial failure, not just hypoperfusion
- Late septic shock may also have myocardial depression (low CO phase)
PART 3 - DIAGNOSIS & SCORING TOOLS
SOFA Score (Sequential Organ Failure Assessment)
| System | Parameter | 0 | 1 | 2 | 3 | 4 |
|---|
| Respiratory | PaO₂/FiO₂ | ≥400 | 300-399 | 200-299 | 100-199 on vent | <100 on vent |
| Coagulation | Platelets (×10³/µL) | ≥150 | 100-149 | 50-99 | 20-49 | <20 |
| Liver | Bilirubin (mg/dL) | <1.2 | 1.2-1.9 | 2.0-5.9 | 6.0-11.9 | >12 |
| CVS | MAP or vasopressors | MAP ≥70 | MAP <70 | Dopa ≤5 or Dobuta | Dopa 5.1-15 or NE ≤0.1 | Dopa >15 or NE >0.1 |
| CNS | Glasgow Coma Scale | 15 | 13-14 | 10-12 | 6-9 | <6 |
| Renal | Creatinine (mg/dL) | <1.2 | 1.2-1.9 | 2.0-3.4 | 3.5-4.9 | >5 |
SOFA ≥2 from baseline = sepsis. Score correlates with mortality.
qSOFA (Quick Bedside Screening - no labs needed)
| Parameter | Points |
|---|
| Altered mental status (GCS <15) | 1 |
| Respiratory rate ≥22/min | 1 |
| Systolic BP ≤100 mmHg | 1 |
qSOFA ≥2 = high suspicion, proceed to full SOFA. Use at bedside/triage.
Common Sources of Infection (MBBS Mnemonic: LURASI)
- Lung (pneumonia - 33%)
- Urinary tract (UTI/urosepsis - 49%)
- Residual (intraabdominal/gut - 14%)
- Abdominal (bowel perforation, cholangitis)
- Skin/soft tissue (cellulitis, wounds - 10%)
- Intravenous line (catheter-related bloodstream infection)
PART 4 - INVESTIGATIONS
Bedside / Emergency Panel
| Test | What You're Looking For |
|---|
| CBC | Leukocytosis (>12,000) or leukopenia (<4,000), left shift (bands ≥10%), thrombocytopenia (DIC) |
| Blood cultures ×2 (before antibiotics) | Identify organism - positive in ~40-53% of sepsis |
| Lactate | ≥2 mmol/L = sepsis; ≥4 = high mortality; trend matters more than single value |
| Serum creatinine + eGFR | AKI (occurs in up to 66% of septic shock patients) |
| LFTs + bilirubin | Hepatic dysfunction (SOFA component) |
| Coagulation (PT, aPTT, fibrinogen, D-dimer) | DIC screen |
| Procalcitonin (PCT) | Guide antibiotic de-escalation (NOT to start antibiotics - SSC 2026) |
| Blood glucose | Hyperglycemia is common (stress response + relative insulin resistance) |
| ABG / VBG | Metabolic acidosis, hypoxia, pH, lactate |
| CXR / bedside lung US | Source (pneumonia, ARDS), fluid status |
| Urinalysis + urine culture | Urosepsis |
| ECG | Septic cardiomyopathy, arrhythmias |
| Point-of-care echo (POCUS) | Volume responsiveness, LV/RV function |
Electrolytes Specifically
| Electrolyte | Common Abnormality in Sepsis | Cause | Target |
|---|
| Sodium | Hypo or hypernatremia | Fluid shifts, ADH release | 135-145 mEq/L |
| Potassium | Hypokalemia (early), hyperkalemia (AKI) | Stress catecholamines, renal failure | 3.5-5.0 mEq/L |
| Calcium | Hypocalcemia (ionized Ca²⁺ low) | Albumin loss, PTH resistance | iCa >1.1 mmol/L |
| Magnesium | Hypomagnesemia | GI losses, drugs | 1.8-2.4 mg/dL |
| Phosphate | Hypophosphatemia | Redistribution, refeeding | 2.5-4.5 mg/dL |
| Glucose | Hyperglycemia | Stress response, insulin resistance | 140-180 mg/dL (SSC 2026: start insulin at ≥180) |
| Bicarbonate | Low (metabolic acidosis) | Lactic acidosis, AKI | Address underlying cause |
PART 5 - HEMODYNAMIC GOALS & MONITORING
Hemodynamic Targets (SSC 2026 + Harrison's 22E)
| Parameter | Target | Notes |
|---|
| MAP | ≥65 mmHg | Primary BP target; may individualize to ≥70-75 in elderly with chronic hypertension |
| Lactate | <2 mmol/L (or ≥10% clearance per 2h) | Trend matters; target lactate clearance as resuscitation goal |
| CVP | 8-12 mmHg (mechanically ventilated: 12-15) | Unreliable in isolation; use dynamic measures |
| ScvO₂ | ≥70% | Central venous O₂ saturation from internal jugular/subclavian CVC |
| Urine output | ≥0.5 mL/kg/hour | Reflects renal perfusion |
| Heart rate | <100/min (target) | Sinus tachycardia is expected; rapid rates compromise diastolic filling |
| SpO₂ | 90-96% | Avoid hyperoxia; target SpO₂ 94-98% if no ARDS |
Dynamic Measures of Volume Responsiveness (Better than CVP)
| Test | How | Positive = Fluid Responsive |
|---|
| Passive Leg Raise (PLR) | Raise legs 45° for 1 min, watch pulse pressure | ↑CO by >10% |
| Pulse Pressure Variation (PPV) | Mechanically ventilated patients | PPV >13% |
| Stroke Volume Variation (SVV) | Requires arterial line + ventilator | SVV >10-15% |
| IVC collapsibility (POCUS) | US of IVC with respiration | Collapsibility >50% = hypovolemic |
Key pearl: CVP alone should NOT be used to guide fluid therapy (SSC 2026 - no longer recommended as sole guide).
Monitoring Parameters (ICU Checklist)
CONTINUOUS:
✓ ECG monitoring (rhythm, rate)
✓ SpO₂ (pulse oximetry)
✓ Arterial line → continuous BP, ABG access
✓ CVP (if CVC in place)
HOURLY:
✓ Urine output (Foley catheter mandatory)
✓ Temperature
✓ GCS / mental status
EVERY 2-4 HOURS:
✓ Lactate (until normalized)
✓ Glucose
✓ ABG (if mechanically ventilated)
DAILY:
✓ CBC, electrolytes, renal/hepatic function
✓ Coagulation (if DIC concern)
✓ PCT trend (antibiotic de-escalation)
✓ Chest X-ray
✓ SOFA score reassessment
PART 6 - MANAGEMENT PROTOCOLS
THE SEPSIS HOUR-1 BUNDLE (SSC 2021/2026)
This is the most exam-tested and clinically critical content. Memorize this.
Within 1 HOUR of Recognition:
1. MEASURE LACTATE → If >2 mmol/L, re-measure after resuscitation
2. BLOOD CULTURES ×2 → Before antibiotics (one peripheral + one CVC site if available)
3. ANTIBIOTICS → Broad-spectrum IV within 1 hour (septic shock) or 3 hours (sepsis)
4. IV FLUIDS → 30 mL/kg crystalloid bolus if hypotension or lactate ≥4 mmol/L
5. VASOPRESSORS → Start norepinephrine if MAP <65 despite initial fluids
Mnemonic: LBLAV
- Lactate measure
- Blood cultures
- Launch antibiotics
- Administer fluids
- Vasopressors if needed
FLUID RESUSCITATION
| Phase | Goal | Fluid Choice | Volume |
|---|
| Rescue (0-1h) | Restore perfusion | Crystalloid (Normal Saline or Lactated Ringer's) | 30 mL/kg bolus |
| Optimization (1-6h) | Meet hemodynamic targets | Crystalloid; albumin if large volumes given | Guided by dynamic measures |
| Stabilization (6-24h) | Maintain organ function | Conservative approach; avoid over-resuscitation | Maintain MAP, UO |
| De-escalation (>24h) | Remove excess fluid | Active diuresis if overloaded | Net negative fluid balance |
SSC 2026 key recommendation: For patients with septic shock NOT responding to initial fluids, start vasopressors EARLY rather than giving more fluid. Use balanced crystalloids (Lactated Ringer's) over normal saline to reduce hyperchloremic acidosis and AKI.
Why NOT colloids (HES)? Hydroxyethyl starch (HES) increases risk of AKI and mortality in sepsis - absolutely contraindicated.
VASOPRESSOR PROTOCOL (SSC 2026)
STEP 1: Norepinephrine (NE) → FIRST-LINE
Dose: 0.01-3.3 mcg/kg/min IV infusion
Start at: 0.01-0.05 mcg/kg/min, titrate to MAP ≥65
↓ If MAP still <65 at moderate NE dose:
STEP 2: ADD Vasopressin 0.03-0.04 units/min (fixed dose, do NOT titrate)
- Spares NE dose
- May reduce AKI risk
↓ If still not at goal:
STEP 3: ADD Epinephrine
- Use when cardiac dysfunction coexists
- Increases HR, contractility, AND vasoconstriction
SPECIAL:
Dobutamine → Add to NE if myocardial dysfunction (low CO + evidence of hypoperfusion)
Angiotensin II → Considered for refractory vasodilatory shock
AVOID:
✗ Dopamine as first-line (higher arrhythmia risk vs. NE - SSC 2026)
✗ Phenylephrine in septic shock (decreases CO)
ANTIBIOTIC PROTOCOL
| Situation | Empiric Regimen (First Choice) |
|---|
| Unknown source, community-acquired | Piperacillin-tazobactam 4.5g IV q6h + Vancomycin 25-30 mg/kg IV load |
| Pneumonia (CAP-origin sepsis) | Ceftriaxone 2g IV OD + Azithromycin 500mg IV/PO |
| Urosepsis (community) | Ceftriaxone 2g IV OD (culture first) |
| Hospital-acquired / ICU / MDRO risk | Meropenem 1g IV q8h + Vancomycin (if MRSA risk) |
| Neutropenic sepsis | Piperacillin-tazobactam 4.5g IV q6h or Ceftazidime 2g IV q8h |
| Abdominal source | Piperacillin-tazobactam OR Meropenem + Metronidazole 500mg IV q8h |
| Fungal risk (immunocompromised, prolonged ICU) | Add Fluconazole 400mg IV or Micafungin |
De-escalation principle: Narrow antibiotics based on culture results (SSC 2026). Use PCT trends to guide stopping antibiotics (not starting them).
CORTICOSTEROIDS
Indication: Septic shock requiring ongoing vasopressor therapy despite adequate fluid resuscitation.
- Drug: Hydrocortisone 200 mg/day IV (50 mg q6h OR 200 mg continuous infusion)
- Do NOT use dexamethasone (suppresses HPA axis cortisol testing)
- ACTH stimulation test NOT required before starting
- Duration: Until vasopressors weaned
- Mechanism: Relative adrenal insufficiency in ~50% of septic shock patients; steroid restores vascular responsiveness to catecholamines
BLOOD GLUCOSE MANAGEMENT
| Glucose Level | Action |
|---|
| <140 mg/dL | No insulin needed |
| 140-180 mg/dL | Monitor closely, consider insulin |
| ≥180 mg/dL | Start insulin infusion (SSC 2026 - Strong recommendation) |
| Target range | 140-180 mg/dL (avoid hypoglycemia) |
Never target normoglycemia (<110 mg/dL) - the NICE-SUGAR trial showed increased mortality with tight glucose control.
PART 7 - ESCALATION OF CARE
When to Escalate from Ward to ICU
| Criterion | Action |
|---|
| MAP <65 despite 1-2L fluid | ICU / HDU - vasopressors needed |
| Lactate >4 mmol/L | ICU urgently |
| SpO₂ <90% despite high-flow O₂ | ICU - may need NIV/intubation |
| GCS deterioration | ICU |
| Oliguria <0.5 mL/kg/h for >2h | Escalate |
| SOFA score increasing | Escalate |
| Respiratory rate >30/min | Escalate |
| Hemodynamic instability despite initial bundle | ICU |
Respiratory Escalation Algorithm
Hypoxemia in Sepsis
↓
SpO₂ <94% → Nasal cannula 2-6 L/min
↓ if inadequate
Simple face mask 6-10 L/min
↓ if inadequate
Non-rebreather mask 10-15 L/min
↓ if inadequate
HIGH-FLOW NASAL CANNULA (HFNC) - preferred over NIV (SSC 2026)
Flow: 40-60 L/min | FiO₂ titrated
↓ if SpO₂ <90% or WOB ↑
INTUBATION + MECHANICAL VENTILATION
(Lung-protective: Vt 6 mL/kg IBW, Plateau P <30 cmH₂O)
↓ if refractory (PaO₂/FiO₂ <150)
PRONE POSITIONING (16 hours/day)
NEUROMUSCULAR BLOCKADE
VV-ECMO (tertiary center)
PART 8 - COMPLICATIONS
Early Complications (First 24-72 Hours)
| Complication | Mechanism | Signs | Management |
|---|
| ARDS (7% of sepsis) | Cytokine-mediated alveolar damage, capillary leak | Bilateral infiltrates, PaO₂/FiO₂ <300, hypoxia | Lung-protective ventilation, prone positioning |
| AKI (up to 66%) | Renal hypoperfusion, microvascular injury, nephrotoxins | ↑Cr, oliguria | Optimize MAP, hold NSAIDs/contrast, avoid aminoglycosides |
| DIC | Widespread endothelial activation, thrombin generation | Thrombocytopenia, ↑PT/aPTT, ↓fibrinogen, ↑D-dimer, bleeding | Treat cause; FFP if bleeding; platelets if <50k and bleeding |
| Hepatic dysfunction | Hypoperfusion + direct cytokine injury | ↑bilirubin, ↑transaminases | Supportive; avoid hepatotoxins |
| Septic cardiomyopathy | TNF-α, IL-1 induced myocardial depression | Low CO, low EF on ECHO | Dobutamine; consider epinephrine |
| Lactic acidosis | Anaerobic metabolism + mitochondrial dysfunction | pH <7.35, lactate >4 | Treat underlying sepsis; avoid sodium bicarbonate unless pH <7.1 |
| Adrenal crisis | Relative adrenal insufficiency | Refractory hypotension | Hydrocortisone 200 mg/day |
Late Complications (After Acute Phase)
| Complication | Notes |
|---|
| Post-sepsis syndrome (PICS) | Physical weakness, cognitive impairment, depression - seen in >50% of survivors |
| ICU-acquired weakness (ICUAW) | Muscle atrophy, critical illness polyneuropathy/myopathy |
| Chronic kidney disease | AKI that does not fully recover |
| Psychological PTSD | Especially after prolonged ICU stay |
| Recurrent infections | Immune suppression post-sepsis ("immunoparalysis") |
| Hospital-acquired infections | VAP, CLABSI, CAUTI - from ICU devices |
Prevention of Complications
DIC/Bleeding: Early antibiotics + source control
AKI: Maintain MAP ≥65, avoid nephrotoxins, balanced crystalloids
VAP: Head-of-bed elevation 30-45°, daily sedation holds, early extubation
DVT/PE: Pharmacological VTE prophylaxis (heparin) - SSC 2026 recommends pharmacologic alone
Stress ulcer: Proton pump inhibitor (consider if on mechanical ventilation)
ICUAW: Early physiotherapy, minimize sedation
PART 9 - PROTOCOLS BY SETTING
OPD Protocol (Walk-In Patient with Possible Sepsis)
Patient presents with fever + altered general condition
STEP 1: SCREEN (2 min)
- Check qSOFA: Altered sensorium? RR ≥22? SBP ≤100?
- Temp, HR, BP, SpO₂, RR at triage
STEP 2: TRIAGE DECISION
qSOFA 0-1 + hemodynamically stable:
→ Blood work (CBC, CRP, cultures), urine culture
→ Oral antibiotics if bacterial infection confirmed
→ Return precautions clearly explained
→ Follow-up in 24h
qSOFA ≥2 OR SBP <90 OR any organ dysfunction:
→ DO NOT discharge → Call ambulance / transfer to ED immediately
→ IV access en route
→ O₂ supplementation
⚠️ SAFETY RULE: Never send a septic patient home with oral antibiotics if they have
evidence of organ dysfunction. This requires hospital admission.
Ward Protocol (Admitted Patient Developing Sepsis)
Ward patient → Nurse notices: fever spike + tachycardia + confusion
STEP 1: RAPID ASSESSMENT (0-15 min)
→ Vital signs Q15 min
→ GCS, urine output check
→ IV access (large bore ×2)
→ O₂ via face mask, SpO₂ monitor
STEP 2: INVESTIGATIONS (simultaneous)
→ Blood cultures ×2 (BEFORE antibiotics)
→ CBC, metabolic panel, lactate, coagulation
→ CXR (portable)
→ Urinalysis + culture
→ ECG
STEP 3: CALL DOCTOR + IMPLEMENT
→ Notify registrar/consultant IMMEDIATELY
→ 30 mL/kg crystalloid bolus over 30-60 min (if not contraindicated)
→ Broad-spectrum antibiotics WITHIN 1 HOUR
→ Catheterize (urine output monitoring)
STEP 4: REASSESS (1h mark)
→ MAP <65 despite fluids → Transfer to HDU/ICU, start vasopressors
→ Lactate not clearing → ICU
→ SpO₂ <90% → Escalate O₂, ICU referral
→ Response to treatment → Continue ward management with close monitoring
ICU Protocol (Septic Shock Patient)
ICU ADMISSION CHECKLIST:
□ Arterial line (continuous BP + ABG access)
□ Central venous catheter (CVC) - right internal jugular or subclavian
□ Foley catheter (hourly urine output)
□ NGT (nutrition)
□ Continuous ECG + SpO₂
□ Point-of-care ECHO (assess volume status, LV function)
BUNDLE COMPLIANCE AUDIT (Hour 1):
□ Lactate measured?
□ Blood cultures × 2 drawn?
□ Broad-spectrum antibiotics given?
□ 30 mL/kg fluid given?
□ Vasopressors started if MAP <65?
ONGOING ICU MANAGEMENT:
□ Vasopressor titration to MAP ≥65
□ Lactate q2h until <2 mmol/L
□ Glucose monitoring q1-2h (target 140-180 mg/dL)
□ Electrolyte correction (K⁺, Mg²⁺, Ca²⁺, PO₄)
□ Lung-protective ventilation if intubated (Vt 6 mL/kg IBW)
□ Daily sedation hold + SAT/SBT protocol
□ VTE prophylaxis (heparin 5000 U SC q8-12h)
□ Stress ulcer prophylaxis (PPI)
□ Early enteral nutrition (within 24-48h, SSC 2026: within 72h)
□ Daily SOFA score recalculation
□ Antibiotic de-escalation based on cultures + PCT trend
□ Source control (drain abscess, remove infected catheter)
Emergency Protocol (ED Presentation)
CODE SEPSIS - Activation Criteria:
Suspected infection + ≥2 of: Temp >38.3 or <36°C | HR >90 | RR >20 | Altered sensorium
TIME ZERO (Recognition):
0 min: Two large-bore IVs | O₂ | Monitor | Glucose check
5 min: Blood cultures ×2 | Lactate | CBC | CMP | Coag
15 min: CXR (portable) | ECG | UA | IV fluids RUNNING
30 min: Antibiotics IN (don't wait for culture results)
60 min: Reassess MAP + lactate
↓ If MAP <65 → Vasopressors (NE via CVC or peripheral large bore)
↓ If SpO₂ <90% → HFNC or NIV
↓ If GCS declining → RSI + intubation
DOCUMENTATION: Time of recognition, time of antibiotics, time of cultures,
fluid volumes, vasopressor start time (medicolegal and audit purposes)
PART 10 - GUIDELINES & SOURCES
| Guideline | Year | Key Points |
|---|
| Surviving Sepsis Campaign (SSC) 2026 | March 2026 | 129 recommendations; 46 new statements; emphasizes early vasopressors, balanced crystalloids, antibiotic stewardship, post-ICU care |
| SSC 2021 | Oct 2021 | Hour-1 bundle; HFNC preferred over NIV; restrictive RBC transfusion |
| Sepsis-3 Consensus | 2016 | SOFA-based definitions, removed SIRS criteria |
| NICE-SUGAR Trial | 2009 | No tight glucose control; target 140-180 mg/dL |
| PROCESS / ARISE / ProMISe Trials | 2014-2015 | EGDT not superior to usual care; simplified bundle |
| SMART Trial | 2018 | Balanced crystalloids (LR) reduce AKI vs NS |
| VASST Trial | 2008 | Vasopressin as NE-sparing agent in moderate shock |
| APROCCHSS Trial | 2018 | Hydrocortisone + fludrocortisone reduce mortality in septic shock |
| REMAP-CAP | Ongoing | Platform trial addressing multiple sepsis interventions |
PART 11 - CLINICAL PEARLS FOR EXAMS & VIVA
High-Yield MBBS Exam Points
- Sepsis-3 definition: Sepsis = infection + SOFA ≥2; Septic shock = sepsis + vasopressor + lactate >2 despite fluids
- Most common source: Urinary tract (48.9%) followed by respiratory (32.9%)
- Most common organisms: Gram+ = S. aureus, Streptococcus; Gram- = E. coli, Klebsiella, Pseudomonas
- First-line vasopressor: Norepinephrine (NOT dopamine - SSC 2026)
- Fluid of choice: Balanced crystalloid (Lactated Ringer's > Normal Saline)
- NEVER give HES (hydroxyethyl starch) - increases mortality
- Glucose target: 140-180 mg/dL (not normal range - NICE-SUGAR)
- Corticosteroids: Only if vasopressor-dependent; Hydrocortisone 200 mg/day
- Antibiotics: WITHIN 1 hour in septic shock; don't wait for culture results
- Septic shock mortality: ~40-50% despite treatment
Common Student Mistakes
| Mistake | Correct Approach |
|---|
| Waiting for cultures before giving antibiotics | Cultures take 5 min to draw, then start antibiotics immediately |
| Using dopamine as first vasopressor | Norepinephrine is first-line (dopamine has higher arrhythmia risk) |
| Targeting tight glucose control | Target 140-180, not <110 |
| Giving HES/colloid | Only crystalloids (and albumin in specific situations) |
| Using CVP alone to guide fluids | Use dynamic measures (PLR, PPV, IVC US) |
| Stopping antibiotics when fever resolves | Use PCT trend + clinical improvement for de-escalation |
| Not doing blood cultures before antibiotics | Always cultures first (takes only minutes) |
| Not doing source control | Remove infected catheters, drain abscesses |
Frequently Asked Viva Questions
-
"What is the difference between Sepsis-2 and Sepsis-3?"
- Sepsis-2 used SIRS criteria (too non-specific). Sepsis-3 uses SOFA score (organ dysfunction focused) and eliminated "severe sepsis" as a term.
-
"Why is lactate important in sepsis?"
- Lactate >2 mmol/L = tissue hypoperfusion; Lactate >4 = very high mortality. Used for diagnosis of septic shock (even with normal BP) and as a resuscitation endpoint (target clearance). Limitation: liver/kidney failure can impair clearance.
-
"What is qSOFA and when do you use it?"
- Quick bedside screen (no labs): altered sensorium + RR ≥22 + SBP ≤100. Score ≥2 = high risk. Use in wards/ED triage, not in ICU.
-
"Why not use dopamine in septic shock?"
- Higher risk of atrial fibrillation and arrhythmias vs. norepinephrine. A 2012 meta-analysis showed dopamine associated with higher 28-day mortality. NE is cleaner, predictable, and preferred.
-
"What is relative adrenal insufficiency?"
- In septic shock, the adrenal glands may produce insufficient cortisol for the degree of stress, even if absolute cortisol levels are "normal." Results in catecholamine-refractory vasodilation. Treated with hydrocortisone.
PART 12 - CASE-BASED LEARNING
I'll ask you to work through these - respond with your answers and I'll guide you:
CASE 1 - OPD Scenario
A 65-year-old man with Type 2 Diabetes comes to your OPD with 2 days of burning micturition, fever (38.8°C), chills, and since this morning he has been "confused." His wife says he is "not himself." He has no prior cardiac or renal disease.
Vitals: BP 88/54 mmHg | HR 118/min | RR 24/min | Temp 38.8°C | SpO₂ 95% on room air | Random glucose 234 mg/dL
Questions for you to answer:
- Calculate his qSOFA score. What does it mean?
- What is the most likely source of sepsis?
- What is your IMMEDIATE next step in this OPD?
- What investigations would you order?
- Would you discharge him on oral antibiotics? Why or why not?
CASE 2 - Ward Scenario
A 52-year-old woman admitted 3 days ago for elective cholecystectomy. Post-op Day 2, the nurse calls you at 2 AM: "Doctor, she has a fever of 39.2°C, her BP dropped to 96/60, heart rate 108, and she seems drowsy."
Questions:
- What are your first three actions in the next 5 minutes?
- What sepsis criteria does she meet?
- What is the most likely source?
- Write the antibiotic order for her.
- When do you call for ICU transfer?
CASE 3 - ICU Scenario
A 70-year-old man is in your ICU on Day 3 of septic shock from pneumonia. He is on:
- Norepinephrine 0.25 mcg/kg/min
- Ventilator (assist control, Vt 420 mL, IBW 70 kg, FiO₂ 0.6, PEEP 8)
- Current vitals: MAP 62, HR 104, SpO₂ 91%, urine output 18 mL in last hour
- Labs: K⁺ 3.1 mEq/L, Creatinine 2.8 (baseline 1.0), Lactate 3.8, Glucose 220 mg/dL, Platelets 62,000
Questions:
- Is he meeting hemodynamic goals? What is not at target?
- What is his approximate SOFA score for the renal component?
- What would you do about his potassium?
- What changes would you make to his ventilator?
- He develops petechiae and oozing from IV sites. What complication do you suspect and how do you confirm it?
PART 13 - VISUAL SUMMARY (MIND MAP)
SEPSIS & SEPTIC SHOCK
│
┌──────────────────────┼──────────────────────┐
│ │ │
DEFINITION DIAGNOSIS MANAGEMENT
Sepsis-3: qSOFA ≥2 LBLAV Bundle
SOFA ≥2 + SOFA ≥2 (Hour-1)
infection Lactate │
│ Blood cx ├─ Fluids: LR 30mL/kg
Septic Shock: POCUS ├─ Antibiotics <1h
+vasopressors + ├─ NE vasopressor
lactate >2 ├─ Source control
│ └─ Steroids if needed
│
COMPLICATIONS
├─ Early: ARDS, AKI, DIC, Septic cardiomyopathy
└─ Late: PICS, ICUAW, CKD, PTSD
│
MONITORING
├─ MAP ≥65, UO ≥0.5 mL/kg/h
├─ Lactate clearance
├─ ScvO₂ ≥70%
└─ SOFA daily
SAFETY DISCLAIMER
Educational Use Only. This content is for learning purposes. All clinical decisions - including antibiotic selection, vasopressor dosing, fluid management, and ICU admission - must be made by a qualified, licensed physician with full knowledge of the patient's clinical status. Drug doses given are standard references; always verify against current formularies and local protocols before prescribing.
Ready for Case-Based Learning? Reply with your answers to Case 1 (the OPD scenario) and I'll provide feedback, guide your reasoning, and progressively reveal the management. Or tell me which specific section you'd like me to go deeper on - electrolytes, mechanical ventilation, DIC management, or any other aspect.