Aortic stenosis
Reading File
Finding Sources
Searching PubMed
"aortic stenosis"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Here is a thorough overview of aortic stenosis (AS) synthesized from Braunwald's Heart Disease, Fuster & Hurst's The Heart, Grainger & Allison's Diagnostic Radiology, and other authoritative textbooks.
Aortic Stenosis
Epidemiology
AS is the most common valvular heart disease in developed countries. It is present in approximately 15% of adults aged 65 and older, with severe AS (valve area <1 cm²) in ~2% of that group. Prevalence rises to 3% in patients aged 75 and above. - Braunwald's Heart Disease; Symptom to Diagnosis
Etiology
| Cause | Key Features |
|---|---|
| Degenerative calcification (most common) | Progressive calcification of a trileaflet valve; patients typically >65 years |
| Congenital bicuspid aortic valve | Affects 1-2% of the population; severe AS develops in 66% of these patients, presenting 1-2 decades earlier than tricuspid disease; often associated with aortic root dilation that can require repair |
| Rheumatic heart disease | Now rare in developed countries |
- Symptom to Diagnosis, 4th ed.; Braunwald's Heart Disease
Pathophysiology
The mechanical obstruction to LV ejection triggers a cascade of compensatory and then maladaptive changes:
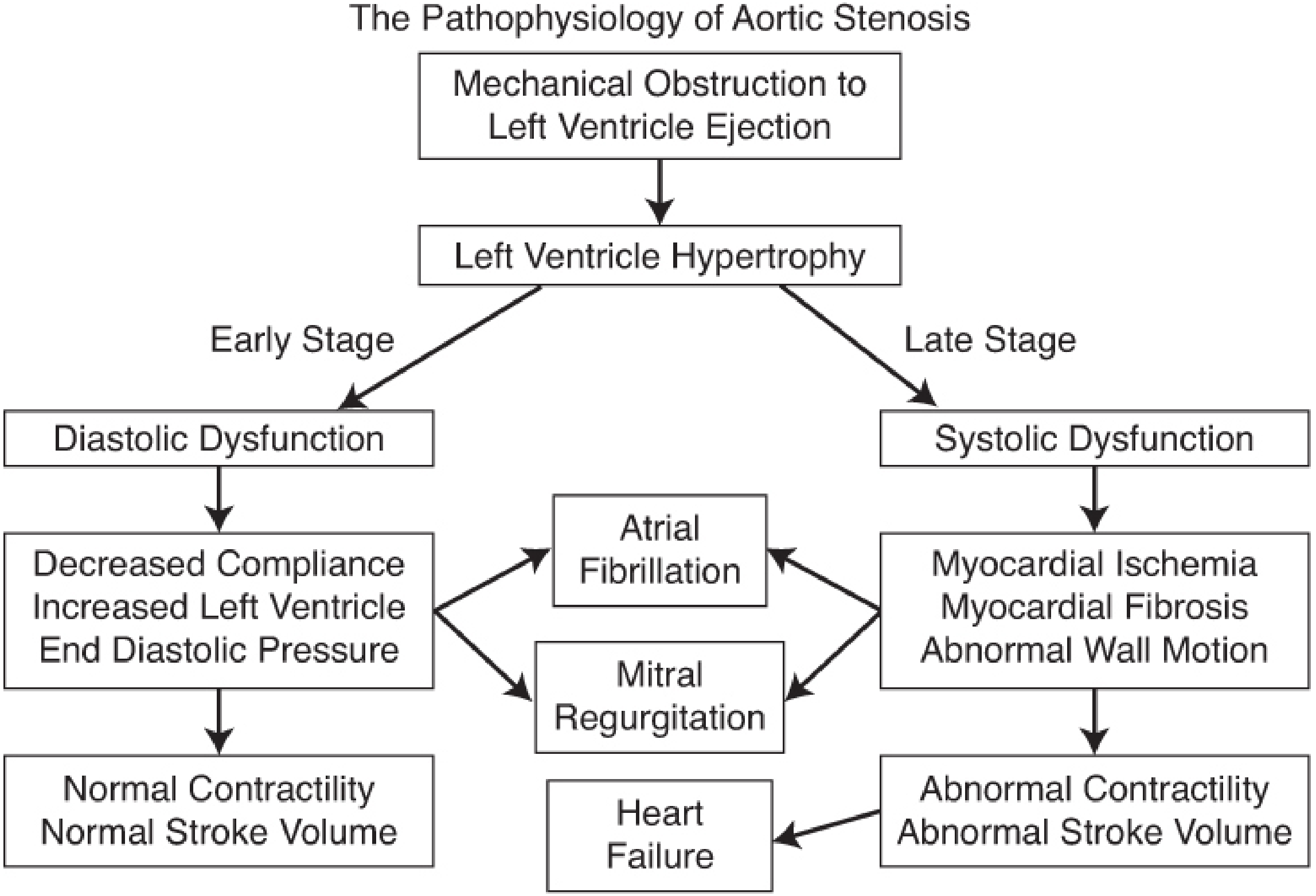
Figure: The Pathophysiology of Aortic Stenosis - Barash Clinical Anesthesia, 9e
- The LV responds to chronic pressure overload by developing concentric hypertrophy, maintaining stroke volume at the cost of increased wall stress and myocardial oxygen demand
- Early stage: Diastolic dysfunction - decreased LV compliance, elevated end-diastolic pressure, but normal contractility and stroke volume
- Late stage: Systolic dysfunction - myocardial ischemia, fibrosis, abnormal wall motion, reduced contractility, ultimately leading to heart failure
- Atrial fibrillation is poorly tolerated because the hypertrophied, noncompliant LV is heavily dependent on the atrial "kick" for filling
- Abnormal shear stress across the stenotic valve disrupts large von Willebrand multimers, causing an acquired bleeding tendency (Heyde syndrome)
Clinical Presentation: The Classic Triad
| Symptom | Mechanism | Prognosis Without AVR |
|---|---|---|
| Angina | Increased O₂ demand + subendocardial ischemia | 50% 5-year mortality |
| Syncope | Exertional vasodilation against fixed cardiac output | 50% 3-year mortality |
| Dyspnea / Heart failure | Elevated LV filling pressures | 50% 2-year mortality |
The most common early symptoms are decreased exercise tolerance and exertional dyspnea. In older, sedentary individuals these may not be reported until late. - Symptom to Diagnosis, 4th ed.
Physical Examination
- Murmur: Harsh, late-peaking crescendo-decrescendo systolic ejection murmur, best heard at the right upper sternal border, radiating to the right carotid (sensitivity 71-73%)
- Carotid upstroke: Slow, sustained (pulsus parvus et tardus) - sensitivity 15-42%, specificity 95-100%, LR+ 9.2
- Note: In older adults with stiff, atherosclerotic vessels, the carotid delay may be absent despite severe AS
- S2: Diminished or absent A2 (calcification limits leaflet motion)
- S4 gallop: Common, reflecting decreased LV compliance
Severity Grading (Doppler Echocardiography)
| Parameter | Mild | Moderate | Severe |
|---|---|---|---|
| Peak velocity (m/s) | 2.0-2.9 | 3.0-3.9 | ≥4.0 |
| Mean gradient (mm Hg) | <20 | 20-39 | ≥40 |
| Valve area (cm²) | >1.5 | 1.0-1.5 | <1.0 |
| Indexed valve area (cm²/m²) | - | - | <0.6 |
Low-Flow, Low-Gradient AS
Over 40% of older patients have lower-than-expected gradients. Two patterns exist:
- Low-flow, low-gradient with reduced LVEF (Stage D2): True severe AS with LV dysfunction - AVR is beneficial
- Low-flow, low-gradient with preserved LVEF (Stage D3): Common in women with small LV cavities and in AF
- Paradoxical high-flow, low-gradient: This subset does NOT generally benefit from AVR
- Braunwald's Heart Disease
Investigations
Chest X-ray:
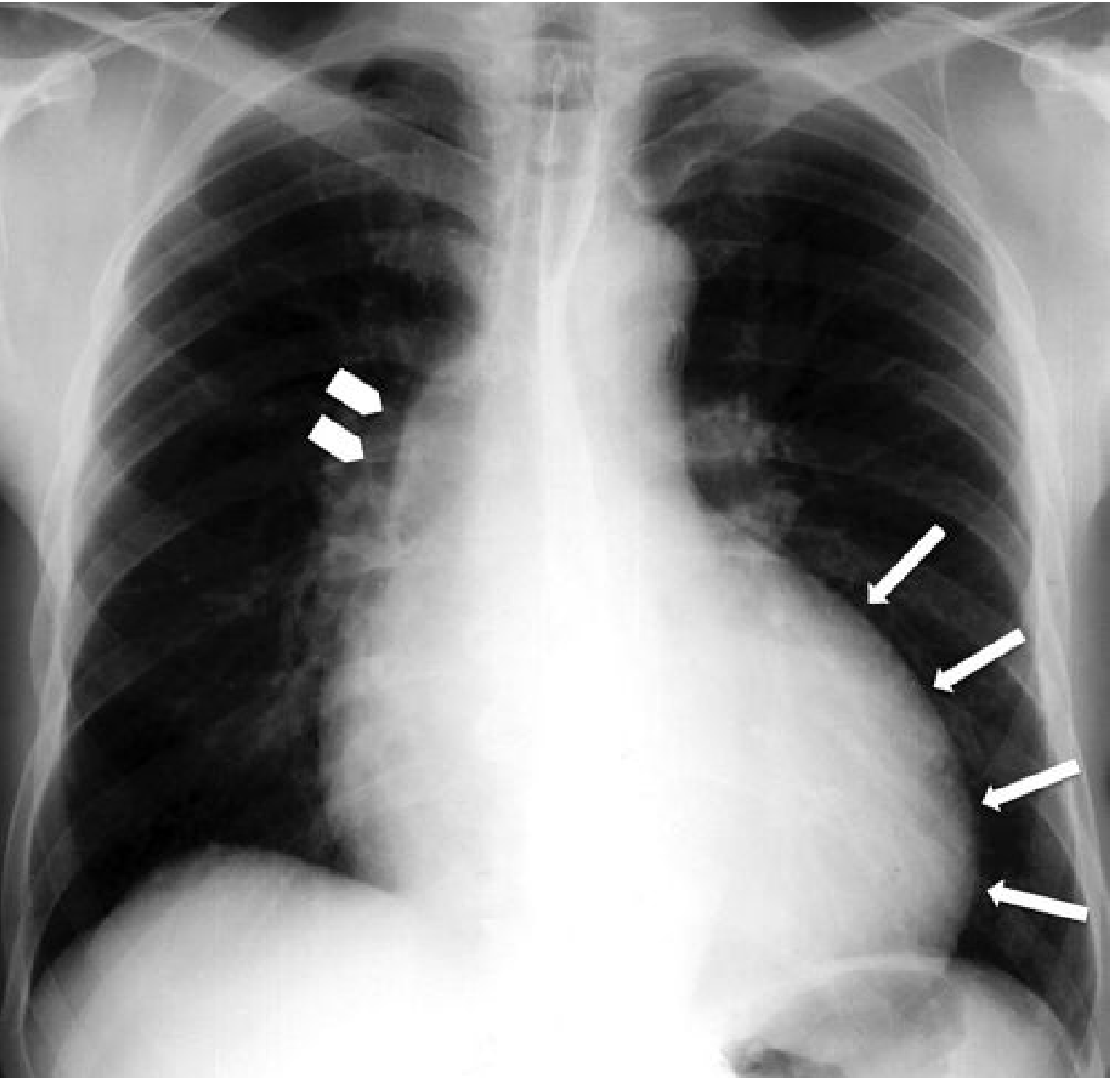 CXR: Rounded left ventricular profile (arrows) with post-stenotic dilation of the ascending aorta (arrowheads) - Grainger & Allison's Diagnostic Radiology
CXR: Rounded left ventricular profile (arrows) with post-stenotic dilation of the ascending aorta (arrowheads) - Grainger & Allison's Diagnostic Radiology
- ECG: LV hypertrophy pattern
- Echocardiography (TTE - first-line): Assess valve morphology, calcification, leaflet motion; Doppler for peak velocity, mean gradient, and valve area via the continuity equation (EOA = SV × VTI_LVOT/VTI_AV)
- CT: Agatston calcium scoring (score ≥1600 in men, ≥800 in women correlates with severe AS); direct planimetry of the orifice area; also evaluates aortic root dimensions before TAVR
- CMR: Assesses LV function and mass, valve morphology; less sensitive than CT for calcium detection but accurate for planimetric orifice area
- Exercise stress testing: Can unmask symptoms in apparently asymptomatic severe AS; triggers for intervention include exercise-induced symptoms, reduced exercise tolerance, or a fall in blood pressure
Management
Medical Therapy
There is no proven pharmacological therapy that alters the natural history of AS. No drug has been shown to slow progression. Management of comorbidities (hypertension, dyslipidemia) is appropriate, but ACE inhibitors and nitrates must be used cautiously to avoid precipitous drops in preload or afterload. - Fuster & Hurst's The Heart, 15th ed.
Indications for Aortic Valve Replacement (ACC/AHA 2020 Guidelines)
| Indication | Class |
|---|---|
| Symptomatic severe high-gradient AS (Stage D1) | Class I |
| Asymptomatic severe AS with LVEF <50% | Class I |
| Severe AS undergoing other cardiac surgery | Class I |
| Symptoms unmasked by exercise testing | Class I or IIa |
| Symptomatic low-flow, low-gradient AS (Stage D2/D3) if severity confirmed | Class IIa |
| Asymptomatic very severe AS (peak velocity ≥5 m/s) | Class IIa |
Surgical AVR (SAVR)
- Standard approach for younger, lower-risk patients and those requiring concomitant procedures (e.g., CABG, aortic root repair for bicuspid valve disease)
- Tissue (bioprosthetic) valves preferred in older individuals to avoid lifelong anticoagulation; degenerate more slowly in the elderly, often lasting the patient's remaining lifespan
- For patients aged 65-80: shared decision-making between SAVR and TAVR is recommended
Transcatheter AVR (TAVR)
TAVR has transformed the management of AS, particularly in older and higher-risk patients:
- FDA approved in the US since 2011
- Originally for inoperable patients (PARTNER trial: 1-year mortality 30% with TAVR vs. 50% with medical therapy)
- Subsequently shown non-inferior to SAVR in high- and intermediate-risk patients
- In low-risk patients (mean age 73): composite of death, stroke, or hospitalization at 1 year was 8.5% (TAVR) vs. 15.1% (SAVR) - significantly better
- TAVR-specific risks: stroke, vascular complications, permanent pacemaker requirement (higher than SAVR), paravalvular leak - all rates have declined with newer-generation devices
- 30-day mortality after TAVR has declined from 4% to 3% (2013-2015 data), with ongoing improvements
- Balloon aortic valvuloplasty is used as a bridge to definitive intervention (effects last only weeks to months) or in pregnancy
Anesthetic/Hemodynamic Goals (Perioperative)
| Parameter | Goal | Rationale |
|---|---|---|
| Preload | Maintain or increase | LV is preload-dependent |
| Afterload | Maintain or increase | Preserve coronary perfusion gradient |
| Heart rate | Normal sinus rhythm, avoid tachycardia and bradycardia | Fixed stroke volume means CO depends on HR |
| Contractility | Maintain | May be reduced in late-stage disease |
Avoid hypotension at all costs - the hypertrophied LV depends on diastolic pressure to perfuse subendocardium. - Barash Clinical Anesthesia, 9e
AS in Special Populations
Pregnancy: Severe AS is high risk in pregnancy (increased circulatory demand may precipitate pulmonary edema or syncope). Balloon valvuloplasty can be used as a bridge; TAVR is emerging but not yet standard. - Creasy & Resnik's Maternal-Fetal Medicine
Elderly/Frail: TAVR has expanded treatment options dramatically. Outcomes are primarily determined by frailty and comorbidities rather than age alone.
Black patients: TAVR experience has been disparate in Black patients with critical AS, with evidence of underutilization despite eligibility. - Fuster & Hurst's The Heart, 15th ed.
Sources: Braunwald's Heart Disease (10e), Fuster & Hurst's The Heart (15e), Grainger & Allison's Diagnostic Radiology, Symptom to Diagnosis (4e), Barash Clinical Anesthesia (9e), Creasy & Resnik's Maternal-Fetal Medicine, Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.