Thyroid eye disease ophthalmology
Reading File
Finding Sources
Finding Sources
Searching PubMed
"thyroid eye disease" AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive material to write a detailed, well-structured answer. Here is the full clinical review:
Thyroid Eye Disease (TED) - Ophthalmology
TED, also known as thyroid-associated orbitopathy or Graves ophthalmopathy, is the most common cause of both unilateral and bilateral proptosis in adults. It is an autoimmune orbitopathy most closely linked to Graves disease, though it can occur in euthyroid (5-10%) and hypothyroid patients (5-10%).
Clinical Appearance

Epidemiology & Risk Factors
- Female predominance (5:1), peak in 4th-5th decades
- Smoking is the major modifiable risk factor - risk is dose-dependent and cessation reduces it
- Radioactive iodine (RAI) treatment for hyperthyroidism can worsen TED; concurrent oral steroids mitigate this
- Family history of thyroid dysfunction is common
- Vitamin D deficiency increases risk of progressive orbitopathy
- Kanski's Clinical Ophthalmology 10th, p. 132-133
Pathogenesis
Anti-thyrotropin-receptor (TSH-R) antibodies react against both thyroid gland cells and orbital fibroblasts. IGF-1R and TSHR are upregulated in orbital and brow fat. The resulting cascade:
- Pleomorphic cellular infiltration (T-cells, mast cells, macrophages)
- Increased glycosaminoglycan secretion → osmotic water imbibition
- Extraocular muscles swell up to 8x normal size
- Lipogenesis by fibroblasts/preadipocytes → orbital fat expansion
- Raised intraorbital pressure → possible optic nerve compression
- Eventual muscle fiber degeneration → fibrosis → restrictive myopathy
- Kanski's Clinical Ophthalmology 10th, p. 133
Disease Course
TED passes through two phases:
| Phase | Description | Timeline |
|---|---|---|
| Congestive (inflammatory) | Red, painful, active inflammation | Remits in 1-3 years |
| Fibrotic (quiescent) | White, quiet eye; painless motility defect may persist | Permanent sequelae |
Only ~10% of patients develop serious long-term ocular problems.
Clinical Features
1. Soft Tissue Involvement
- Grittiness, redness, lacrimation, photophobia, retrobulbar discomfort
- Epibulbar hyperaemia over horizontal rectus insertions (sensitive activity marker)
- Periorbital swelling, chemosis, fat prolapse into lids
- Tear insufficiency, superior limbic keratoconjunctivitis (SLK)
2. Eyelid Retraction (present in ~50%)
- Upper lid retraction with lateral flare - highly specific for TED
- Von Graefe sign - lid lag on downward gaze
- Lagophthalmos leading to exposure keratopathy
- Mechanism: Muller muscle sympathetic overstimulation + levator/inferior rectus fibrosis
3. Proptosis
- Usually axial (bilateral or unilateral/asymmetric)
- Myogenic variant: prominent muscle enlargement, minimal proptosis, apical crowding on CT
- Lipogenic variant: severe proptosis, increased fat volume, minimal muscle involvement
4. Restrictive Myopathy
- EOM involvement frequency: Inferior > Medial > Superior > Lateral rectus (mnemonic: "I'M SLow")
- Typically muscle belly enlargement with tendon sparing (distinguishes TED from orbital myositis)
- Elevation and abduction most commonly restricted
- Positive forced duction test
5. Compressive Optic Neuropathy (CON)
Occurs in 5-7% of TED patients - must be excluded at every visit.
Key features:
- Reduced VA (not always), colour desaturation (sensitive early sign), diminished brightness appreciation
- Relative afferent pupillary defect (RAPD) - "gives cause for marked concern"
- Visual field defects (central/paracentral, nerve fibre bundle)
- Optic disc: normal, swollen, or atrophic
- Critically, axial proptosis is often absent or mild in CON - apical crowding by enlarged muscles is the cause
- VEPs useful when diagnosis uncertain
- Kanski's Clinical Ophthalmology 10th, p. 135-136; Wills Eye Manual, p. 424
Systemic Associations
- Hyperthyroidism in ≥80% (TFTs may be normal; euthyroid patients need 6-12 monthly TFTs)
- TED can precede, coincide with, or follow thyroid dysfunction by months to years
- May co-exist with myasthenia gravis - ptosis (rather than retraction) or adduction deficit should raise this possibility
EUGOGO Classification (2021)
Activity (Clinical Activity Score - CAS): 1 point each for:
- Spontaneous retrobulbar pain
- Pain on attempted up/down gaze
- Redness of eyelids
- Redness of conjunctiva
- Conjunctival/plical swelling (chemosis)
- Swelling of eyelids
Score ≥3/7 = active disease warranting immunosuppression.
Severity:
| Grade | Description |
|---|---|
| Mild | Minor impact on daily life |
| Moderate-severe | ≥2mm lid retraction, ≥3mm proptosis, moderate-severe soft tissue involvement, diplopia |
| Sight-threatening | Compressive optic neuropathy or corneal breakdown |
Investigation
- Thyroid function tests (TSH, T3, T4) - may be normal; TSI and TPO antibodies can guide diagnosis and treatment
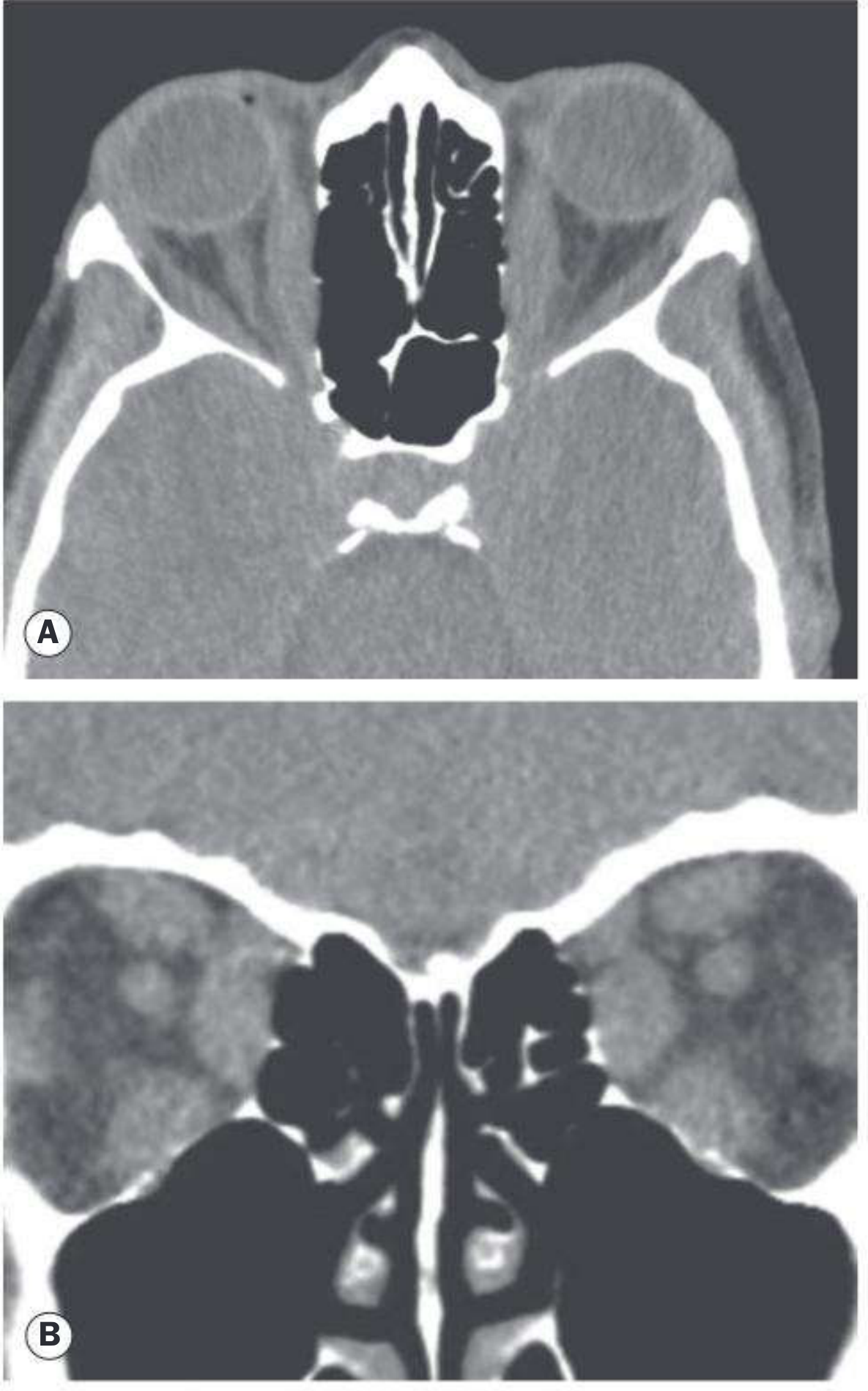
- Orbital CT (axial + coronal, without contrast) - indicated for: atypical presentation, unilateral proptosis, severe congestive orbitopathy, optic neuropathy, pre-surgical planning
- Classic finding: fusiform muscle belly enlargement with tendon sparing
- Automated visual fields + OCT - screen for subclinical optic neuropathy
- Colour vision testing / RAPD - at every visit for CON surveillance
- Serum vitamin D level
- MRI: superior soft-tissue resolution; preferred in children (no radiation)
CT Appearance in TED
Treatment
Step 1: All Patients - General Measures
- Smoking cessation - mandatory first step
- Adequate control of thyroid dysfunction (with steroid cover if RAI is used)
- Lubricants, topical anti-inflammatories for ocular surface
- Head elevation at night (3 pillows) to reduce periorbital edema
- Lid taping at night for exposure keratopathy
Mild Active Disease
- Lubricants, topical ciclosporin/NSAIDs
- Selenium 200 µg/day for 6 months (in selenium-deficient areas; reduces progression of mild-moderate TED; use with caution in males due to possible prostate cancer risk)
- Vitamin D supplementation if deficient
Moderate-Severe Active Disease
- IV methylprednisolone (preferred over oral): 500 mg weekly x 6 weeks → 250 mg weekly x 6 weeks (max cumulative dose <8 g to protect liver)
- IV methylprednisolone + mycophenolate sodium (0.72 g/day x 24 weeks) = superior to steroids alone; regimen of choice in specialist centres
- Low-dose orbital radiotherapy: 20 Gy in 10-14 fractions over 2 weeks
- Second-line; reduces restrictive strabismus progression; ~40% non-responders
- Avoid or use cautiously in diabetics and vasculopaths (radiation retinopathy risk)
- Contraindicated in patients <35 years old
Sight-Threatening TED (Optic Neuropathy)
- Immediate pulsed IV methylprednisolone: 0.5-1 g on 3 successive days, converted to oral
- If steroids ineffective (20%) or contraindicated → orbital decompression surgery
- Posterior orbital/apex decompression is most effective for optic neuropathy
Biologics (Second-line / Corticosteroid-Resistant Disease)
| Agent | Target | Notes |
|---|---|---|
| Teprotumumab | IGF-1R | FDA-approved Jan 2020; reduces proptosis and CAS in both active and chronic TED; effective for optic neuropathy in small series; hearing loss is a side effect |
| Rituximab | CD20 (B-cells) | Off-label; some evidence |
| Tocilizumab | IL-6 receptor | Off-label; emerging evidence |
Recent 2025 meta-analyses confirm teprotumumab's efficacy (PMID 39952471) and tocilizumab's safety profile (PMID 40304985) in TED.
Surgical Algorithm (Post-Inflammatory Phase Only)
Must follow strict sequence to avoid unpredictable results:
- Orbital decompression (if needed)
- Strabismus surgery (for significant diplopia)
- Eyelid surgery (retraction repair, blepharoplasty)
Orbital decompression options:
| Approach | Proptosis Reduction | Notes |
|---|---|---|
| 1-wall (deep lateral) | 4-5 mm | Lowest diplopia risk |
| 2-wall (balanced medial + lateral) | Greater | Significant new diplopia risk |
| 3-wall (includes floor) | 6-10 mm | Risk of hypoglobus, infraorbital nerve damage |
| 4-wall (+ roof) | Reserved for severe cases |
Indications for decompression: compressive optic neuropathy, severe exposure keratopathy, globe luxation, uncontrollable IOP elevation, morbid proptosis.
- Kanski's Clinical Ophthalmology 10th, p. 136-138; Wills Eye Manual, p. 427-430
Differential Diagnosis of Eyelid Retraction
- Previous lid surgery/trauma
- Contralateral severe ptosis (Hering's law)
- Oculomotor nerve palsy with aberrant regeneration (pseudo-von Graefe sign)
- Parinaud syndrome - dorsal midbrain; lid retraction (Collier sign) + upgaze palsy + convergence-retraction nystagmus + light-near dissociation
Differential Diagnosis of Orbital Myositis vs TED EOM Enlargement
| Feature | TED | Orbital Myositis |
|---|---|---|
| Tendon involvement | Spared | Involved |
| Onset | Gradual | Rapid, painful |
| Laterality | Often bilateral | Usually unilateral |
| Response to steroids | Partial | Dramatic |
Key Points Summary
- TED is the most common cause of proptosis in adults
- The EOM order of involvement: Inferior > Medial > Superior > Lateral (tendon sparing)
- CON occurs in 5-7% but must be excluded at every visit; color vision loss is an early sensitive sign
- Treatment decisions depend on: activity (CAS), severity (EUGOGO), and disease duration (immunosuppression is much less effective after 18 months)
- Teprotumumab (anti-IGF-1R) is the first FDA-approved biologic for TED (2020)
- Surgical sequence is fixed: decompression → strabismus → eyelid
This is a shared conversation. Sign in to Orris to start your own chat.