Question - arsh (hemorrhoids) a- treatment/ instument b pre / procedure/ post
In Kashyap samhita, khila sthan
Tell me the taila,ghruta, dhomra Varna of stanya shloka and refrence
Kashyapa Samhita Khila Sthana stanya varna taila ghrita dhuma shloka
Kashyapa Samhita Khilasthana stanya pariksha taila ghrita dhoomra varna shloka reference
https://ijprajournal.com/issue_dcp/A%20Review%20Contribution…
Kashyapa Samhita Khila sthana stanya adhyaya chapter taila varna bala ghrita varna dhana dhuma khyati shloka
Kashyapa Samhita - Khila Sthana: Stanya Varna (Taila, Ghrita, Dhuma)
Context
Stanya Varna - Shloka and Meaning
| Varna (Color/Appearance) | Appearance of Stanya | Effect on Child (Phala) |
|---|---|---|
| Taila Varna | Color like oil (Taila-like, slightly yellowish/oily appearance) | Imparts Bala (strength and physical power) to the baby |
| Ghrita Varna | Color like ghee (clear, pale yellow, ghee-like) | Child becomes Dhanadhya / Dhanavan (very wealthy/prosperous) |
| Dhuma / Dhomra Varna | Smoky, grayish or dusky color | Child attains Khyati / Yashas (fame, renown, glory) |
| Shankha Varna (pure/normal) | White like a conch shell (Shankha-abha) | Imparts Sarvagunasampanna - all positive qualities; is the ideal, normal stanya |
| Madhura / Swadu Stanya | (by rasa, not varna) Sweet milk | Increases frequency of stool and urine (normal digestive activity) |
Shloka (as described in the text):
"Tailavarnam balam dadyat ghritavarnam dhanapradam | Dhumavarnam yashasvinyam shuddham sarvagunottaram ||"
- Taila-varnam = milk that resembles the color of oil
- Balam dadyat = gives strength (Bala) to the child
- Ghrita-varnam = milk resembling the color of ghee
- Dhana-pradam = bestows wealth/prosperity
- Dhuma-varnam = milk of smoky color
- Yashasvinam = makes the child famous/glorious
- Shuddham = pure/white milk (Shankha-abha)
- Sarva-guna-uttaram = best in all qualities
Reference
Kashyapa Samhita (Vriddha Jivakiya Tantra) Khila Sthana - Ksheerguna Vigyaniya Adhyaya
- Ed. Shri Satyapal Bhishagacharya with Hindi commentary Vidyotini, Reprint Edition, Chaukhamba Sanskrit Series, Varanasi
- Khila Sthana, Chapter (Ksheerguna vigyaniya)/22 - p. 355
- Also cited as: Khila Sthana 22/355 (Satyapal edition)
P.V. Tewari edition (English translation):
- Acharya Kashyapa, Kashyapa Samhita or Vrddhajivakiya Tantra, Text with English Translation and commentary, Chowkhambha Vishvabharati, Varanasi, Reprint 2018
Clinical (Ayurvedic) Significance
- Taila Varna stanya indicates Kapha-dominant, nourishing milk - good for physical growth
- Ghrita Varna stanya is considered ideal and sattvic in quality
- Dhuma Varna stanya may indicate mild Pitta-Vata derangement but is not pathological; it is considered a positive variation
- Shankha-abha (pure white) stanya is the gold standard of healthy breast milk per Kashyapa
Formula milk brand
🍼 Infant Formula Milk Brands
Stage 1 (0–6 months)
| Brand | Company | Key Feature |
|---|---|---|
| Nan Pro 1 | Nestlé | With Bifidus BL + Probiotics |
| Similac Advance | Abbott | No palm olein oil, DHA/ARA |
| Enfamil A+ | Mead Johnson (Reckitt) | MFGM + DHA |
| Aptamil 1 | Danone (Nutricia) | LCP + Prebiotics |
| Farex 1 | Heinz (Zydus) | Iron fortified |
| Lactogen 1 | Nestlé (India) | Probiotic L.reuteri |
Stage 2 (6–12 months)
| Brand | Stage | Note |
|---|---|---|
| Nan Pro 2 | Follow-on | For weaning period |
| Similac Follow-On | Stage 2 | Reduced protein |
| Enfamil Follow-On A+ | Stage 2 | Higher iron |
| Aptamil 2 | Follow-on | With GOS/FOS prebiotics |
| Lactogen 2 | Stage 2 | India - budget friendly |
Stage 3 / Toddler (12–36 months)
| Brand | Note |
|---|---|
| Nan Pro 3 / Nan Supreme | Growth formula |
| Similac Gain / 3+ | Toddler milk |
| Enfagrow A+ | Brain development focus |
| Aptamil 3 | With immunity blend |
| Complan | Older toddlers, India |
| PediaSure | 2+ years, growth supplement |
Special/Medical Formula
| Brand | Indication |
|---|---|
| Pregestimil / Neocate | Protein allergy, malabsorption |
| Alimentum (Abbott) | Cow milk protein allergy (CMPA) |
| Nutramigen (Enfamil) | Extensively hydrolyzed, CMPA |
| EleCare / Neocate | Amino acid-based, severe allergy |
| Similac Preemie | Preterm / LBW infants |
| Enfamil Premature | Preterm - high calorie |
| Novalac AR | Anti-regurgitation |
| Isomil / Nan Soy | Lactose intolerance / galactosemia |
India-Specific Brands
| Brand | Company |
|---|---|
| Dexolac | Danone |
| Farex | Heinz/Zydus |
| Amulspray | Amul (cow milk based) |
| Nestogen | Nestlé |
| SMA Gold | Wyeth/Pfizer (some markets) |
Important Notes
WHO & IAP (Indian Academy of Pediatrics) position:
- Exclusive breastfeeding for the first 6 months is strongly recommended
- Formula is a medical substitute, not a first choice
- In India, IMS Act (1992) prohibits advertising of infant formula for 0–2 years
- Formula should only be used when breastfeeding is medically contraindicated or insufficient
Abdominal examination in pregnancy with images,
abdominal examination pregnancy inspection palpation auscultation clinical images obstetrics
Abdominal Examination in Pregnancy
Sources: Textbook of Family Medicine 9e (Rakel), Park's Textbook of Preventive and Social Medicine, Creasy & Resnik's Maternal-Fetal Medicine
Position & Preparation
- Patient lies in dorsal recumbent position (semi-recumbent, 15-30° tilt to avoid aortocaval compression after 20 weeks)
- Bladder should be emptied before examination
- Expose abdomen from xiphisternum to pubic symphysis
- Warm hands before palpation
I. INSPECTION
| Finding | Significance |
|---|---|
| Shape & size of uterus | Consistency with gestational age |
| Linea nigra | Dark vertical midline pigmentation - normal in pregnancy |
| Striae gravidarum | Stretch marks - pink/purple (new), silvery (old) |
| Umbilicus | Becomes flat/everted as pregnancy advances |
| Fetal movements | Visible rippling after ~28 weeks |
| Scars | Previous LSCS, laparotomy |
| Skin | Jaundice, spider angiomata |
| Shape | Transverse/longitudinal lie visible with large fetus |
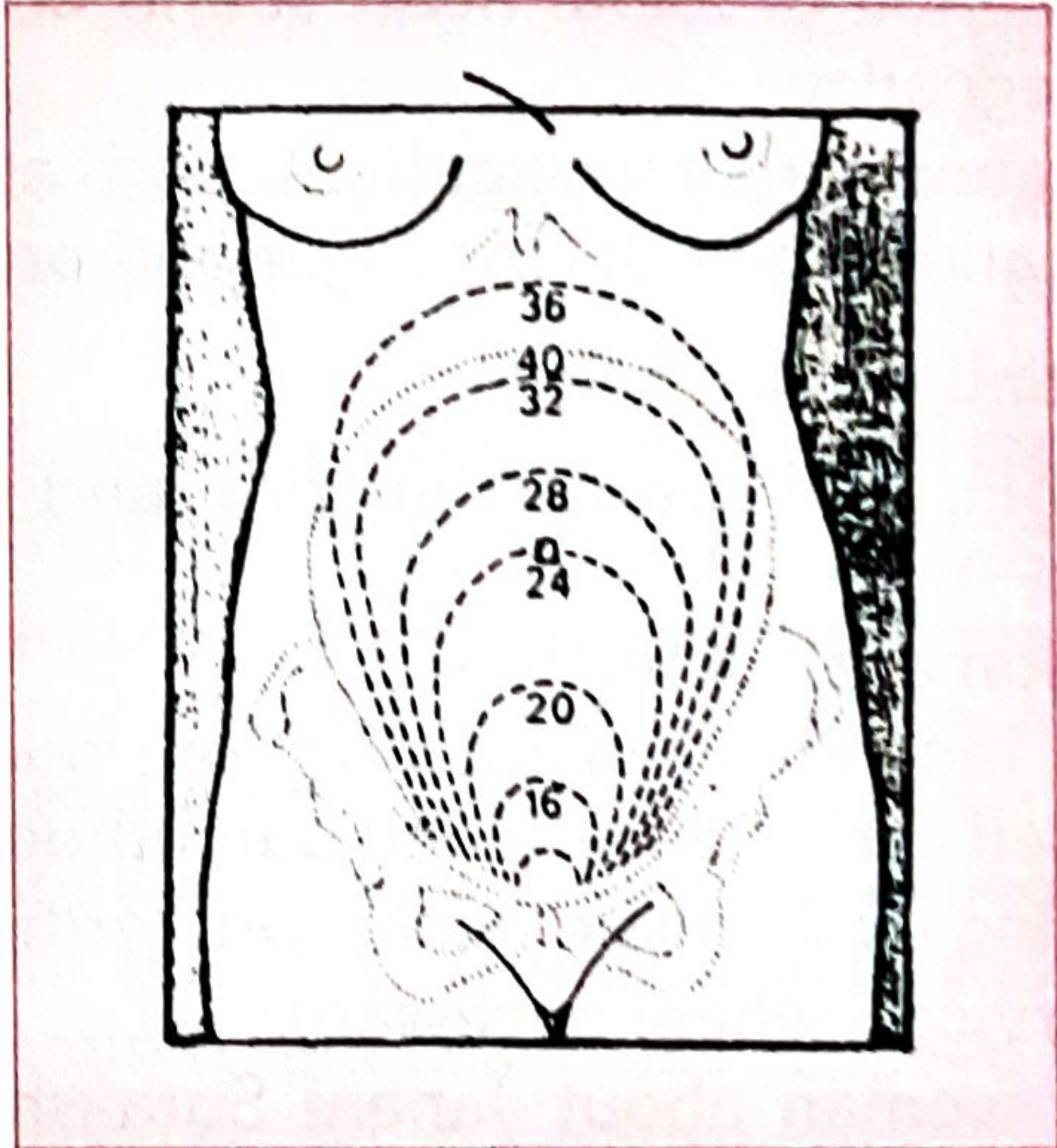
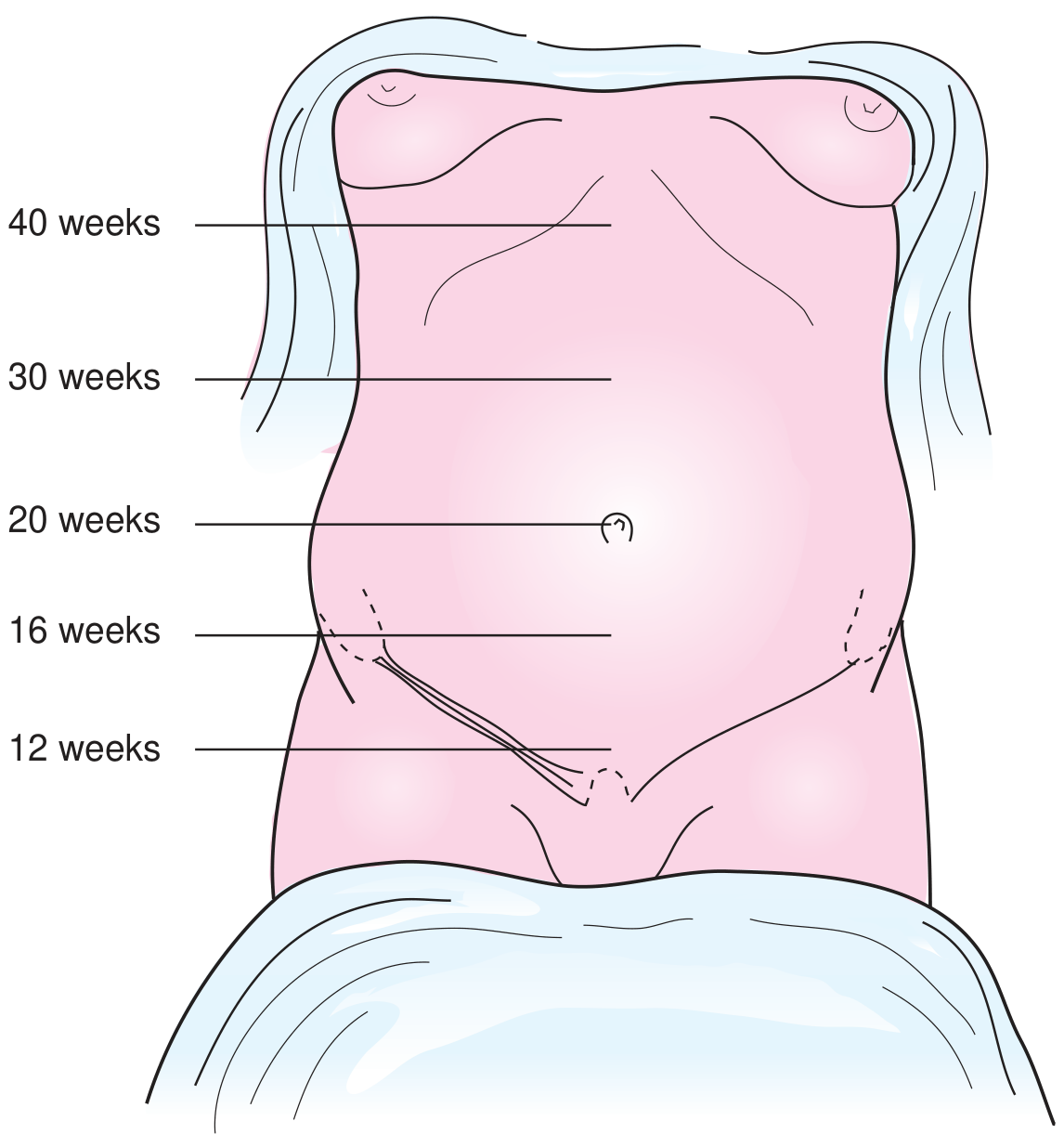
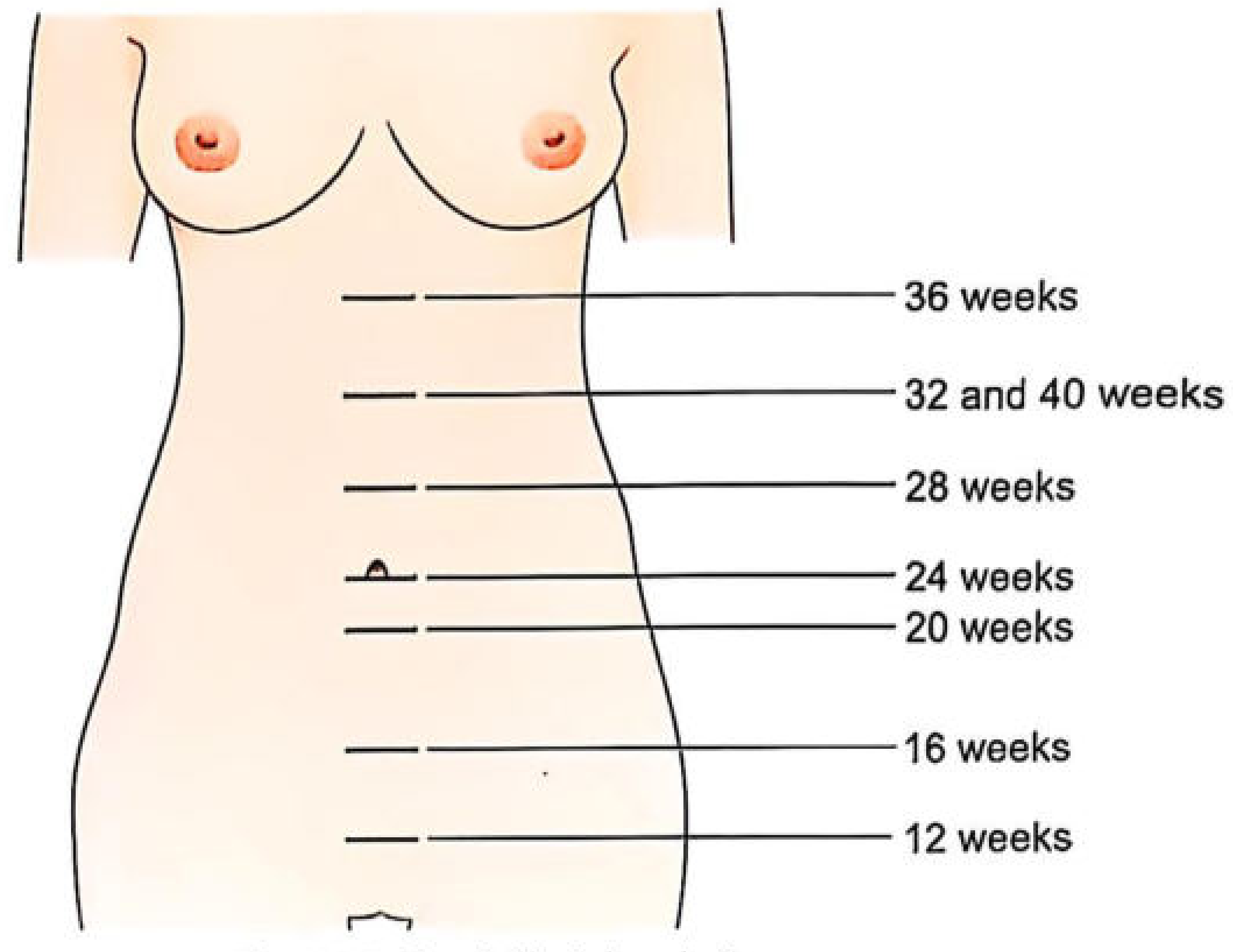
II. MEASUREMENT OF FUNDAL HEIGHT
Fundal Height at Various Gestational Ages:
| Weeks | Fundal Level |
|---|---|
| 12 weeks | Just palpable above pubic symphysis |
| 16 weeks | Between symphysis and umbilicus |
| 20 weeks | At the level of the umbilicus |
| 24 weeks | Midway between umbilicus and xiphisternum |
| 28 weeks | 3-4 fingers above umbilicus |
| 32 weeks | Midway between umbilicus and xiphisternum (upper) |
| 36 weeks | At the level of xiphisternum |
| 40 weeks | Drops slightly (lightening) - at 32-week level |
- Measure from upper border of pubic symphysis to the top of the uterine fundus with a tape measure
- SFH (cm) = gestational age in weeks ± 2 cm (after 20 weeks)
- Causes of large-for-dates: multiple gestation, polyhydramnios, macrosomia, fibroids, incorrect dates
- Causes of small-for-dates: IUGR, oligohydramnios, incorrect dates, fetal demise, transverse lie
III. PALPATION - Leopold's Maneuvers
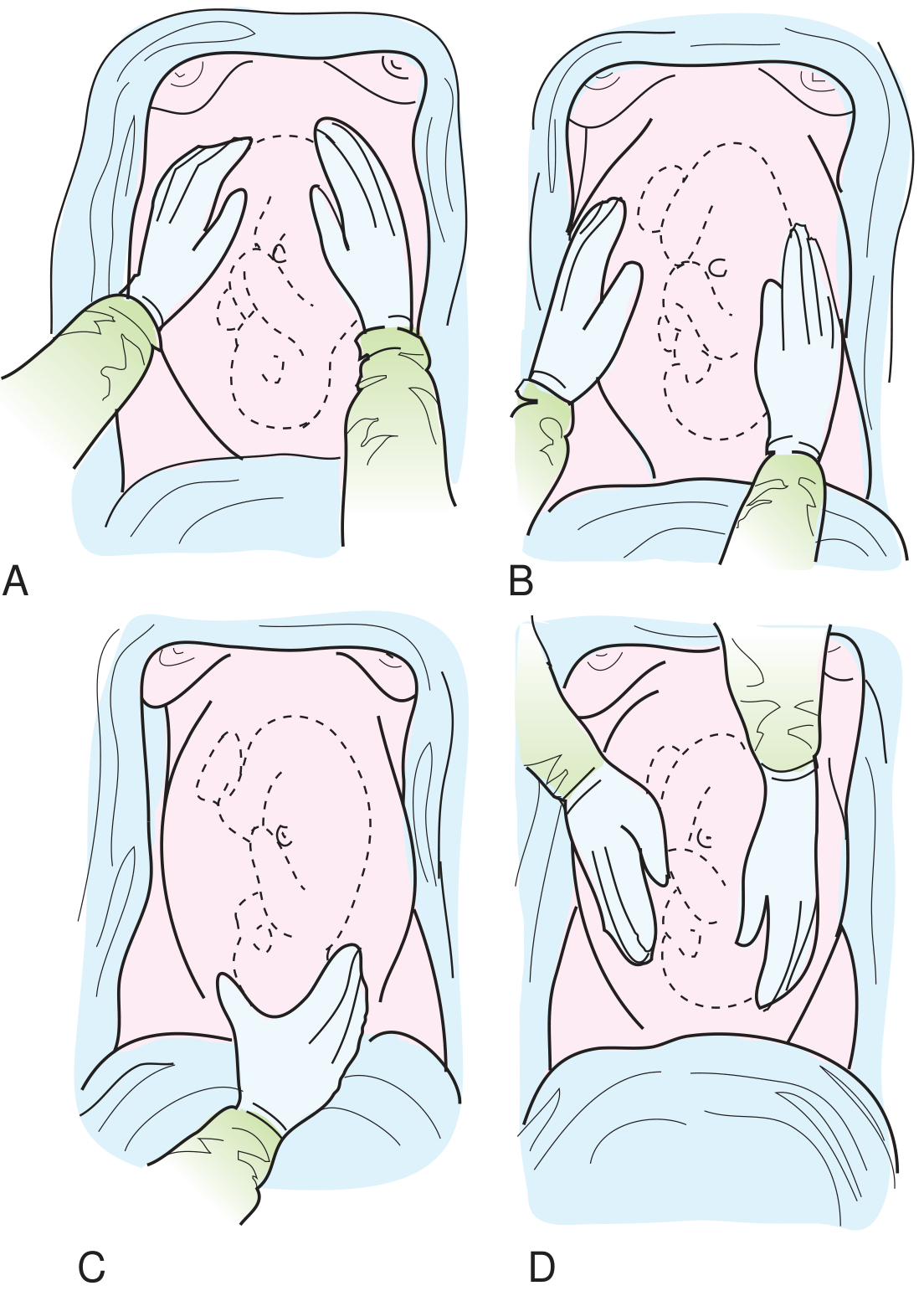
The 4 Leopold's Maneuvers:
- Face the patient's head
- Cup both hands around the fundus
- Feel which fetal pole is at the fundus
- Breech (buttocks) = soft, irregular, not ballottable
- Head = hard, round, ballottable
- Hands slide down laterally from fundus
- One hand stabilizes; other palpates the opposite side
- Back = smooth, firm, continuous resistance
- Limbs = irregular nodular, small parts
- Examiner faces patient's head
- Thumb and fingers of one hand grasp the presenting part just above the pubic symphysis
- Head = hard, round, ballottable (if not engaged)
- Buttocks = soft, irregular
- Examiner turns to face the patient's feet
- Both hands placed on the lower uterus, fingers pointing toward the pelvis
- Fingers walk down toward pelvic brim
- Cephalic prominence = the brow side (if on same side as back = deflexed/extended; if on opposite side = well-flexed, normal)
- Determines degree of descent into pelvis
IV. AUSCULTATION
Fetal Heart Sounds (FHS):
| Method | Audible from |
|---|---|
| Pinard fetoscope / Fetal stethoscope | 20-24 weeks |
| Sonicaid / Doppler | 10-12 weeks |
Where to Auscultate:
- FHS are heard best through the fetal back
- Cephalic presentation, LOA (Left Occiput Anterior): Left lower quadrant
- Cephalic presentation, ROA: Right lower quadrant
- Breech presentation: At or above the umbilicus
- After 28 weeks, location changes with fetal position
V. SPECIAL TESTS ON PALPATION
| Test | How Done | Finding |
|---|---|---|
| Ballottement | Tap lower pole of uterus with fingers | Free-floating head taps back = unengaged |
| Engagement | 4th maneuver - pawlik grip | Head not movable above brim = engaged (0/5 palpable) |
| Uterine tone | General palpation | Relaxed vs hypertonic (as in abruption) |
| Tenderness | Gentle palpation | Tenderness over fibroids, abruption, appendix |
VI. Summary of What Abdominal Exam Tells You
Inspection → Skin changes, shape, size, fetal movement, scars
Measurement → Gestational age, growth discrepancy
Palpation → Lie, presentation, position, engagement
Auscultation → FHR (rate, rhythm), fetal wellbeing
Quick Reference: Lie, Presentation, Position
| Term | Definition |
|---|---|
| Lie | Relationship of fetal long axis to uterine long axis (longitudinal/transverse/oblique) |
| Presentation | Part of fetus in the lower uterine segment (cephalic/breech/shoulder) |
| Position | Relationship of denominator to maternal pelvis (LOA, ROA, LOP, etc.) |
| Station | Level of presenting part relative to ischial spines (-3 to +3) |
| Engagement | Widest diameter of presenting part has passed the pelvic brim |
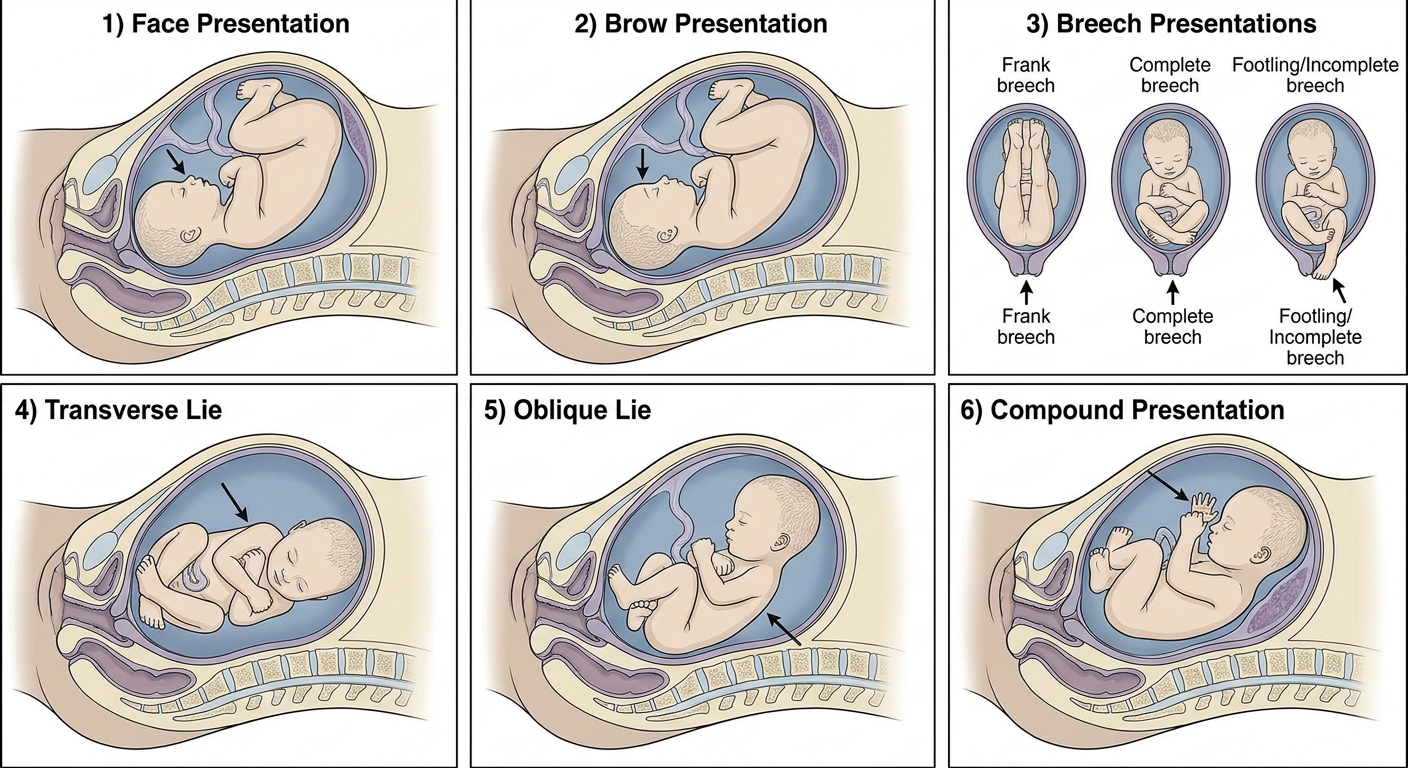
Generate clinical images/diagrams of abnormal fetal positions and presentations
Medical obstetrics educational diagram showing abnormal fetal presentations and positions in the uterus, clean clinical illustration style. Show 6 panels labeled: 1) Face Presentation - fetal head fully extended with face as presenting part, 2) Brow Presentation - partial head extension with brow presenting, 3) Breech Presentations - three types: Frank breech (legs extended upward), Complete breech (legs flexed), Footling/Incomplete breech (one or both feet presenting), 4) Transverse Lie - fetus lying horizontally across the uterus with shoulder presenting, 5) Oblique Lie - fetus at diagonal angle, 6) Compound Presentation - hand/arm prolapsed alongside the head. Each panel clearly labeled with the presentation name. Clean white background, anatomical cross-section view showing uterus outline, fetus in correct anatomical detail, arrows indicating presenting part, professional medical textbook style diagram.
Medical obstetrics educational diagram showing abnormal fetal HEAD positions and deflexion attitudes in cephalic presentation. Clean clinical cross-section illustrations showing the maternal pelvis and fetal head. Four panels: 1) Normal - Vertex presentation, well-flexed head, occiput presenting, chin on chest, 2) Sinciput/Military presentation - head in neutral position, neither flexed nor extended, 3) Brow presentation - head partially extended, brow is the presenting part, largest diameter presenting, 4) Face presentation - head fully hyperextended, face is the presenting part, mentum (chin) is the denominator. Each panel shows the maternal pelvis outline, cervix, and fetal head in anatomical detail with degree of extension indicated by curved arrow. Labels clearly show the presenting part and denominator. Professional medical textbook illustration, white background, labeled anatomy.
Medical obstetrics educational diagram showing types of breech presentation in the uterus. Clean anatomical cross-section illustrations, professional medical textbook style. Four labeled panels showing the full uterus outline with fetus inside: 1) Frank Breech - both hips flexed, both knees extended, legs pointing straight up alongside the body, buttocks presenting at pelvic inlet, most common breech type, 2) Complete Breech - both hips flexed, both knees also flexed, fetus in cross-legged sitting position, feet near buttocks, 3) Incomplete/Footling Breech - one or both feet are the lowermost part, foot presenting through cervix, 4) Knee Presentation - rare, one or both knees presenting first. Each panel clearly labeled with the type name and showing which part is at the cervix/pelvic inlet. White background, clean line art with color fill, anatomical accuracy.
Medical obstetrics educational diagram showing abnormal fetal LIE and compound presentations. Clean anatomical cross-section medical illustration, professional textbook style, white background. Three labeled panels: 1) Transverse Lie - fetus lying completely horizontal across the uterus, long axis of fetus perpendicular to long axis of mother, shoulder is the presenting part, acromion is the denominator, shoulder impacted at pelvic inlet shown from front view, 2) Oblique Lie - fetus lying at a 45-degree diagonal angle inside the uterus, neither longitudinal nor transverse, unstable lie, 3) Compound Presentation - vertex cephalic presentation with one arm/hand prolapsed alongside the fetal head into the pelvis, both head and hand visible at the pelvic inlet simultaneously. Each panel has clear anatomical labels: uterus wall, cervix, presenting part labeled with arrows, denomination noted. Color-coded anatomy, professional medical illustration.
Abnormal Fetal Presentations & Positions
1. Overview - All Major Abnormal Presentations
2. Deflexion Attitudes of the Head (Cephalic Malpresentations)
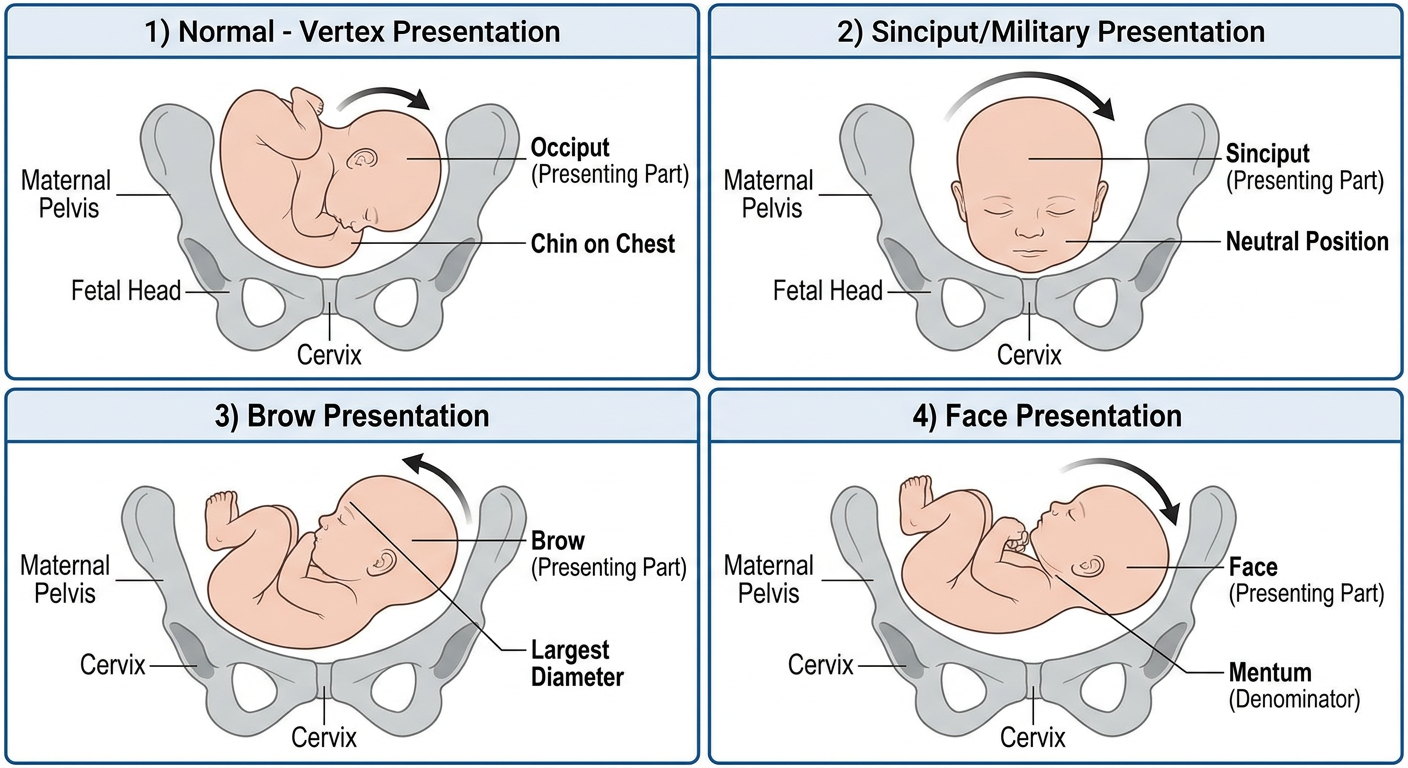
| Presentation | Degree of Extension | Presenting Diameter | Denominator |
|---|---|---|---|
| Vertex (normal) | Full flexion | Suboccipitobregmatic (9.5 cm) | Occiput |
| Sinciput/Military | Neutral | Occipitofrontal (11.5 cm) | Occiput |
| Brow | Partial extension | Mentovertical (13.5 cm) - largest | Frontal bone |
| Face | Full hyperextension | Submentobregmatic (9.5 cm) | Mentum (chin) |
Brow presentation has the largest presenting diameter - vaginal delivery impossible unless it converts.
3. Types of Breech Presentation
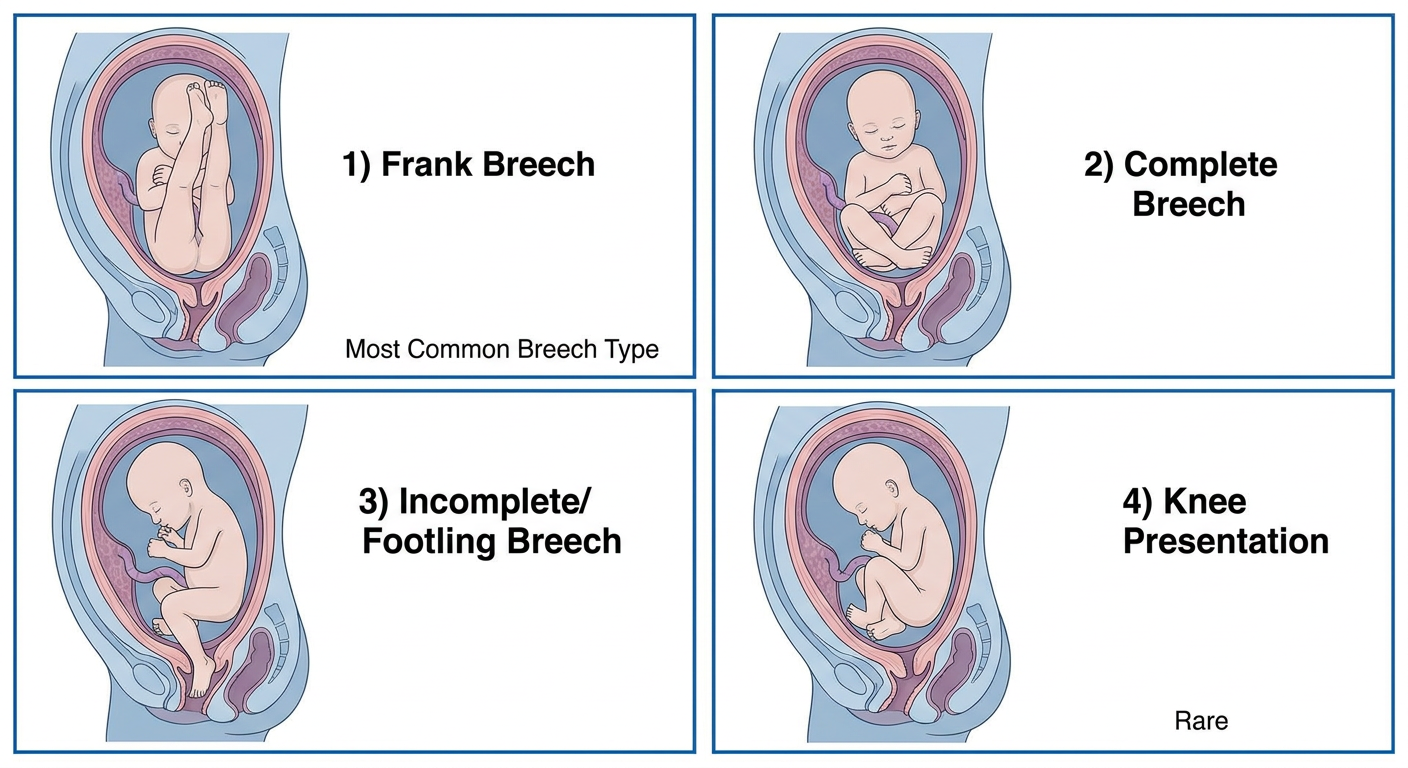
| Type | Description | Frequency | Notes |
|---|---|---|---|
| Frank Breech | Hips flexed, knees extended (pike position) | 65-70% | Most common; best for vaginal breech |
| Complete Breech | Hips flexed, knees flexed (cross-legged) | 5-10% | "Squatting" position |
| Footling/Incomplete | One or both feet presenting | 20-25% | High cord prolapse risk |
| Knee Presentation | Knees are the lowest part | Rare | Very high cord prolapse risk |
4. Transverse Lie, Oblique Lie & Compound Presentation
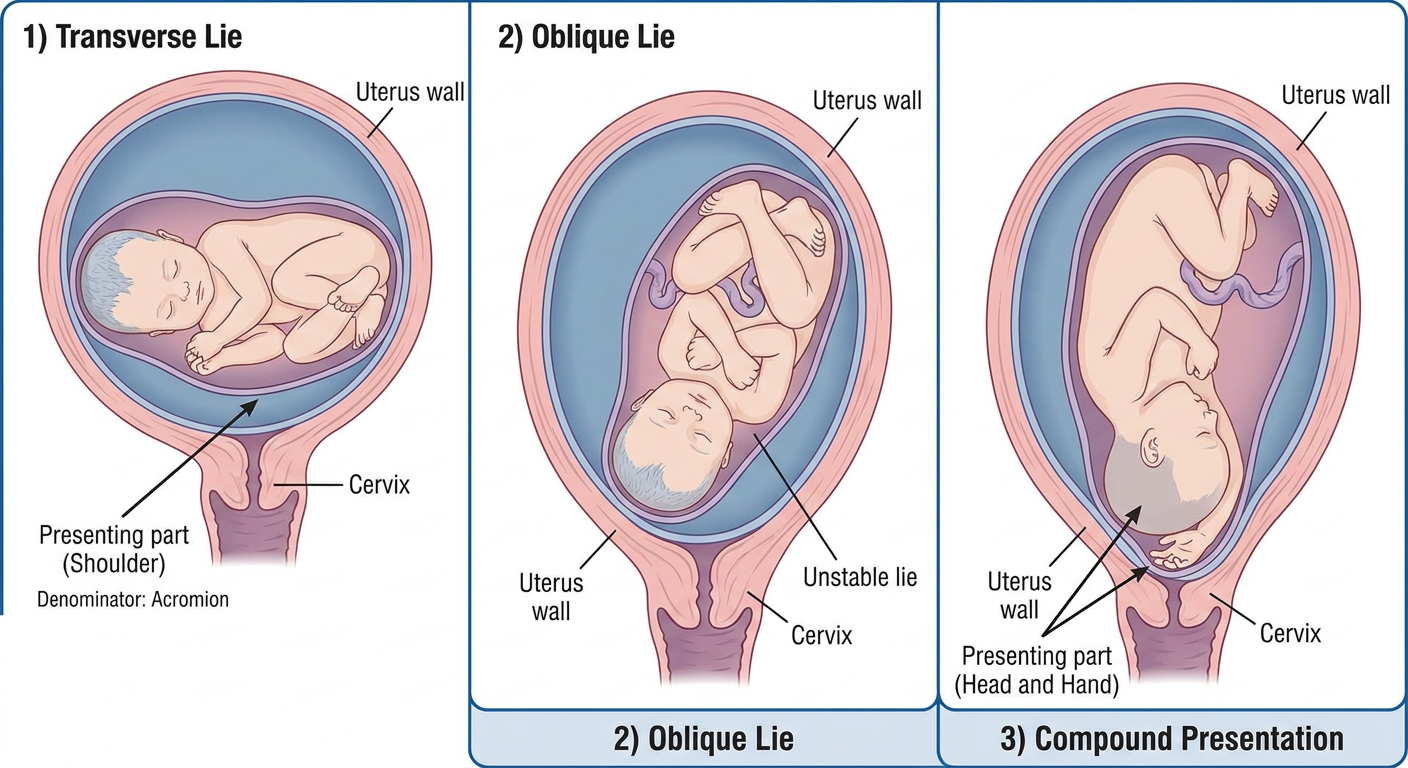
| Presentation | Denominator | Risk | Management |
|---|---|---|---|
| Transverse Lie | Acromion (shoulder) | Neglected shoulder dystocia, uterine rupture | Cesarean section |
| Oblique Lie | Unstable - may become transverse/longitudinal | Usually corrects in labor | Monitor; ECV if persists |
| Compound Presentation | Head + arm/hand | Cord prolapse, obstructed labor | Reposition limb; CS if needed |
Summary: Causes of Abnormal Presentation
Maternal factors: Uterine anomalies, fibroids, contracted pelvis,
multiparity (lax uterus), full bladder
Fetal factors: Prematurity, multiple pregnancy, macrosomia,
fetal anomalies (hydrocephalus, anencephaly),
short umbilical cord
Placental factors: Placenta previa, cornual placenta
Liquor: Polyhydramnios (unstable lie)
Oligohydramnios (restricted fetal movement)
study all the signs and symptoms and when it appears- of 1st -and 2 nd trimester Diagnosis of pregnancy . 2nd trimester-breast ,face and abdominal changes eg: Chloasma,linea nigra,Linea alba,stria gravidarum,internal and external ballotment,fundal height etc notes with images
Medical obstetrics educational diagram showing breast changes during pregnancy progression. Clean clinical illustration, white background, professional textbook style. Four panels showing the breast at different stages: 1) Non-pregnant breast - showing normal pink areola, no Montgomery tubercles, no pigmentation; 2) First Trimester (6-8 weeks) - slight breast enlargement, tingling, primary areola becoming darker, dilated veins (Haller's veins) visible under skin, nipple more erectile; 3) Second Trimester (12-16 weeks) - significant breast enlargement, secondary areola (areola of pregnancy), Montgomery tubercles visible as raised bumps around nipple, nipple dark brown, colostrum expressible, striae beginning; 4) Third Trimester (28+ weeks) - maximum enlargement, very dark nipple and areola, prominent Montgomery tubercles, striae gravidarum on breast, colostrum secretion. Each panel labeled with the trimester, weeks, and key features listed with arrows pointing to them. Professional anatomical illustration style.
Medical obstetrics educational diagram showing skin and face changes during pregnancy. Professional clinical illustration, white background. Four panels: 1) Chloasma (Melasma / Mask of Pregnancy) - front view of pregnant woman's face showing butterfly-shaped brown pigmentation patches on forehead, cheeks, bridge of nose, and upper lip; labeled "Chloasma gravidarum - appears 2nd trimester, due to MSH/estrogen"; 2) Linea Nigra - front view of pregnant abdomen showing dark pigmented vertical line running from pubis to umbilicus and above, with label showing it was previously the white Linea Alba; 3) Striae Gravidarum - close-up of pregnant abdomen showing pinkish-purple irregular stretch marks arranged concentrically around umbilicus, also on flanks; 4) Other pigmentation changes - showing hyperpigmented nipples and areola, axillary pigmentation, and spider angiomata. Each panel clearly labeled with timing of appearance and pathophysiology note. Medical textbook illustration style.
Medical obstetrics educational diagram showing internal and external ballottement technique during pregnancy examination. Clean clinical illustration, professional textbook style, white background. Two panels side by side: LEFT PANEL - Internal/Vaginal Ballottement (4th-5th month): Cross-section view showing gloved examiner's two fingers inserted into vaginal anterior fornix, giving a sharp upward tap; fetus shown floating up in amniotic fluid in uterus, then falling back down onto fingers like a bouncing ball; arrows showing the upward movement of fetus and downward rebound; label 'Positive at 16-20 weeks, when fetus small relative to liquor amnii'. RIGHT PANEL - External Ballottement: Front view showing examiner's hand on maternal abdomen giving a sharp inward tap on one side of uterus; fetus shown moving to opposite side and rebounding; sensation of floating object bouncing back felt on the same hand; labeled 'External ballottement - positive 4th to 5th month'. Both panels show anatomical detail with uterus wall, amniotic fluid, and fetus clearly depicted. Medical textbook illustration style.
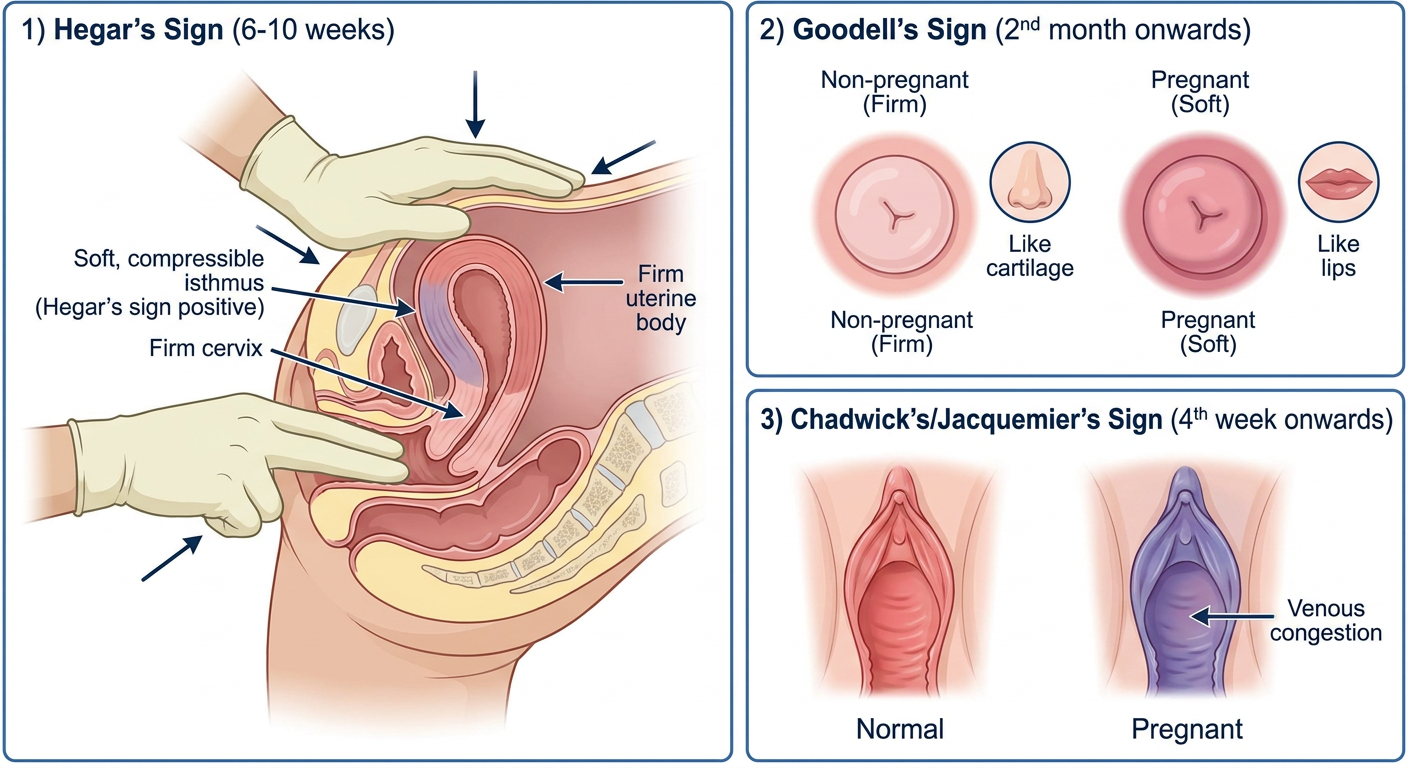
Medical obstetrics educational diagram showing Hegar's sign and other probable signs of pregnancy. Clean clinical cross-section illustrations, professional textbook style, white background. Three panels: 1) Hegar's Sign (6th week) - sagittal cross-section showing bimanual examination: two fingers in vagina reaching posterior fornix, other hand on abdomen over uterine fundus; middle segment showing the soft, compressible isthmus (lower uterine segment) between the hard cervix below and the firm uterine body above; labeled zones showing cervix (firm), isthmus (soft/compressible - Hegar's sign positive), uterine body (firm); arrows indicating the examiner's hands and the soft zone; note '6-10 weeks'; 2) Goodell's Sign - showing the softening of the cervix from normal firm (like cartilage) to soft (like lips) in pregnancy; comparison between non-pregnant firm cervix and pregnant soft cervix; labeled '2nd month onwards'; 3) Chadwick's/Jacquemier's Sign - vaginal view showing the color change of vaginal mucosa from normal pink/red to violaceous blue-purple due to venous congestion; labeled '4th week onwards'. Professional anatomical medical illustration.
Diagnosis of Pregnancy - Signs & Symptoms
Sources: The Essentials of Forensic Medicine & Toxicology 36e, Creasy & Resnik's Maternal-Fetal Medicine 8e, Park's Preventive & Social Medicine, Textbook of Family Medicine 9e
Classification of Signs of Pregnancy
| Group | Nature | Reliability |
|---|---|---|
| Presumptive | Subjective - felt by patient | Least reliable |
| Probable | Objective - detected by examiner | More reliable |
| Positive (Conclusive) | Definitive proof | Absolute proof |
PART I: PRESUMPTIVE SIGNS
1. Amenorrhea
- When: From the time of conception
- Earliest and most important symptom
- Menstruation may still occur for first 2-3 months (until decidua vera and reflexa fuse)
- Causes of false amenorrhea: Fear, stress, intense desire for pregnancy, hormonal disorders
2. Morning Sickness (Nausea & Vomiting)
- When: End of 1st month → disappears by 6-8 weeks later (6-14 weeks)
- Nausea + vomiting, typically in the morning, passes off in a few hours
- Due to rising hCG levels
- Not reliable as a sign alone
3. Breast Changes (Presumptive)
- When: From 6-8 weeks onward
- Sense of tenseness and tingling in breasts (early weeks)
- Breasts increase in size from 2nd month
- Nipples become more deeply pigmented and erectile
- Areola becomes dark brown (from pink in virgins)
- Montgomery's tubercles appear by end of 2nd month - small round dark sebaceous gland enlargements around nipple
- Colostrum expressible from 3rd month
- Striae on breasts appear after 6 months (especially in primipara)
4. Quickening
- When: 16-20 weeks
- First perception of fetal movements by the mother
- Described as "slight fluttering" that gradually increases
- Multigravida feel it earlier (~16 wks); primigravida later (~18-20 wks)
5. Pigmentation of Skin
- When: Progressively from 2nd trimester
- Vulva, abdomen, axillae become darker
- Linea nigra - dark line from pubis to beyond umbilicus
- Chloasma (Melasma/Mask of Pregnancy) - face pigmentation
6. Changes in the Vagina (Chadwick's/Jacquemier's Sign)
- When: From 4th week
- Vaginal mucosa changes from pink → violet → blue (venous congestion)
- Anterior vaginal wall flattened; mucus secretion increased
7. Urinary Disturbances (Frequency)
- When: Early weeks (uterus presses on bladder)
- Disappears as uterus rises into abdomen (3rd-4th month)
- Reappears near term (head descends into pelvis)
8. Other Presumptive Signs
| Sign | Timing |
|---|---|
| Fatigue / easy tiredness | 1st trimester |
| Salivation (ptyalism) | 1st trimester |
| Perverted appetite (pica) | 1st trimester |
| Irritability/emotional changes | Throughout |
PART II: PROBABLE SIGNS
1. Enlargement of Abdomen
- When: Visible after 12th week (uterus palpable per abdomen)
| Week | Fundal Level |
|---|---|
| 12 weeks | Just palpable above pubic symphysis |
| 16 weeks | Midway between symphysis and umbilicus |
| 20 weeks | At level of umbilicus |
| 24 weeks | 2-3 fingers above umbilicus |
| 28 weeks | 3-4 fingers above umbilicus |
| 32 weeks | Midway between umbilicus and xiphisternum |
| 36 weeks | Level of xiphisternum |
| 40 weeks | Drops back to ~32-week level (lightening) |
2. Hegar's Sign
- When: ~6th week (positive 6-10 weeks)
- Most valuable physical sign of early pregnancy
- Bimanual examination: two fingers in vagina (posterior fornix), other hand on abdomen
- The isthmus (lower uterine segment) feels soft and compressible between the firm cervix below and firm uterine body above
- Due to softening of the isthmus with decidual change and increased vascularity
3. Goodell's Sign
- When: From 2nd month (well marked by 4th month)
- Progressive softening of the cervix from below upward
- Normal cervix feels like the tip of the nose (cartilaginous)
- Pregnant cervix feels like the lips (soft)
- Due to increased vascularity and edema of cervical stroma
4. Chadwick's / Jacquemier's Sign
- When: From 4th week
- Bluish-violet discoloration of the vagina and cervix
- Due to increased vascularity and venous engorgement
5. Braxton Hicks Contractions
- When: Difficult before 3rd month; easily felt after 4th month
- Intermittent, irregular, painless uterine contractions
- Each contraction lasts ~1 minute, relaxation 2-3 minutes
- Present even when fetus is dead (differentiates from fetal movement)
- Due to stretching of uterine muscle
6. Ballottement
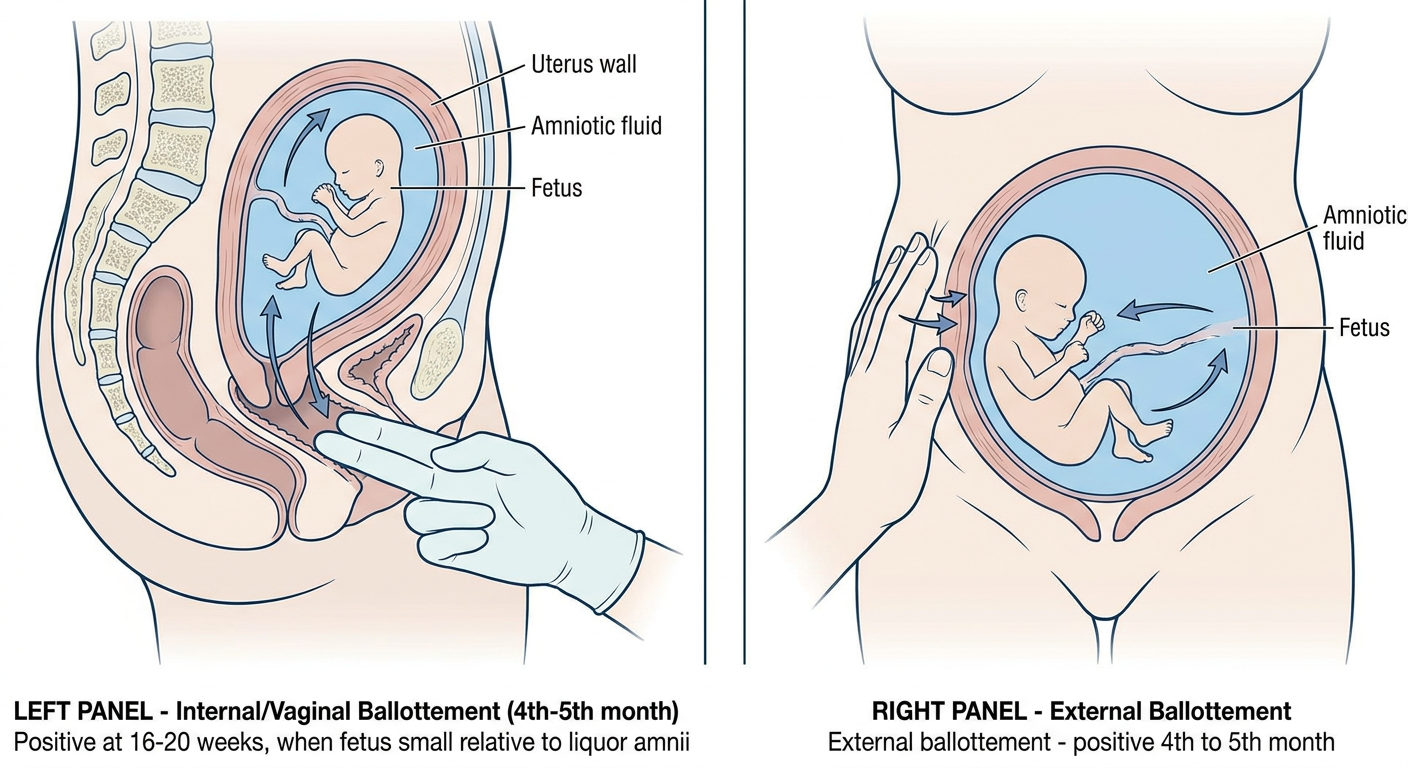
- When: 4th-5th month (16-20 weeks) - when fetus is small relative to liquor amnii
- Two fingers inserted into the anterior fornix
- Sudden upward motion given - fetus moves up in liquor amnii
- After a moment, fetus falls back down onto fingers like a bouncing ball
- Sharp tap given on abdominal wall over the uterus
- In a few seconds, rebound of the fetus felt on the same hand
- Negative if amniotic fluid is scanty (oligohydramnios)
7. Hegar's, Goodell's & Chadwick's - Illustrated
8. Uterine Souffle
- When: End of 4th month
- Soft blowing murmur heard on auscultation just above inguinal ligament
- Synchronous with mother's pulse (not fetal)
- Due to increased blood flow through uterine vessels
9. Pregnancy Tests (hCG)
- Urine/Blood hCG - detectable in blood from 8th day after implantation
- Rises rapidly, peaks at 7th week after conception
- Immunological tests (latex slide test): Positive 12-15 days after implantation
- Accuracy ~98%
- Also positive in: hydatidiform mole, choriocarcinoma, ectopic pregnancy
PART III: POSITIVE (CONCLUSIVE) SIGNS
| Sign | When Detectable |
|---|---|
| Fetal Heart Sounds (Doppler) | From 10-12 weeks |
| Fetal Heart Sounds (Fetoscope/Pinard) | 20-24 weeks |
| Fetal Movements (felt by examiner) | 18-22 weeks |
| Fetal Parts palpable | ~22 weeks |
| Fetal skeleton on X-ray | After 14-16 weeks (not used routinely) |
| Ultrasound - Gestational sac | 4-5 weeks |
| Ultrasound - Fetal pole + heartbeat | 6-7 weeks |
PART IV: 2ND TRIMESTER - BODY CHANGES WITH IMAGES
A. BREAST CHANGES
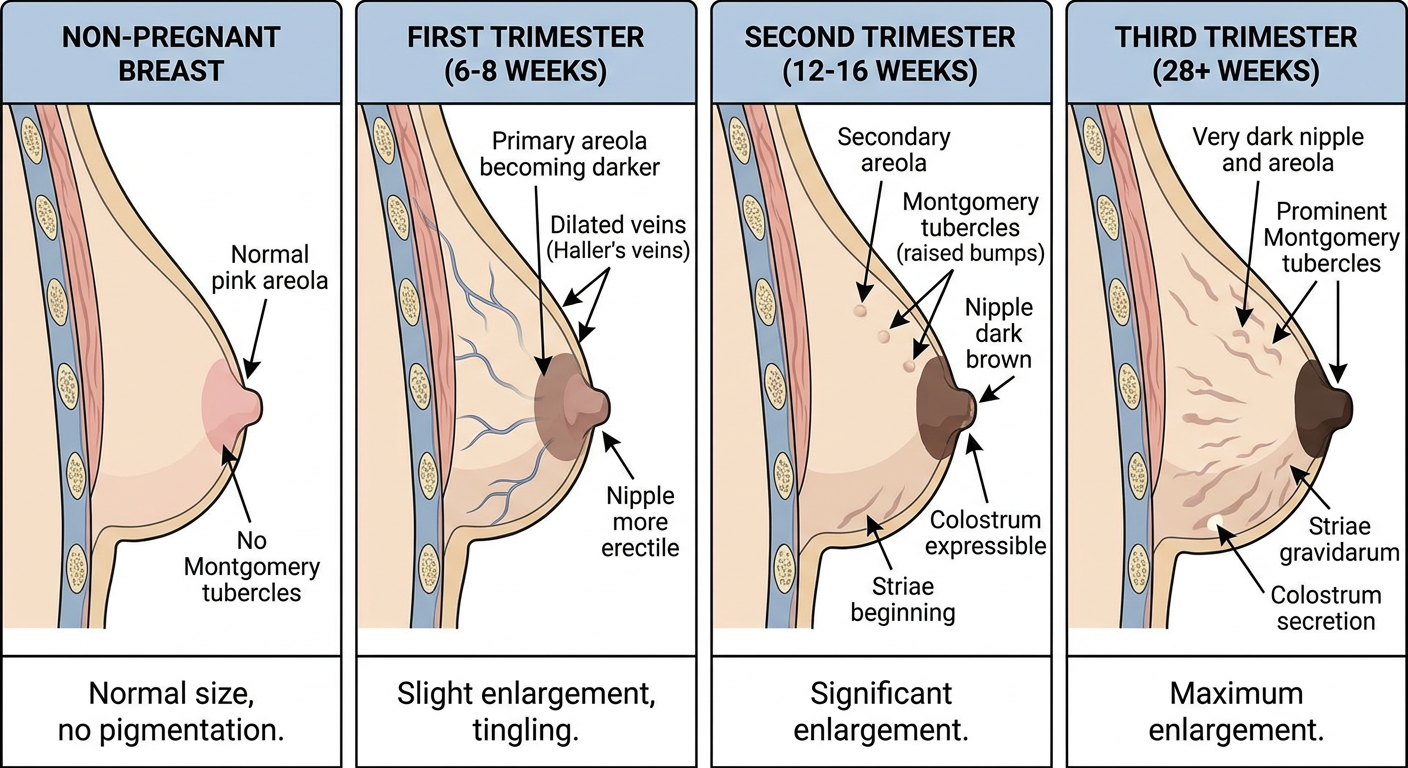
| Change | Timing | Notes |
|---|---|---|
| Tingling/tenseness | 6-8 weeks | Due to progesterone |
| Size increase, nodular | 2nd month | Mammary alveoli hypertrophy |
| Dilated veins (Haller's veins) | 2nd month | Due to increased blood flow |
| Nipple pigmentation, erectile | 2nd month | Due to MSH, estrogen |
| Areola darkens (primary areola) | 2nd month | From pink → dark brown |
| Montgomery's tubercles | End of 2nd month | Hypertrophied sebaceous glands |
| Secondary areola | 3rd-4th month | Mottled, less defined outer ring |
| Colostrum expressible | From 3rd month | Thin, yellowish, fat-rich fluid |
| Striae on breasts | After 6 months | Especially primipara |
B. FACE CHANGES - CHLOASMA
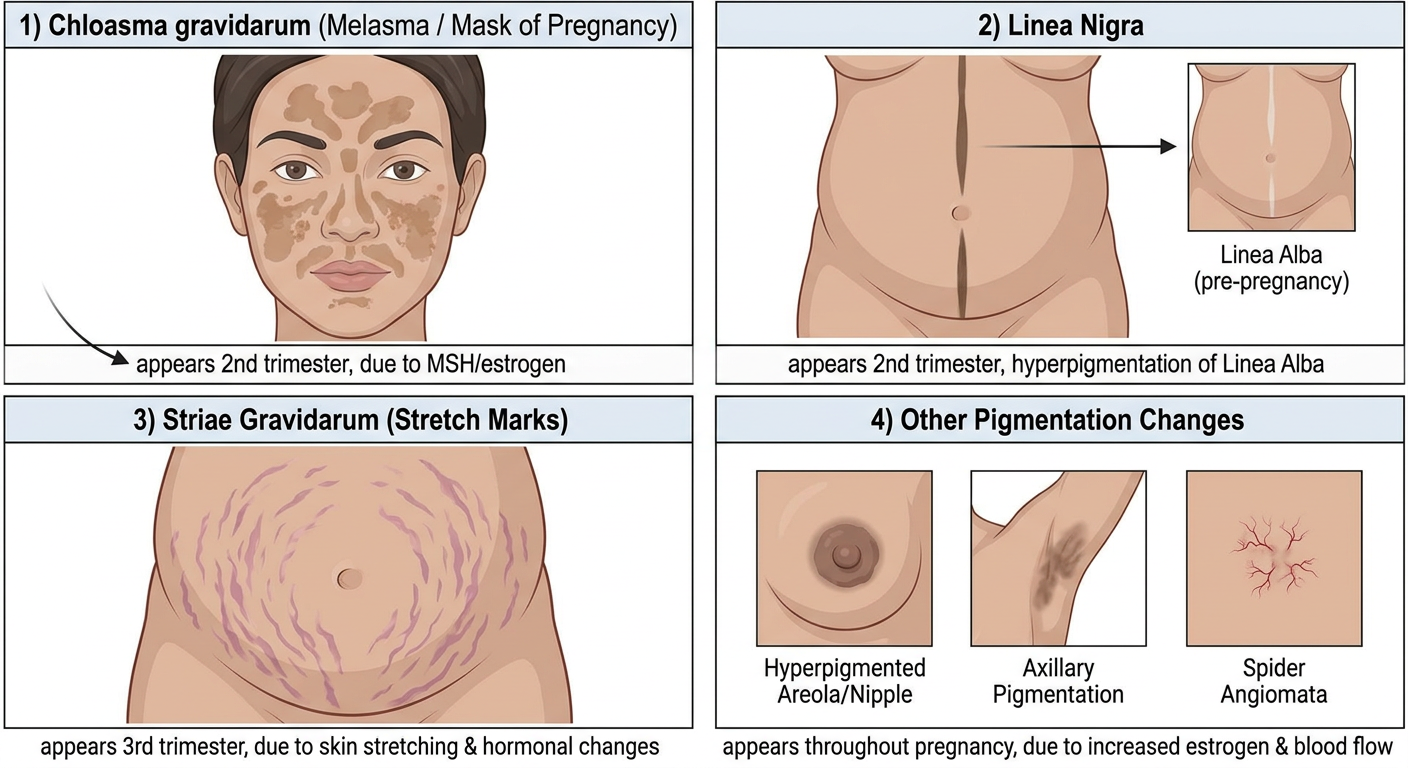
Chloasma Gravidarum (Melasma / Mask of Pregnancy)
- When: 2nd trimester onwards (after ~16 weeks)
- Appearance: Diffuse macular brown hyperpigmentation of face - forehead, cheeks, nose bridge, upper lip (butterfly distribution)
- Cause: Elevated MSH (Melanocyte Stimulating Hormone), estrogen, progesterone stimulating melanocytes
- 70% of pregnant women affected
- Worsened by sun exposure
- Usually regresses after delivery
- Treatment if persists: Topical hydroquinone, sunscreen (SPF ≥15), tretinoin, azelaic acid
C. ABDOMINAL CHANGES
1. Linea Nigra
- When: 2nd trimester (after 12-14 weeks)
- Dark pigmented vertical line running from pubis to umbilicus (and sometimes above)
- It is the Linea Alba (a white/pale midline raphe in non-pregnant) that becomes darkly pigmented
- Due to: Elevated MSH and estrogen → melanocyte stimulation
- Occurs in >90% of pregnant women
- Usually regresses after delivery
Memory: Linea Alba (white) → becomes Linea Nigra (black) in pregnancy
2. Striae Gravidarum (Stretch Marks)
- When: Usually begin in 2nd-3rd trimester (6th-7th month), sometimes from 1st trimester
- Appearance: Pinkish-purple, curved, irregular, depressed bands
- Arranged concentrically/radially around umbilicus
- Also on breasts, thighs, buttocks, groin, axillae
- Cause: Linear tears in dermal connective tissue (rupture of subcuticular elastic fibers) due to abdominal distension + hormonal effects
- Occur in 50-80% of pregnancies; severe in ~10%
- After delivery: Color fades → become white/silvery scars called Lineae Albicantes (Lineae Albigantes)
- Risk factors: Young age, family history, higher weight gain, large baby, non-White race
- No proven topical treatment prevents or reverses them
3. Umbilical Changes
| Week | Umbilicus |
|---|---|
| Normal | Depressed/inverted |
| 24 weeks | Begins to flatten |
| 28 weeks (7th month) | Level with skin |
| 32-36 weeks | Everted/protruding |
4. Fundal Height (Abdominal measurement)
- SFH (cm) = gestational age in weeks ± 2 cm (from 20 weeks onward)
- Measured from upper border of pubic symphysis to top of fundus
Quick Summary Table
| Sign | Type | Trimester | Timing (Weeks) |
|---|---|---|---|
| Amenorrhea | Presumptive | 1st | From 4 weeks |
| Morning sickness | Presumptive | 1st | 4-14 weeks |
| Breast tingling/size | Presumptive | 1st | 6-8 weeks |
| Chadwick's/Jacquemier's | Presumptive/Probable | 1st | 4-6 weeks |
| Montgomery's tubercles | Presumptive | 1st | 8 weeks |
| Hegar's sign | Probable | 1st | 6-10 weeks |
| Goodell's sign | Probable | 1st | 8-10 weeks |
| Positive hCG test | Probable | 1st | 12-15 days post-implantation |
| USG - gestational sac | Positive | 1st | 4-5 weeks |
| USG - fetal heartbeat | Positive | 1st | 6-7 weeks |
| Quickening | Presumptive | 2nd | 16-20 weeks |
| Linea nigra | Presumptive | 2nd | 12-16 weeks |
| Chloasma | Presumptive | 2nd | 16 weeks |
| Ballottement | Probable | 2nd | 16-20 weeks |
| Braxton Hicks | Probable | 2nd | After 16 weeks |
| Striae gravidarum | Presumptive | 2nd-3rd | 24-28 weeks |
| FHS (Doppler) | Positive | 2nd | 10-12 weeks |
| FHS (Pinard) | Positive | 2nd | 20-24 weeks |
| Fetal parts palpable | Positive | 2nd | 22-24 weeks |
Hinguvacahadi gutika
Shloka, ingredients, indications
Hinguvachadi gutika shloka ingredients indications Ayurveda classical reference
Hinguvachadi gutika Kashyapa Samhita Ashtanga Hridayam shloka composition reference
https://ayurmedinfo.com/2019/10/21/hinguvachaadi-gulika
Hinguvachadi gutika Sahasrayogam shloka Sanskrit text ingredients Hingu Vacha
हिंगुवचादि गुटिका / Hinguvachadi Gutika
Classical Reference
Ashtanga Hridayam - Chikitsa Sthana, Gulmaroga Adhyaya (Chapter 14), Shlokas 31-33 Also mentioned in Sahasrayogam (same ingredients)
Shloka (Sanskrit - Devanagari)
हिंगुवचावजयापशुगन्धा- दाडिमदीप्यकधान्यकपाठाः। पुष्करमूलशठीपुषागग्नि- क्षारयुगत्रिपटुत्रिकटूनि॥ ३१॥
साजाग्जचव्यं सिनिविीकं सवेतसाम्लं वनिग्नि चूर्णमम।
Hingu-Vacha-Vajaya-Pashugandha - Dadima-Dipyaka-Dhanyaka-Pathah | Pushkara-mula-Shathi-Hapusha-Agni - Kshara-yuga-Tripathu-Trikatu-ni ||31||
Sa-Ajaji-Chavyam-Sinivali-kam Sa-Veta-Samlam-Vanhi-agni-churnam ||
Ingredients (24 in Total)
| No. | Sanskrit Name | Botanical Name | Common Name | Primary Action |
|---|---|---|---|---|
| 1 | Hingu (Shuddha) | Ferula asafoetida | Asafoetida | Chief ingredient - Deepana, Pachana, Vatanulomana, Carminative |
| 2 | Vacha | Acorus calamus | Sweet flag | Deepana, Pachana, relieves Adhmana |
| 3 | Vijaya / Haritaki | Terminalia chebula | Chebulic Myrobalan | Anulomana, digestive, laxative |
| 4 | Pashugandha / Ajagandha | Cleome viscosa / gynandra | Wild mustard | Deepana, Krimighna |
| 5 | Dadima (dry) | Punica granatum | Pomegranate (dry seeds) | Grahi, Rochana, appetizer |
| 6 | Dipyaka / Yavani | Trachyspermum ammi | Carom seeds / Ajwain | Shulahara, Krimighna, Pachana |
| 7 | Dhanyaka | Coriandrum sativum | Coriander | Deepana, Trishnanigrahana |
| 8 | Patha | Cyclea peltata | Paatha | Krimighna, Pachana |
| 9 | Pushkara-mula | Inula racemosa | Pushkarmool | Kasa-Shwasa-Shulahara |
| 10 | Shati / Shatpushpa | Hedychium spicatum | Spiked ginger lily | Shulahara, Deepana |
| 11 | Hapusha | Juniperus communis | Juniper berry | Shulahara, Pachana, Deepana |
| 12 | Agni / Chitraka | Plumbago zeylanica | Leadwort | Deepana, Pachana, Krimighna |
| 13 | Yava Kshara | Hordeum vulgare (alkali) | Barley alkali | Vatanulomana, Mutrala |
| 14 | Svarjika Kshara | Sodium bicarbonate / natural alkali | Sajji kshara | Vatanulomana, digestive |
| 15 | Saindhava Lavana | Rock salt | Sendha namak | Deepana, Vatanulomana |
| 16 | Sauvarchala Lavana | Sochal salt | Bit loona | Deepana, Rochana |
| 17 | Vida Lavana | Bida salt | Black salt variety | Vatanulomana, carminative |
| 18 | Shunti | Zingiber officinale | Dry ginger | Deepana, Pachana, Shulahara |
| 19 | Maricha | Piper nigrum | Black pepper | Deepana, Pachana, Krimighna |
| 20 | Pippali | Piper longum | Long pepper | Deepana, Rasayana |
| 21 | Ajaji | Cuminum cyminum | Cumin | Shulahara, Deepana, Grahi |
| 22 | Chavya | Piper chaba / retrofractum | Cubeb pepper | Deepana, Krimighna, Shulahara |
| 23 | Tintidika | Rhus parviflora | Tintidi | Deepana, Amlapachana |
| 24 | Veta-Samla / Vetasa-amla | Garcinia morella | Wild mangosteen / Tintali | Shulahara, Anulomana |
Trikatu = Shunti + Maricha + Pippali (Nos. 18, 19, 20) Tripatu = Same as Trikatu in some references Kshara yuga = Two Ksharas (Yava + Svarjika) Three Lavanas = Saindhava + Sauvarchala + Vida
Pharmacological Properties (Rasapanchaka)
| Property | Quality |
|---|---|
| Rasa | Predominantly Katu (pungent), Amla, Lavana |
| Guna | Laghu (light), Tikshna (sharp), Ruksha (dry) |
| Virya | Ushna (hot potency) |
| Vipaka | Katu |
| Dosha Karma | Vata-Kapha shamana (pacifies Vata and Kapha); may aggravate Pitta |
Indications (Rogadhikara)
Primary Indications:
| Ayurvedic Term | Clinical Meaning |
|---|---|
| Gulma | Abdominal tumor/phantom tumor, gaseous distension |
| Adhmana | Flatulence, bloating, tympanitis |
| Shula | Colic pain (abdominal) |
| Anaha | Obstruction of flatus, constipation with distension |
| Vibandha | Constipation |
| Parshva Shula | Flank/lateral chest pain |
| Basthi Shula | Groin / bladder pain |
| Trika Shula | Sacral pain |
| Yoni Shula | Dysmenorrhea / uterine/vaginal pain |
| Pandu | Anaemia / initial liver disorders |
| Krimi Roga | Worm infestation |
| Mutra Krichra | Dysuria |
| Hridroga | Cardiac disorders |
| Hikka | Hiccup |
| Shwasa / Kasa | Respiratory disorders |
| Agnimandya / Agnisada | Digestive weakness / low Agni |
| Pleeharoga | Splenic disorders |
| Arshas | Hemorrhoids / piles |
| Stana / Kukshi Roga | Breast and abdominal disorders |
Dosage & Anupana
| Parameter | Details |
|---|---|
| As Gutika (tablet) | 1-2 tablets (500 mg - 1 g) twice daily |
| As Churna (powder) | 1-3 grams once or twice a day |
| Time of administration | Before or after food |
| Anupana (vehicle) | Warm water, buttermilk (Takra), or as directed |
| Duration | 2-3 months (as per physician advice) |
Method of Preparation (Gutika)
- All 24 ingredients are taken in equal parts and made into fine powder (churna)
- Hingu is first purified (Shuddha Hingu) - fried in ghee (Ghrita-bhavita)
- All powders are mixed uniformly
- Pills are formed using appropriate binding agents
- Dried and stored in cool, dry place
Important Notes
- This formulation is primarily for Vata-Kapha disorders of the gastro-intestinal tract
- The three salts (Tri-lavana) and two ksharas make it highly effective in Vata-avrita conditions
- Trikatu (three peppers) + Chitraka + Hingu form the powerful Deepana-Pachana core
- Caution in Pitta-predominant conditions (hyperacidity, gastritis) - may aggravate
- Pregnancy - use only under physician guidance
- Also mentioned as Hinguvachadi Vati in some references (same formula, pill form)
Reference Summary
| Reference | Chapter | Verse |
|---|---|---|
| Ashtanga Hridayam | Chikitsa Sthana, Gulmaroga Adhyaya | 14/31-33 |
| Sahasrayogam | Gutika Prakarana | Same ingredients mentioned |
Each ingredient indications
Hinguvachadi Gutika - Individual Drug Indications
1. 🔸 Hingu (Shuddha) - Ferula asafoetida
| Property | Detail |
|---|---|
| Rasa | Katu (pungent) |
| Guna | Laghu, Snigdha, Tikshna |
| Virya | Ushna |
| Vipaka | Katu |
| Dosha | Vata-Kapha shamana |
- Adhmana - flatulence, gaseous distension (CHIEF drug)
- Shula - abdominal colic
- Anaha - obstruction of flatus
- Gulma - abdominal phantom tumor
- Krimi - intestinal worm infestation
- Agnimandya - digestive weakness
- Hikka - hiccup
- Shwasa - asthma, dyspnoea
- Kasa - cough
- Arshas - hemorrhoids
- Rajarodha - amenorrhea (emmenagogue)
- Netrya - eye diseases (used as Anjana)
- Visharoga - toxic conditions
- Unmada / Apasmara - psychiatric/epileptic conditions (Nasya, Dhumapana)
"Hingu deepanam pachnam vatanulomanam shulaharam" - restores normal Vata movement
2. 🔸 Vacha - Acorus calamus
| Property | Detail |
|---|---|
| Rasa | Katu, Tikta |
| Guna | Laghu, Tikshna |
| Virya | Ushna |
| Vipaka | Katu |
| Dosha | Kapha-Vata shamana |
- Adhmana - bloating, abdominal distension
- Vibandha - constipation
- Agnimandya - low digestive fire
- Vak-shuddhi - speech disorders, stammering
- Manovikara - mental disorders, Unmada
- Apasmara - epilepsy
- Buddhi-vriddhi - memory and intellect enhancement (Medhya)
- Kasa, Shwasa - cough, respiratory diseases
- Krimi - worm infestation
- Jwara - fever
- Vrana - wound healing (external)
- Karna-roga - ear diseases (oil preparation)
- Visharoga - antidote/detoxifying
3. 🔸 Vijaya / Haritaki - Terminalia chebula
| Property | Detail |
|---|---|
| Rasa | Pancharasa (all 5 except Lavana) |
| Guna | Laghu, Ruksha |
| Virya | Ushna |
| Vipaka | Madhura |
| Dosha | Tridosha shamana |
- Vibandha - constipation (mild laxative)
- Arshas - piles/hemorrhoids
- Gulma - abdominal growths
- Pandu - anemia, jaundice
- Kushtha - skin diseases
- Prameha - diabetes mellitus
- Kasa, Hikka, Shwasa - respiratory diseases
- Netraroga - eye diseases (Triphala eye wash)
- Hridroga - cardiac conditions
- Rasayana - anti-aging, immune boosting
- Mutrala - diuretic
- Shothahara - anti-inflammatory
- Vrana-ropana - wound healing
4. 🔸 Pashugandha / Ajagandha - Cleome viscosa / gynandra
| Property | Detail |
|---|---|
| Rasa | Katu, Tikta |
| Guna | Laghu, Tikshna, Ruksha |
| Virya | Ushna |
| Vipaka | Katu |
| Dosha | Vata-Kapha shamana |
- Krimi - worm infestation (Krimighna - primary use)
- Adhmana - flatulence
- Shula - abdominal colic
- Jwara - fever
- Kushtha - skin diseases
- Vrana - wound healing (external)
- Karna-roga - ear disorders (juice used)
- Agnimandya - poor digestion
- Shotha - edema, swelling
5. 🔸 Dadima - Punica granatum (dry seeds)
| Property | Detail |
|---|---|
| Rasa | Madhura, Amla, Kashaya |
| Guna | Laghu, Snigdha |
| Virya | Anushna |
| Vipaka | Madhura |
| Dosha | Tridosha shamana |
- Agnimandya - digestive weakness (appetizer - Rochana)
- Atisara - diarrhea (Grahi, astringent)
- Grahani - malabsorption / IBS
- Hikka - hiccup
- Raktapitta - bleeding disorders
- Trishna - excessive thirst
- Hridroga - cardiac conditions
- Mukharoga - oral disorders (gargle)
- Krimi - worm infestation
- Arshas - hemorrhoids
- Shwasa, Kasa - respiratory
- Mutrakrichra - dysuria
- Jwara - fever (cooling in Pitta jwara)
6. 🔸 Dipyaka / Yavani - Trachyspermum ammi
| Property | Detail |
|---|---|
| Rasa | Katu, Tikta |
| Guna | Laghu, Tikshna, Ruksha |
| Virya | Ushna |
| Vipaka | Katu |
| Dosha | Vata-Kapha shamana |
- Shula - abdominal colic (primary use - Shulahara)
- Adhmana - flatulence (strong carminative)
- Krimi - worm infestation (Krimighna)
- Agnimandya - digestive weakness
- Atisara - diarrhea
- Grahani - IBS/malabsorption
- Hikka - hiccup
- Shwasa, Kasa - respiratory disorders
- Arshas - piles
- Mutrakrichra - dysuria
- Shothahara - anti-edema
- Hridroga - cardiac disorders
- Stanya-janana - galactagogue (mild)
7. 🔸 Dhanyaka - Coriandrum sativum
| Property | Detail |
|---|---|
| Rasa | Katu, Tikta, Madhura |
| Guna | Laghu, Snigdha |
| Virya | Ushna (seed); Sheeta (fresh leaf) |
| Vipaka | Madhura |
| Dosha | Tridosha shamana |
- Trishnanigrahana - relieves excessive thirst
- Adhmana - bloating, distension
- Agnimandya - digestive weakness
- Jwara - fever (especially Pitta-jwara)
- Atisara - diarrhea
- Mutrakrichra - urinary disorders (Mutrala)
- Raktapitta - bleeding disorders
- Netraroga - eye diseases
- Shwasa, Hikka - respiratory
- Vamana - nausea/vomiting (antiemetic)
- Kushtha - skin disorders
8. 🔸 Patha - Cyclea peltata
| Property | Detail |
|---|---|
| Rasa | Tikta, Katu |
| Guna | Laghu, Tikshna, Ruksha |
| Virya | Ushna |
| Vipaka | Katu |
| Dosha | Kapha-Vata shamana |
- Krimi - worm infestation (Krimighna - primary)
- Jwara - fever (anti-pyretic)
- Atisara - diarrhea
- Agnimandya - poor digestion
- Kushtha - skin diseases
- Shotha - edema
- Visha - toxic conditions (anti-toxic)
- Pandu - anemia
- Raktapitta - bleeding disorders
- Gulma - abdominal growths
9. 🔸 Pushkaramula - Inula racemosa
| Property | Detail |
|---|---|
| Rasa | Katu, Tikta |
| Guna | Laghu, Ruksha, Tikshna |
| Virya | Ushna |
| Vipaka | Katu |
| Dosha | Kapha-Vata shamana |
- Kasa - cough (best Kasahara herb per Ashtanga Hridayam)
- Shwasa - asthma, dyspnoea
- Hikka - hiccup
- Parshva-shula - pleuritic/flank pain (primary indication)
- Hridroga - cardiac disorders
- Shotha - edema
- Jwara - fever
- Vatavyadhi - Vata diseases
- Agnimandya - digestive weakness
- Kushtha - skin conditions
"Parshvashule Pushkaramulam" - famous for flank/chest pain
10. 🔸 Shati - Hedychium spicatum
| Property | Detail |
|---|---|
| Rasa | Katu, Tikta |
| Guna | Laghu, Tikshna |
| Virya | Ushna |
| Vipaka | Katu |
| Dosha | Kapha-Vata shamana |
- Shula - colic, abdominal pain
- Adhmana - flatulence
- Agnimandya - digestive weakness
- Kasa, Shwasa - cough, asthma
- Hikka - hiccup
- Jwara - fever
- Vamana - nausea/vomiting
- Krimi - worms
- Arshas - hemorrhoids
- Shotha - edema
11. 🔸 Hapusha - Juniperus communis
| Property | Detail |
|---|---|
| Rasa | Katu, Tikta, Kashaya |
| Guna | Laghu, Ruksha, Tikshna |
| Virya | Ushna |
| Vipaka | Katu |
| Dosha | Kapha-Vata shamana |
- Shula - pain (Vedanahara)
- Shotha - localized swelling, edema
- Agnimandya - indigestion
- Shiroroga - headache
- Kasa, Shwasa - cough, asthma
- Galaganda - goiter, neck swelling
- Shlipadha - elephantiasis
- Kushtha - skin diseases
- Vatavyadhi - Vata disorders
- Vrushya - aphrodisiac (improves vigor)
- Mutrala - diuretic
12. 🔸 Agni / Chitraka - Plumbago zeylanica
| Property | Detail |
|---|---|
| Rasa | Katu |
| Guna | Laghu, Tikshna, Ruksha |
| Virya | Ushna (most Ushna among Deepaniya herbs) |
| Vipaka | Katu |
| Dosha | Kapha-Vata shamana |
- Agnimandya - chief Deepana herb (ignites Agni strongly)
- Gulma - abdominal tumor
- Shula - colic
- Adhmana - flatulence
- Arshas - piles/hemorrhoids
- Grahani - IBS/sprue
- Krimi - worm infestation
- Shotha - edema
- Medoroga - obesity, dyslipidemia
- Kushtha - skin diseases
- Vata-Kapha jwara - fever
- Vishama jwara - malarial fever
One of the most potent Deepaniya (digestive fire-kindling) drugs in Ayurveda
13. 🔸 Yava Kshara - Hordeum vulgare (alkali)
| Property | Detail |
|---|---|
| Rasa | Katu, Lavana |
| Guna | Tikshna, Laghu, Ruksha |
| Virya | Ushna |
| Dosha | Kapha-Vata shamana |
- Mutrakrichra - urinary difficulty (diuretic)
- Ashmari - urinary calculi (breaks stones)
- Gulma - abdominal growths
- Medoroga - obesity
- Vatanulomana - corrects Vata movement
- Shotha - edema
- Arshas - hemorrhoids
- Hikka, Shwasa - respiratory disorders
14. 🔸 Svarjika Kshara
| Property | Detail |
|---|---|
| Rasa | Katu, Lavana |
| Guna | Tikshna, Laghu |
| Virya | Ushna |
| Dosha | Kapha-Vata shamana |
- Anaha - obstruction of flatus, constipation (Vatanulomana)
- Adhmana - flatulence
- Gulma - abdominal growths
- Agnimandya - poor digestion
- Ashmari - urinary calculi
- Arshas - hemorrhoids
- Shotha - edema
- Visarpa - herpes/spreading skin conditions
15. 🔸 Saindhava Lavana
| Property | Detail |
|---|---|
| Rasa | Lavana |
| Guna | Sukshma, Snigdha, Laghu |
| Virya | Sheeta (cooling) |
| Vipaka | Madhura |
| Dosha | Tridosha shamana (best among salts) |
- Agnimandya - improves digestion and taste (Ruchya, Deepana)
- Vibandha - constipation
- Vatanulomana - regulates Vata movement
- Hridroga - cardiac disorders
- Netraroga - eye diseases (Anjana)
- Arochaka - anorexia
- Shotha - edema
- Krimi - worm infestation
Best of all salts - "Saindhavam Lavanottamam"
16. 🔸 Sauvarchala Lavana
| Property | Detail |
|---|---|
| Rasa | Lavana, Katu |
| Guna | Laghu, Tikshna |
| Virya | Ushna |
| Dosha | Vata-Kapha shamana |
- Agnimandya - digestive weakness (Rochana, Deepana)
- Adhmana - flatulence
- Shula - colic
- Vibandha - constipation
- Arshas - piles
- Netraroga - eye disorders
- Hikka - hiccup
17. 🔸 Vida Lavana
| Property | Detail |
|---|---|
| Rasa | Lavana, Katu, Amla |
| Guna | Laghu, Tikshna, Sukshma |
| Virya | Ushna |
| Dosha | Vata-Kapha shamana |
- Vatanulomana - corrects Vata movement (primary action)
- Vibandha - constipation
- Adhmana - flatulence
- Shula - colic
- Agnimandya - digestive weakness
- Arshas - hemorrhoids
18. 🔸 Shunti - Zingiber officinale
| Property | Detail |
|---|---|
| Rasa | Katu |
| Guna | Laghu, Snigdha, Tikshna |
| Virya | Ushna |
| Vipaka | Madhura |
| Dosha | Vata-Kapha shamana |
- Agnimandya - digestive weakness (best Deepana)
- Shula - colic
- Adhmana - flatulence
- Vamana / Hikka - nausea, hiccup
- Shwasa, Kasa - asthma, cough
- Shothahara - anti-inflammatory
- Ama-pachana - digests Ama (metabolic toxins)
- Jwara - fever
- Hridroga - cardiac conditions
- Vatavyadhi - Vata disorders (arthritis)
- Mutrakrichra - urinary disorders
19. 🔸 Maricha - Piper nigrum
| Property | Detail |
|---|---|
| Rasa | Katu |
| Guna | Laghu, Tikshna, Sukshma |
| Virya | Ushna |
| Vipaka | Katu |
| Dosha | Kapha-Vata shamana |
- Agnimandya - digestive fire kindler
- Krimi - worm infestation
- Shwasa, Kasa - respiratory disorders
- Jwara - fever
- Shotha - anti-inflammatory
- Kushtha - skin diseases
- Netraroga - eye conditions (Anjana preparation)
- Visha - antidote (anti-toxic)
- Prameha - diabetes
- Arsha - piles
20. 🔸 Pippali - Piper longum
| Property | Detail |
|---|---|
| Rasa | Katu |
| Guna | Laghu, Snigdha, Tikshna |
| Virya | Anushna-Sheeta (paradoxical - mildly cooling) |
| Vipaka | Madhura |
| Dosha | Vata-Kapha shamana |
- Agnimandya - digestive weakness (Deepana-Pachana)
- Shwasa - asthma (one of best)
- Kasa - cough
- Hikka - hiccup
- Gulma - abdominal growths
- Shula - colic
- Arshas - hemorrhoids
- Pandu - anemia/jaundice
- Jwara - fever
- Rasayana - anti-aging, rejuvenation
- Vrushya - aphrodisiac
- Netraroga - eye diseases
- Shotha - edema
21. 🔸 Ajaji - Cuminum cyminum
| Property | Detail |
|---|---|
| Rasa | Katu, Tikta |
| Guna | Laghu, Ruksha, Tikshna |
| Virya | Ushna |
| Vipaka | Katu |
| Dosha | Kapha-Vata shamana |
- Shula - abdominal colic (Shulahara)
- Adhmana - flatulence, bloating
- Atisara - diarrhea (Grahi)
- Grahani - IBS/malabsorption
- Agnimandya - digestive weakness
- Arshas - piles
- Mutrakrichra - urinary disorders
- Jwara - fever
- Vamana - nausea (antiemetic)
- Stanya-shodhana - purifies breast milk
22. 🔸 Chavya - Piper chaba / retrofractum
| Property | Detail |
|---|---|
| Rasa | Katu |
| Guna | Laghu, Tikshna, Ruksha |
| Virya | Ushna |
| Vipaka | Katu |
| Dosha | Kapha-Vata shamana |
- Krimi - worm infestation (Krimighna - primary)
- Vibandha - constipation
- Shula - abdominal pain
- Adhmana - flatulence
- Arshas - piles
- Grahani - malabsorption
- Mutrakrichra - urinary disorders
- Kasa, Shwasa - respiratory disorders
- Pandu - anemia
- Shotha - edema
23. 🔸 Tintidika - Rhus parviflora
| Property | Detail |
|---|---|
| Rasa | Amla |
| Guna | Laghu, Ruksha |
| Virya | Ushna |
| Vipaka | Amla |
| Dosha | Vata-Kapha shamana |
- Agnimandya - digestive weakness (Deepana)
- Arochaka - anorexia (Rochana)
- Adhmana - flatulence
- Shula - colic
- Arshas - hemorrhoids
- Atisara - diarrhea (mildly Grahi)
- Hikka, Vamana - hiccup, vomiting
24. 🔸 Vetasa-amla / Tintali - Garcinia morella / Tamarindus indica
| Property | Detail |
|---|---|
| Rasa | Amla |
| Guna | Guru, Snigdha |
| Virya | Ushna |
| Vipaka | Amla |
| Dosha | Vata-Kapha shamana |
- Vibandha - constipation (laxative)
- Shula - colic pain
- Adhmana - flatulence
- Agnimandya - poor digestion
- Arshas - hemorrhoids
- Atisara - diarrhea (paradoxically used in small doses)
- Anulomana - promotes downward movement of Vata
- Hridroga - cardiac conditions
- Trishna - thirst
Summary: Drug Group-wise Actions
| Group | Drugs | Primary Action |
|---|---|---|
| Chief Deepana-Pachana | Hingu, Chitraka, Shunti, Pippali, Maricha | Kindles digestive fire |
| Krimighna | Vacha, Pashugandha, Dipyaka, Patha, Chavya, Maricha | Anti-worm |
| Shulahara | Hingu, Dipyaka, Shunti, Ajaji, Shati, Hapusha, Pushkamula | Relieves colic |
| Vatanulomana | Vida Lavana, Kshara-yuga, Hingu, Vacha | Regulates Vata |
| Anulomana | Haritaki, Vetasamla, Lavana-traya | Laxative/carminative |
| Kasa-Shwasa-Hara | Pushkaramula, Pippali, Shunti, Maricha | Respiratory |
| Deepana | Saindhava, Sauvarchala, Dadima, Tintidika | Appetizer |
| Kshara-dravya | Yava kshara, Svarjika kshara | Alkalizing, stone-dissolving |
Milk formula brand India report with images